Ectopic Spinal Ligament Ossification | Cervical Myelopathy | East Asian Prevalence
- OPLL is ectopic ossification of the PLL causing cervical canal stenosis and compressive myelopathy
- East Asian prevalence is 10-20 times higher than Western populations; strong genetic association (COL6A1, rs6919606)
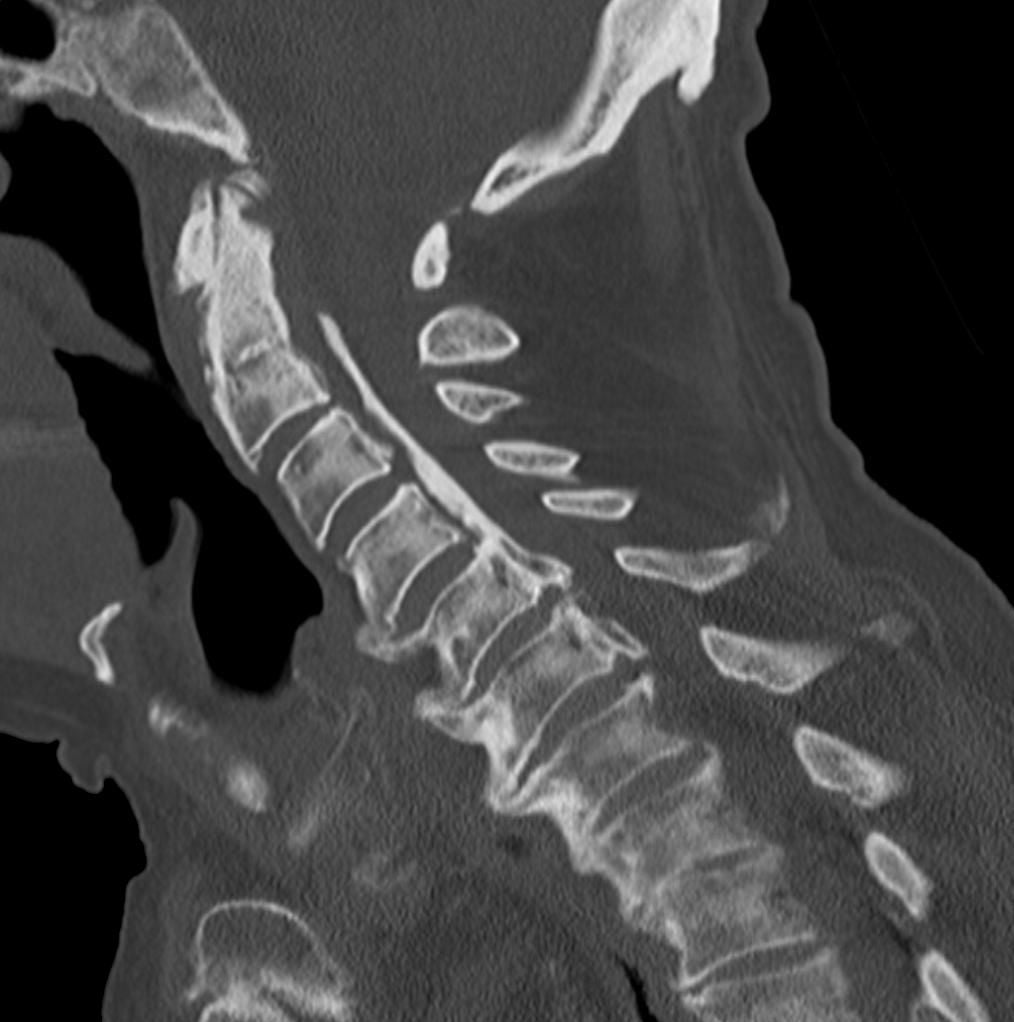
- CT is the gold standard for diagnosis and classification (sagittal reformats show ossification morphology)
- K-line on lateral cervical radiograph predicts outcome of posterior decompression: K-line positive = good result, K-line negative = consider anterior approach
- Dural ossification (double-layer sign or single-layer sign on CT) predicts intraoperative CSF leak and dural defect
- “OPLL is the most common cause of cervical myelopathy in Japan
- “Four types: continuous, segmental, mixed, localised (know CT appearances)
- “K-line positive = ossification does not cross the line connecting C2 and C7 mid-vertebral body points
- “Anterior approach directly removes OPLL but risks dural injury; posterior decompresses indirectly via posterior shift of the cord
- “Ossification of the ligamentum flavum (OLF) can coexist, especially in the thoracic spine
Japanese prevalence 1.9-4.3 percent; symptomatic myelopathy in 5-15 percent of those with OPLL. East Asian populations (Japanese, Korean, Chinese) affected 10-20 times more frequently than Caucasian populations. Male-to-female ratio approximately 2:1. Mean onset age 40-60 years.
