Two Pathways of Bone Formation | Membranous vs Cartilage Template | Development
Ossification Types
Critical Must-Knows
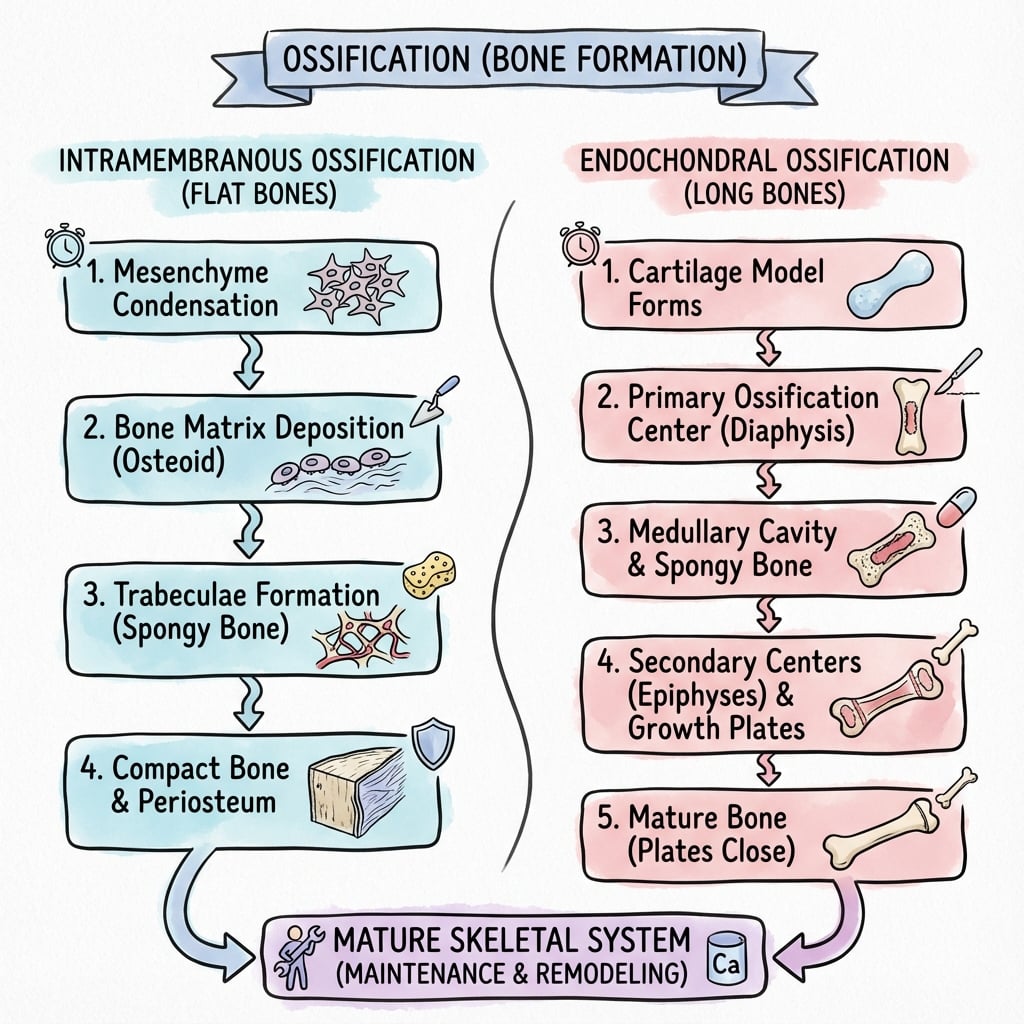
- Intramembranous: bone forms directly from mesenchymal condensation (no cartilage intermediate)
- Endochondral: bone forms by replacing cartilage template through coordinated chondrocyte maturation
- Flat bones (skull, clavicle, mandible) form via intramembranous ossification
- Long bones form via endochondral ossification with growth plates for longitudinal growth
- Both pathways produce lamellar bone; woven bone is emergency/pathologic
Clinical Pearls
- "Clavicle is unique: intramembranous ossification but medial physis for growth
- "Growth plate zones: Reserve, Proliferative, Hypertrophic, Ossification
- "Salter-Harris fractures exploit growth plate zone weakness
- "Distraction osteogenesis uses intramembranous ossification
Critical Ossification Exam Points
Two Pathways
Fundamentally different. Intramembranous = direct mesenchyme to bone. Endochondral = mesenchyme to cartilage to bone. Same end product (lamellar bone).