K-line = straight line connecting midpoints of C2 and C7 vertebral bodies on lateral radiograph. K-line positive: OPLL does not cross the K-line (predicts good outcome after laminoplasty). K-line negative: OPLL crosses the K-line (posterior decompression alone may be insufficient, consider anterior approach).
Dural ossification occurs when the OPLL mass incorporates the ventral dura. CT signs: double-layer sign (two distinct ossified layers with intervening hypodense band) or single-layer sign (homogeneous ossified mass without visible dura). Present in approximately 5.7 percent of surgical cases and predicts intraoperative CSF leak.
Anterior = direct removal of OPLL mass but high dural injury risk. Posterior = indirect decompression via posterior cord shift. Choice depends on OPLL type, canal occupancy ratio, K-line status, number of levels involved, cervical alignment, and presence of dural ossification. Mixed and continuous types often require multi-level surgery.
- Diagnosis
- CT confirms type, MRI no cord signal change
- Treatment
- Observation with serial follow-up
- Key Pearl
- Most OPLL is asymptomatic; treat only when myelopathy develops
- Diagnosis
- MRI: cord compression with T2 signal change; CT: OPLL classification
- Treatment
- Posterior laminoplasty
- Key Pearl
- K-line positive predicts good outcome with posterior decompression
- Diagnosis
- Anterior OPLL displacing cord, kyphotic alignment
- Treatment
- Anterior corpectomy with OPLL resection or floating method
- Key Pearl
- Posterior decompression alone insufficient when OPLL crosses K-line
- Diagnosis
- Double-layer sign on CT; anterior OPLL with canal occupancy greater than 60 percent
- Treatment
- Anterior approach with dural repair planning or posterior decompression
- Key Pearl
- Pre-operative recognition of dural ossification allows CSF leak prevention planning
DOSSDural Ossification CT Signs
Hook:DOSS = Dural Ossification Signs on CT - recognise BEFORE the operation, not during!
Overview and Epidemiology
OPLL is the most common cause of cervical compressive myelopathy in East Asian populations and is increasingly recognised worldwide with advancing imaging. It is a condition where the posterior longitudinal ligament undergoes progressive ectopic endochondral ossification, producing a mass that encroaches on the spinal canal. The condition is frequently asymptomatic and discovered incidentally, but when symptomatic myelopathy develops, timely surgical decompression is essential to prevent irreversible cord damage. Knowledge of the CT classification, K-line concept, and dural ossification risk is critical for both the FRACS and FRCS spine examinations.
- Japan: 1.9-4.3 percent prevalence in adults on CT/radiograph screening
- Korea and China: Comparable prevalence to Japan
- Caucasian populations: 0.1-0.3 percent (10-20 times lower)
- Male predominance: Ratio approximately 2:1
- Age of onset: Typically 40-60 years, slowly progressive
- Genetic association: COL6A1 polymorphism (rs6919606), R-Spondin 2 pathway, N-cadherin
- Cervical myelopathy: Most common symptomatic presentation
- Asymptomatic: Majority of OPLL is discovered incidentally
- Progressive: Natural history involves slow ossification growth over years
- Spinal levels: C3-C5 most commonly affected; can extend from C2 to thoracic spine
- Coexisting ossification: OLF (ligamentum flavum) and OYL (yellow ligament) in 5-10 percent
- Trauma sensitivity: Minor trauma can precipitate acute myelopathy in pre-existing OPLL
Pathophysiology
OPLL develops through endochondral ossification of the posterior longitudinal ligament, mediated by osteogenic differentiation of ligamentous mesenchymal stem cells. The PLL normally runs along the posterior surface of the vertebral body from C2 to the sacrum, forming the anterior boundary of the spinal canal. In OPLL, the ligament undergoes progressive replacement by mature lamellar bone through a sequence of ligament hypertrophy, chondroid metaplasia, and endochondral ossification. Key molecular drivers include BMP-2, BMP-4, and BMP-7 (bone morphogenetic proteins), osteocalcin, Runx2, and Sox9. The COL6A1 gene (collagen type VI alpha 1) has the strongest genetic association, and the condition shares pathogenic pathways with diffuse idiopathic skeletal hyperostosis (DISH) and ossification of the ligamentum flavum (OLF). The OPLL mass grows anterior to the dura and can eventually incorporate or replace the ventral dural layer, creating the surgical challenge of dural ossification.
- Histology
- Fibrocartilaginous proliferation within PLL
- Imaging Correlate
- Thickened PLL on MRI, no ossification on CT
- Clinical Significance
- Pre-clinical, not detectable on radiographs
- Histology
- Cartilaginous foci within the ligament substance
- Imaging Correlate
- Early punctate calcification on CT
- Clinical Significance
- Progressive but may remain asymptomatic
- Histology
- Mature lamellar bone replacing cartilage
- Imaging Correlate
- Clear ossification on CT, hyperdense on sagittal reformats
- Clinical Significance
- Canal encroachment begins; myelopathy possible
- Histology
- Ossification incorporates ventral dura
- Imaging Correlate
- Double-layer sign or single-layer sign on CT
- Clinical Significance
- CSF leak risk at surgery; dural defect anticipated
Key growth factors: BMP-2, BMP-4, BMP-7 (osteogenic), TGF-beta (profibrotic)
Transcription factors: Runx2 (osteoblast differentiation), Sox9 (chondrogenesis)
Genetic loci: COL6A1 (collagen VI), R-Spondin 2 (Wnt signalling), N-cadherin
Systemic associations: DISH, metabolic syndrome, hyperinsulinaemia, hypoparathyroidism
Mechanical factors: Repeated micro-trauma to PLL may trigger osteogenic response
- Ethnicity: East Asian heritage (Japanese, Korean, Chinese)
- Genetics: Family history of OPLL increases risk 5-10 times
- Metabolic: Diabetes mellitus, impaired glucose tolerance, hyperinsulinaemia
- Endocrine: Hypoparathyroidism (classical association)
- Skeletal: DISH (Forestier disease) coexists in 25-40 percent of OPLL patients
- Dietary: High salt and low animal protein diet proposed (epidemiological correlation)
- Mechanical: Cervical spine repetitive stress, occupational neck loading
Classification and Types
Japanese Investigation Committee Classification (1994)
The CT-based classification is the standard system for OPLL, defining four types based on the morphological pattern of ossification on sagittal CT reformats:
- Morphology on Sagittal CT
- Ossification extends across vertebral bodies and disc spaces as a single uninterrupted band
- Frequency
- Approximately 27-30 percent
- Surgical Implication
- Often requires multi-level anterior corpectomy or skip corpectomy
- Morphology on Sagittal CT
- Ossification present behind vertebral bodies only, with sparing at disc levels
- Frequency
- Approximately 39-43 percent (most common)
- Surgical Implication
- Posterior laminoplasty effective if K-line positive
- Morphology on Sagittal CT
- Combination of continuous and segmental patterns
- Frequency
- Approximately 26-30 percent
- Surgical Implication
- Approach determined by K-line and number of levels
- Morphology on Sagittal CT
- Ossification confined to the disc level only
- Frequency
- Approximately 2-5 percent (rarest)
- Surgical Implication
- Anterior discectomy or single-level corpectomy
The canal occupancy ratio (OPLL thickness divided by canal anteroposterior diameter on axial CT) quantifies severity: less than 30 percent is mild, 30-60 percent moderate, and greater than 60 percent severe. Surgical decompression is generally recommended when the ratio exceeds 60 percent or progressive myelopathy is present.
This topic is cervical-focused, but the examinable contrast is thoracic OPLL, which is less common than cervical OPLL yet far more dangerous - it carries the highest neurological-deterioration rate of any OPLL surgery and behaves differently for two anatomical reasons.