Anatomical Distribution
Location determines pathway. Flat bones (skull, clavicle) = intramembranous. Long bones, vertebrae, pelvis = endochondral. Rib cage mixed.
Growth Plate Zones
RZPHO sequence. Reserve → Proliferative → Hypertrophic (maturation, calcification) → Ossification. Injury pattern basis for Salter-Harris classification.
Clinical Applications
Fracture healing uses both. Primary (intramembranous) direct bone formation. Secondary (endochondral) via cartilage callus. Distraction osteogenesis is intramembranous.
At a Glance
Bone formation occurs through two fundamentally different pathways that produce the same final product—lamellar bone. Intramembranous ossification involves direct transformation of mesenchymal condensations into bone without a cartilage intermediate, forming flat bones (skull vault, clavicle, facial bones, mandible). Endochondral ossification proceeds through a hyaline cartilage template that is progressively replaced by bone, forming long bones and axial skeleton with growth plates enabling longitudinal growth. The growth plate demonstrates organized zones: Reserve → Proliferative → Hypertrophic → Ossification (RZPHO), with the hypertrophic zone's weakness explaining Salter-Harris fracture patterns. The clavicle is unique: it forms via intramembranous ossification yet possesses a medial physis for growth. Clinically, distraction osteogenesis utilizes intramembranous ossification, while secondary fracture healing proceeds through an endochondral callus.
RZPHOGrowth Plate Zones (Endochondral)
| R | Reserve (Resting) Stem cell reservoir, sparse chondrocytes |
| Z | Zone of proliferation Rapid cell division, columnar stacks |
| P | Prehypertrophic Cell enlargement begins |
| H | Hypertrophic Large cells, matrix calcification |
| O | Ossification Chondrocyte apoptosis, vascular invasion, bone deposition |
| R | Reserve (Resting) Stem cell reservoir, sparse chondrocytes | H | Hypertrophic Large cells, matrix calcification |
| Z | Zone of proliferation Rapid cell division, columnar stacks | O | Ossification Chondrocyte apoptosis, vascular invasion, bone deposition |
| P | Prehypertrophic Cell enlargement begins |
Hook:RZPHO: Real Zebras Produce Huge Offspring - the sequential zones of endochondral bone growth!
SCFMIntramembranous Bones
| S | Skull vault Frontal, parietal, temporal, occipital |
| C | Clavicle Only long bone that is intramembranous |
| F | Facial bones Maxilla, zygomatic, nasal |
| M | Mandible Jaw bone |
| S | Skull vault Frontal, parietal, temporal, occipital | F | Facial bones Maxilla, zygomatic, nasal |
| C | Clavicle Only long bone that is intramembranous | M | Mandible Jaw bone |
Hook:SCFM: Skull, Clavicle, Face, Mandible form directly without cartilage!
Overview and Development
Ossification is the process of bone formation. There are two distinct pathways by which bone develops and heals:
Intramembranous Ossification:
- Bone forms directly from mesenchymal stem cells without a cartilage intermediate
- Occurs in flat bones: skull, facial bones, mandible, clavicle
- Also used in primary fracture healing and distraction osteogenesis
Endochondral Ossification:
- Bone forms by replacing a cartilage template
- Occurs in long bones, vertebrae, pelvis, and most of the skeleton
- Growth plates are persistent endochondral ossification zones
- Also used in secondary fracture healing
Both Pathways Produce Same Bone
Despite fundamentally different mechanisms, both intramembranous and endochondral ossification produce identical lamellar bone. The pathway is determined by anatomical location and mechanical environment, not by final bone type.