- The spine is kyphotic, not lordotic: in the kyphotic thoracic spine the cord already lies draped against the anterior ossified mass, so posterior decompression alone allows little posterior cord drift - the K-line/posterior-shift logic that works in the lordotic cervical spine often fails here, and decompression may be inadequate or the cord can even be injured.
- The thoracic cord has a watershed blood supply (especially the mid-thoracic region), making it vulnerable to ischaemic injury during decompression and manipulation.
- Circumferential compression: T-OPLL frequently coexists with ossification of the ligamentum flavum (OLF) posteriorly, producing front-and-back ("pincer") compression that a single-sided decompression cannot relieve.
Surgical strategy differs accordingly: options include posterior decompression with instrumented fusion (often with some kyphosis correction/dekyphosis), posterolateral or anterior (transthoracic) decompression for a focal anterior beak, or a circumferential procedure for combined OPLL+OLF. Intra-operative neuromonitoring (MEP and SSEP) is essential given the high cord-injury risk, and patients must be counselled that transient or permanent neurological worsening is more common than after cervical surgery.
Exam point: thoracic OPLL is rarer but more dangerous than cervical - the kyphotic alignment defeats posterior cord drift, the watershed thoracic cord is ischaemia-prone, and it often combines with OLF for circumferential compression, so management leans on decompression with instrumented fusion (sometimes dekyphosis) under neuromonitoring, with a higher neurological-complication rate.
CSMLOPLL CT Classification Types
Hook:CSML = Continuous, Segmental, Mixed, Localised - the four OPLL types in order of frequency!
Clinical Assessment
- Insidious onset: Slowly progressive clumsiness of hands, gait disturbance over months to years
- Hand dexterity: Difficulty with buttons, chopsticks, writing (early sign)
- Gait: Stiff-legged, spastic gait; frequent falls
- Bowel and bladder: Urinary hesitancy, urgency, incontinence in advanced cases
- Neck pain: May be present but often minimal relative to degree of myelopathy
- Trauma history: Minor trauma (whiplash, fall) can precipitate acute deterioration
- Motor: Upper limb weakness (intrinsic hand muscles), lower limb spastic weakness
- Reflexes: Hyperreflexia, Hoffmann sign positive, Babinski sign positive
- Sensory: Variable sensory loss below the level of compression
- Gait: Spastic, broad-based, decreased proprioception
- Neck range: May be limited; cautious examination to avoid precipitating myelopathy
- Lhermitte sign: Electric shock sensation with neck flexion (non-specific)
The modified Japanese Orthopaedic Association (mJOA) score (0-18) is the standard clinical tool for assessing cervical myelopathy severity:
- Mild myelopathy: mJOA 15-17 (subtle hand dysfunction, no gait disturbance)
- Moderate myelopathy: mJOA 12-14 (obvious hand dysfunction, mild gait disturbance)
- Severe myelopathy: mJOA less than 12 (marked gait disturbance, possible bowel and bladder dysfunction)
Surgical decompression is generally recommended for moderate and severe myelopathy (mJOA less than 15) and for progressive mild myelopathy. The mJOA recovery rate is used to quantify post-operative improvement.
- Key Discriminator
- East Asian ethnicity, ossified PLL on CT
- Imaging Finding
- Hyperdense band posterior to vertebral body on CT
- Management Difference
- Ossification-specific surgical planning required
- Key Discriminator
- Disc-osteophyte complexes, no ossification
- Imaging Finding
- Disc protrusion and osteophytes on MRI/CT, no OPLL
- Management Difference
- Standard anterior or posterior decompression
- Key Discriminator
- Acute onset, often radicular component
- Imaging Finding
- Focal disc extrusion on MRI
- Management Difference
- Anterior discectomy and fusion
- Key Discriminator
- Posterior compression, thoracic more common
- Imaging Finding
- Hyperdense mass in ligamentum flavum on CT
- Management Difference
- Laminectomy for posterior decompression
- Key Discriminator
- Progressive myelopathy with vascular congestion
- Imaging Finding
- Flow voids on MRI, dilated perimedullary veins
- Management Difference
- Endovascular or surgical fistula obliteration
- Key Discriminator
- Upper and lower motor neuron signs, no sensory loss
- Imaging Finding
- No structural compression on imaging
- Management Difference
- Medical management, not surgical
Differentiating OPLL from cervical spondylotic myelopathy is critical because OPLL carries additional surgical risks (dural ossification, CSF leak) and may require different operative strategies. OPLL is confirmed by demonstrating ossification of the PLL on CT (not just disc protrusion or osteophytes). Always obtain CT in addition to MRI when OPLL is suspected, as MRI may not clearly distinguish between OPLL, disc material, and osteophytes. The ossified mass appears dark on both T1 and T2 MRI sequences, whereas disc material is typically T2 hyperintense.