Mechanisms: Intramembranous
Direct Bone Formation Pathway
Intramembranous ossification forms bone directly from mesenchymal tissue WITHOUT a cartilage intermediate. This is the embryonic pathway for flat bones (skull vault, facial bones, mandible, clavicle) and also the mechanism of fracture healing via primary union and distraction osteogenesis.
Intramembranous Ossification Steps
Mesenchymal stem cells aggregate at ossification center, forming condensed tissue with increased cell density and vascularity.
MSCs differentiate into osteoblasts under influence of Runx2 and Osterix transcription factors. Cells secrete osteoid (unmineralized matrix).
Osteoblasts deposit collagen type I and non-collagenous proteins forming osteoid matrix. This occurs along radiating spicules from ossification center.
Hydroxyapatite deposition within osteoid after 10-day lag phase. Some osteoblasts become embedded as osteocytes. Trabeculae form.
Initial woven bone (disorganized collagen) is gradually replaced by organized lamellar bone through remodeling.
Periosteum forms at surface. Appositional growth creates cortical bone. Trabecular spaces become marrow cavities.
Bones Formed Intramembranously
- Skull: Frontal, parietal, occipital, temporal (flat parts)
- Face: Maxilla, zygomatic, nasal
- Jaw: Mandible
- Shoulder: Clavicle (unique: has medial physis!)
Key Characteristics
- No cartilage intermediate
- Direct vascular invasion
- Multiple ossification centers coalesce
- Rapid bone formation
- Used in distraction osteogenesis
Endochondral Ossification
Cartilage Template Pathway
Endochondral ossification forms bone by REPLACING a cartilage template. This is the pathway for most of the skeleton (long bones, vertebrae, pelvis, ribs) and the mechanism of secondary fracture healing via cartilaginous callus. The growth plate is an endochondral ossification zone that persists until skeletal maturity.
Endochondral Ossification Steps
Mesenchymal cells condense and differentiate into chondrocytes, forming hyaline cartilage model of future bone. Shape matches final bone.
Central chondrocytes enlarge (hypertrophy), matrix calcifies. Hypertrophic cells secrete VEGF, attracting blood vessels.
Vascular invasion at mid-diaphysis. Chondrocytes undergo apoptosis. Osteoblasts arrive and deposit bone on calcified cartilage scaffold. Occurs week 8 fetal development.
Intramembranous bone forms around mid-shaft via periosteum, providing structural support during cartilage replacement.
Epiphyseal ossification centers develop (birth to adolescence). Same process: vascular invasion, chondrocyte apoptosis, bone deposition.
Cartilage persists between diaphysis and epiphysis as growth plate. Endochondral ossification continues here until skeletal maturity, driving longitudinal growth.
Estrogen-mediated closure at skeletal maturity. Cartilage fully replaced by bone, forming epiphyseal line scar.
Growth Plate Structure and Function
Five Functional Zones
| Zone | Cell Characteristics | Matrix | Function |
|---|---|---|---|
| Reserve/Resting | Sparse, small chondrocytes | High proteoglycan | Stem cell niche |
| Proliferative | Columnar stacks, flat cells | Type II collagen | Rapid cell division |
| Prehypertrophic | Cells begin enlarging | Transition matrix | Maturation initiation |
| Hypertrophic | Large cells (10x volume) | Type X collagen, calcified | Matrix mineralization |
| Ossification | Chondrocyte apoptosis | Calcified cartilage scaffold | Vascular invasion, bone deposition |
Hypertrophic Zone Is Mechanically Weakest
The hypertrophic zone is the weakest point in the growth plate due to large cells with minimal matrix. This is where Salter-Harris fractures propagate. Zone of Ranvier (peripheral fibrous ring) provides lateral support and circumferential growth.
Comparison of Ossification Pathways
Intramembranous vs Endochondral
| Feature | Intramembranous | Endochondral |
|---|---|---|
| Intermediate | None (direct) | Cartilage template |
| Location | Flat bones, clavicle | Long bones, axial skeleton |
| Vascularization | Early, throughout | Late, after hypertrophy |
| Embryonic timing | Week 8 fetal life | Week 8 (primary center) |
| Growth mechanism | Appositional only | Interstitial (physis) + appositional |
| Fracture healing | Primary union, distraction | Secondary union (callus) |
Both Produce Same Final Bone
Despite different pathways, both intramembranous and endochondral ossification produce identical lamellar bone. The pathway is determined by anatomical location and mechanical environment, not by final bone type. Woven bone (disorganized collagen) is an immature or pathological form seen in rapid ossification, always replaced by lamellar bone.
Differential of Impaired Ossification (Exam Discriminators)
Disorders of Ossification — Differentiating Features
| Disorder | Molecular defect | Pathway predominantly affected | Discriminating clinical clue |
|---|---|---|---|
| Achondroplasia | FGFR3 gain-of-function (G380R) | Endochondral (proliferative zone) | Rhizomelic short limbs, macrocephaly, normal trunk and intellect |
| Cleidocranial dysplasia | RUNX2 haploinsufficiency | Both (osteoblast maturation) — clavicle/skull | Absent/hypoplastic clavicles, wide fontanelles, dental anomalies |
| Osteogenesis imperfecta | Type I collagen (COL1A1/2) | Both (matrix quality) | Fragile bones, blue sclerae, dentinogenesis imperfecta |
| Rickets / osteomalacia | Vitamin D / phosphate handling | Endochondral (defective mineralisation of hypertrophic zone) | Widened physis, metaphyseal cupping/fraying, bowing |
| Cleidocranial vs Pyknodysostosis | Cathepsin K loss (pyknodysostosis) | Remodelling (osteoclast) | Dense brittle bone + acro-osteolysis distinguishes pyknodysostosis |
Clinical Applications
Ossification in Fracture Repair
Primary (Direct) Healing:
- Absolute stability (compression plating)
- Uses intramembranous ossification
- Cutting cone crosses fracture
- No visible callus
Secondary (Indirect) Healing:
- Relative stability (IM nail, cast)
- Uses endochondral ossification
- Cartilaginous callus replaced by bone
- Visible external callus
Why Secondary Healing Uses Endochondral
At fracture site with movement, low oxygen tension favors cartilage formation over direct bone. Cartilage is more tolerant of motion and hypoxia. As vascularity improves and stability increases, cartilage is replaced by bone via endochondral ossification - recapitulating embryonic development.