The history section notes that minor trauma can precipitate acute deterioration - this is a high-yield emergency scenario in its own right, because a canal already narrowed by OPLL has no reserve space for the cord.
- Mechanism: a relatively trivial hyperextension injury (a fall onto the face, a low-speed motor vehicle collision, even a fall from standing in an older patient) momentarily buckles the ligamentum flavum and pinches the cord between it and the anterior OPLL - often producing a spinal cord injury without any fracture or dislocation (the SCIWORA-type pattern in adults with stenosis).
- The classic syndrome is acute central cord syndrome: the most common incomplete cord injury, with upper-limb weakness disproportionately worse than the legs (hands worst), variable bladder dysfunction and sacral sparing, reflecting the central/medial location of the cervical (hand) fibres.
- Acute management: urgent MRI to define cord compression and signal change; maintain spinal cord perfusion (support mean arterial pressure, often a MAP target around 85 to 90 mmHg) and avoid hypotension/hyperextension; high-dose steroids are not routinely recommended. For a patient with ongoing cord compression, early surgical decompression (increasingly favoured, often within about 24 hours) gives better neurological recovery than delayed surgery, though a purely central cord injury with minimal residual compression may initially be managed expectantly.
- The prevention message: this is exactly why an asymptomatic OPLL patient must be counselled about trauma risk and why a pre-existing stenotic OPLL lowers the threshold for considering decompression.
Exam point: an OPLL-stenosed canal turns minor hyperextension trauma into a spinal cord injury without fracture, classically an acute central cord syndrome (arms worse than legs, sacral sparing) - manage with urgent MRI, MAP-supported cord perfusion, no routine steroids, and early decompression when compression persists.
Investigations
Imaging Protocol
Views: AP, lateral, flexion-extension of cervical spine
Look for: Radiodense band posterior to vertebral bodies (OPLL), cervical alignment (lordosis vs kyphosis), DISH features (flowing anterior osteophytes)
Limitation: May miss early or small OPLL; CT is more sensitive
Gold standard for OPLL diagnosis and classification
Axial cuts: Assess canal occupancy ratio, dural ossification signs (double-layer, single-layer)
Sagittal reformats: Classify OPLL type (continuous, segmental, mixed, localised)
Measurements: Canal occupancy ratio = OPLL thickness divided by sagittal canal diameter
Assess cord compression and signal change
T2 sagittal/axial: Cord compression at OPLL levels, T2 hyperintensity in cord = myelomalacia
T1: OPLL appears as low signal anterior to cord; helps distinguish from disc material
Prognostic value: Pre-operative T2 cord signal change correlates with post-operative recovery; multi-level high signal predicts poorer outcome
When MRI is contraindicated (pacemaker, cochlear implant)
Shows: Contrast outline of the thecal sac and relationship between OPLL mass and cord
Dural assessment: Can confirm dural ossification when CT signs are equivocal
Assess cervical instability or mobile OPLL
Segmental mobility: Important if planning posterior surgery; instability may necessitate fusion
Caveat: Perform cautiously in myelopathic patients to avoid cord injury

The minimum imaging workup for suspected OPLL myelopathy is CT + MRI. CT classifies the OPLL and evaluates dural ossification. MRI assesses cord compression and signal change. The lateral radiograph is used for the K-line but is not sufficient for diagnosis. Always report the OPLL type, canal occupancy ratio, K-line status, and presence or absence of dural ossification signs.