Evidence and References
Developmental Regulation of the Growth Plate
- Landmark review synthesising the signalling networks controlling endochondral bone formation
- Detailed the Ihh-PTHrP negative feedback loop: Ihh from prehypertrophic/hypertrophic chondrocytes drives PTHrP, which delays hypertrophy and maintains the proliferative pool
- Integrated FGF, BMP and Wnt signalling with Runx2/Sox9 transcriptional control
- Disruption of these pathways underlies human skeletal dysplasias
The Amazing Osteocyte
- Osteocytes comprise 90 to 95 percent of all bone cells and are the longest-lived bone cell
- Act as the principal mechanosensors orchestrating both osteoblast and osteoclast activity
- Function as endocrine cells regulating phosphate metabolism (via FGF23) and calcium availability
- Glucocorticoids and inflammatory cytokines induce osteocyte death, impairing remodelling
Cbfa1/Runx2 Is Essential for Both Ossification Pathways
- Cbfa1 (Runx2) knockout mice showed a complete lack of ossification and died at birth from respiratory failure
- Both intramembranous and endochondral ossification were blocked, owing to maturational arrest of osteoblasts
- Established Runx2 as the master transcription factor for osteoblast differentiation
- Cartilage anlage formed normally but no mineralisation occurred
The Tension-Stress Effect on the Genesis and Growth of Tissues (Part I)
- Canine tibial study establishing that gradual tension stress on living tissue stimulates regeneration
- Increased fixator stability and preservation of periosteum, marrow and medullary blood supply enhanced bone formation
- New bone formed parallel to the tension vector, even when applied perpendicular to the mechanical axis
- Bone marrow preservation during osteotomy was critical for osteogenesis
FGFR3 Mutations Cause Achondroplasia
- Identified a recurrent G380R missense mutation in the transmembrane domain of FGFR3 in 23 of 23 achondroplasia cases
- Confirmed achondroplasia as a fully penetrant autosomal dominant trait (incidence approximately 1 in 15,000)
- Mutation is gain-of-function: constitutively active FGFR3 inhibits chondrocyte proliferation in the proliferative zone
- Most cases sporadic with paternal-origin de novo mutation
Vosoritide in Children with Achondroplasia (Phase 3 Extension)
- C-type natriuretic peptide analogue antagonising FGFR3 downstream signalling to restore endochondral growth
- Annualised growth velocity rose from 4.26 to 5.52 cm/year at 104 weeks in the treated cohort
- Placebo crossover children gained a comparable increase after starting vosoritide
- No new safety signals over 2 years of daily treatment
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Ossification Pathways (~3 min)
"Compare and contrast intramembranous and endochondral ossification."
Scenario 2: Growth Plate Structure (~3 min)
"Describe the zones of the growth plate and explain the clinical relevance to Salter-Harris fractures."
Scenario 3: Ossification Defects and Skeletal Dysplasia (~4 min)
"A child presents with disproportionate short stature affecting the limbs more than the trunk, with normal intelligence and macrocephaly. How does ossification biology explain the phenotype, and how does this contrast with a child who has clavicular and skull-vault defects?"
MCQ Practice Points
Pathway Question
Q: Which bones form via intramembranous ossification? A: Flat bones of skull, facial bones, mandible, and clavicle. All other bones use endochondral ossification.
Growth Plate Zone Question
Q: Which growth plate zone is the weakest and site of Salter-Harris fracture propagation? A: Hypertrophic zone - large cells with minimal surrounding matrix make this the mechanically weakest area.
Distraction Question
Q: What type of ossification occurs in distraction osteogenesis? A: Intramembranous ossification - direct bone formation along axis of tension stress without cartilage intermediate.
Secondary Healing Question
Q: Why does secondary fracture healing use endochondral ossification? A: Low oxygen tension and movement at fracture site favors cartilage formation. Cartilage is more tolerant of hypoxia and motion. As vascularity improves, cartilage is replaced by bone via endochondral pathway.
Clavicle Question
Q: What is unique about clavicle ossification? A: Only long bone formed by intramembranous ossification but has a medial growth plate (physis) for longitudinal growth. First bone to ossify (week 5-6 fetal life).