- Severity
- Mild
- Typical mJOA
- 15-17 (mild or normal)
- Management
- Observation if no myelopathy; serial imaging
- Severity
- Moderate
- Typical mJOA
- 12-14 (moderate)
- Management
- Surgical decompression if progressive myelopathy
- Severity
- Severe
- Typical mJOA
- Less than 12 (severe)
- Management
- Urgent surgical decompression recommended
Management Algorithm
Observation for Asymptomatic and Mild OPLL
Goal: Monitor for progression and prevent myelopathy development
Observation Protocol
CT: Classify OPLL type and measure canal occupancy
MRI: Assess cord compression and signal change
Clinical: mJOA score, hand function assessment, gait evaluation
Counselling: Educate patient on myelopathy symptoms to watch for
Serial imaging: CT or MRI at 6-12 month intervals for 2-3 years
Clinical review: mJOA score, new symptoms (hand clumsiness, gait change)
Red flags: Any neurological deterioration prompts surgical discussion
Activity modification: Avoid high-impact activities, contact sports, extreme neck positions
No proven disease-modifying therapy for OPLL progression
Experimental: Bisphosphonates, vitamin K2 (menatetrenone), and etidronate have been studied with limited evidence for slowing ossification progression
Analgesia: Simple analgesics for neck pain; avoid opioids in myelopathic patients
Physiotherapy: Gentle range of motion exercises; avoid aggressive cervical manipulation
Most OPLL is asymptomatic and does not require surgery. However, the risk of progression to myelopathy is approximately 1-3 percent per year, and minor trauma can precipitate acute neurological deterioration. Patients under observation must be educated about myelopathy symptoms and advised to seek urgent review if these develop. There is no proven pharmacological treatment to halt OPLL progression.
KAPK-line Assessment for Surgical Planning
Hook:KAP = K-line Assessment determines Plan - positive for posterior, negative needs anterior!
Complications
- Incidence
- 5-32 percent with anterior approach (higher with dural ossification)
- Risk Factors
- Dural ossification, continuous type, anterior approach
- Management
- Intra-operative repair, lumbar drain 3-5 days, fascial graft, tissue sealant
- Incidence
- 5-15 percent after posterior decompression
- Risk Factors
- Posterior cord shift, foraminal stenosis at C4-C5
- Management
- Observation (most recover 6-12 months), targeted therapy, consider prophylactic foraminotomy
- Incidence
- 10-30 percent show progression at 5 years post-operatively
- Risk Factors
- Young age, continuous type, metabolic syndrome
- Management
- Serial imaging, no proven pharmacological prevention
- Incidence
- 10-20 percent partial closure over time
- Risk Factors
- Hinge fracture, inadequate spacer, poor bone quality
- Management
- May require revision with laminectomy and fusion
- Incidence
- 5-15 percent at 5 years (higher with fusion than laminoplasty)
- Risk Factors
- Fusion constructs, long-segment fixation
- Management
- Conservative initially; revision extension of fusion if symptomatic
- Incidence
- 5-10 percent after corpectomy
- Risk Factors
- Multi-level corpectomy, osteoporosis, poor endplate preparation
- Management
- Revision fixation; consider posterior augmentation
- Incidence
- 1-3 percent
- Risk Factors
- Antiplatelet therapy, extensive decompression, inadequate drainage
- Management
- Emergency wound exploration and evacuation if cord compression
CSF leak is the most feared and characteristic complication of anterior OPLL surgery, directly related to dural ossification. The incidence ranges from 5 percent (when no dural signs are present) to over 30 percent (when the double-layer or single-layer sign is identified on pre-operative CT). Prevention strategies include pre-operative identification of dural ossification signs, use of the floating method instead of OPLL resection, and having dural repair materials available. When CSF leak occurs, management includes primary repair or patch graft, lumbar drainage for 3-5 days, and close monitoring for pseudomeningocele and meningitis.