Guidelines, Registries & Global Practice
Global Epidemiology of Ossification Disorders
| Condition | Global frequency | Pathway affected |
|---|---|---|
| Achondroplasia (FGFR3) | ~1 in 15,000–30,000 live births | Endochondral (proliferative zone) |
| Osteogenesis imperfecta (type I collagen) | ~1 in 15,000–20,000 | Both (matrix quality) |
| Cleidocranial dysplasia (RUNX2) | ~1 in 1,000,000 | Both (osteoblast maturation) — clavicle/skull |
| Slipped capital femoral epiphysis | ~1–10 per 100,000 adolescents (rising with obesity) | Endochondral (hypertrophic zone shear) |
Side-by-Side Society Guidance
| Body | Relevant position |
|---|---|
| AO Foundation | Fracture-healing biology — absolute stability favours direct (intramembranous/contact) healing; relative stability favours endochondral callus |
| AAOS (US) | Paediatric physeal injury management; vitamin D / metabolic bone optimisation in healing |
| BOA / BOAST (UK) | Standards for paediatric fracture and limb-reconstruction care, including physeal-sparing principles |
| EFORT / European consensus | Limb-lengthening and bone-transport (distraction osteogenesis) standards and complication reporting |
| International achondroplasia consensus (2022) | Multidisciplinary care; vosoritide as the first disease-modifying option in eligible children |
Registry and Outcome Notes
- Distraction osteogenesis / limb reconstruction registries (e.g. ASAMI/ILLRS-affiliated databases) track external-fixator vs magnetic intramedullary lengthening — both rely on tension-stress intramembranous regenerate.
- Magnetic motorised nails (e.g. lengthening intramedullary devices) have shifted practice from external frames in high-resource settings; circular frames remain the workhorse where implant cost is prohibitive.
High- vs Limited-Resource Practice Variation
- High-resource: magnetic lengthening nails, vosoritide for eligible achondroplasia, advanced 3D deformity planning.
- Limited-resource: Ilizarov/circular external fixation remains the global standard for lengthening and bone transport — low implant cost, no power source, supports infected/segmental defect reconstruction.
- SUFE and physeal injuries present later in settings with limited access to imaging, increasing avascular necrosis and growth-arrest rates.
Controversies and Areas of Uncertainty
- Optimal distraction rate/rhythm: ~1 mm/day in divided steps is the Ilizarov standard, but younger patients and accordion/dynamisation protocols may tolerate variation; over-rapid distraction risks poor regenerate, too slow risks premature consolidation.
- Definition of "primary" healing: truly gap-free contact (Haversian/cutting-cone) healing is rare clinically; most "absolute stability" constructs heal through a mix of contact and small-gap intramembranous bone.
- Disease-modifying dysplasia therapy: vosoritide improves growth velocity (a surrogate), but durable effects on final height, body proportion, foramen magnum stenosis and quality of life are still being established.
- Physeal-bar prevention: no intervention reliably prevents bar formation after high-grade Salter-Harris injuries; interposition grafting outcomes remain variable.
Management Algorithm
OSSIFICATION PATHWAYS
Clinical summary
Intramembranous
- •Direct mesenchyme → bone (no cartilage)
- •Flat bones: skull, face, mandible, clavicle
- •MSC → osteoblast → osteoid → mineralization
- •Used in: primary fracture healing, distraction osteogenesis
Endochondral
- •Mesenchyme → cartilage → bone (cartilage template)
- •Long bones, axial skeleton, pelvis
- •Cartilage model → hypertrophy → vascular invasion → ossification
- •Growth plate = persistent endochondral zone until closure
Growth Plate Zones (RZPHO)
- •Reserve: sparse cells, stem cell niche
- •Proliferative: columnar stacks, rapid division
- •Hypertrophic: large cells, calcified matrix (WEAKEST)
- •Ossification: apoptosis, vascular invasion, bone deposition
Growth Plate Regulation
- •Ihh-PTHrP loop maintains proliferative zone
- •Growth hormone → IGF-1 → promotes growth
- •Estrogen (high dose) → physeal closure
- •Zone of Ranvier = peripheral fibrous support
Clinical Applications
- •Primary fracture healing = intramembranous
- •Secondary fracture healing = endochondral (cartilage callus)
- •Salter-Harris fractures through hypertrophic zone
- •SUFE = shear through hypertrophic zone of proximal femur
Key Differences
- •Intramembranous: early vascular, direct bone, appositional growth
- •Endochondral: late vascular, cartilage first, interstitial + appositional
- •Both produce lamellar bone (same end product)
- •Woven bone = immature form, always replaced