Outcomes and Prognosis
- Indication
- Segmental OPLL, lordosis, multi-level
- Expected Neurological Recovery
- mJOA improvement 3-5 points; 60-80 percent recovery rate
- Key Complications
- C5 palsy, laminoplasty closure, axial neck pain
- Indication
- Localised or segmental OPLL, kyphosis
- Expected Neurological Recovery
- mJOA improvement 4-6 points; 70-85 percent recovery rate
- Key Complications
- CSF leak, graft complications, dysphagia
- Indication
- Severe multi-level OPLL, K-line negative, kyphosis
- Expected Neurological Recovery
- mJOA improvement 3-5 points; variable recovery rate
- Key Complications
- High morbidity, blood loss, infection, prolonged recovery
Best prognosis: Segmental type, K-line positive, mJOA greater than 12, duration of myelopathy less than 12 months, no T2 cord signal change on MRI, age less than 65 years
Poor prognosis: Continuous or mixed type, K-line negative, mJOA less than 10, long-standing myelopathy (greater than 2 years), multi-level T2 cord hyperintensity, age greater than 70 years
Key threshold: Duration of myelopathy is the most important modifiable prognostic factor - earlier decompression yields better outcomes. Do not delay surgery in progressive myelopathy.
Guidelines, Registries & Global Practice
- East Asia: Highest prevalence worldwide (Japan 1.9-4.3 percent, Korea and China comparable)
- North America and Europe: 0.1-0.3 percent prevalence; increasing recognition with widespread CT usage
- Male predominance: 2:1 ratio globally
- Age distribution: Onset typically 40-60 years across all ethnicities
- Rising diagnosis: Global increase in OPLL detection paralleling increased CT utilisation, suggesting true prevalence in non-Asian populations may be higher than historical estimates
- Japan and Korea: Extensive surgical experience with laminoplasty; OPLL-specific instrumentation and techniques widely available
- North America: OPLL less commonly encountered; anterior approaches more familiar to spine surgeons; laminoplasty expertise concentrated in specialist centres
- Europe: Mixed practice; increasing adoption of laminoplasty for multi-level OPLL; anterior approaches preferred for focal disease
- Resource-limited settings: CT availability is the primary diagnostic barrier; laminectomy (without instrumentation) may be the only available surgical option
- Universal principle: Regardless of region, CT + MRI assessment, K-line analysis, and dural ossification screening should guide surgical planning
- Diagnosis Emphasis
- CT classification mandatory; mJOA scoring for all patients
- Surgical Approach
- Laminoplasty for K-line positive multi-level disease; anterior for K-line negative or focal OPLL
- Special Considerations
- Developed the K-line concept; extensive laminoplasty experience
- Diagnosis Emphasis
- CT and MRI essential; systematic classification of OPLL type
- Surgical Approach
- Approach based on K-line, alignment, number of levels, and dural status
- Special Considerations
- Prospective multicentre data on laminoplasty outcomes supports posterior approach for suitable candidates
- Diagnosis Emphasis
- MRI for myelopathy assessment; CT if OPLL suspected
- Surgical Approach
- Specialist spinal centre management; approach individualised
- Special Considerations
- Posterior decompression preferred for multi-level disease; anterior for focal disease with kyphosis
- Diagnosis Emphasis
- CT and MRI recommended; OPLL classification when identified
- Surgical Approach
- Surgeon experience and OPLL-specific factors guide approach
- Special Considerations
- Higher proportion of anterior surgery in US practice; increasing laminoplasty adoption
There is no dedicated international OPLL registry comparable to arthroplasty registries. The largest datasets come from the Japanese Investigation Committee on OPLL (nationwide surveys of over 10,000 cases), the AOSpine International study (prospective multicentre), and individual high-volume centre series from Japan and Korea. The Japanese nationwide surveys provide the most comprehensive natural history data and form the basis of current classification and management recommendations.
Record in every OPLL surgical planning case:
- OPLL type on CT (continuous, segmental, mixed, localised)
- Canal occupancy ratio (percentage)
- K-line status (positive or negative)
- Dural ossification signs on axial CT (double-layer, single-layer, or absent)
- Cervical alignment (lordotic, straight, or kyphotic)
- mJOA score
- Number of levels involved
- Presence or absence of coexisting OLF or DISH
These factors collectively determine the surgical approach and must be documented before the operative plan is finalised.
Controversies & Areas of Uncertainty
While K-line negative status suggests posterior decompression alone is insufficient, the optimal alternative (anterior corpectomy vs combined approach vs posterior decompression with fusion) remains debated. Some surgeons advocate a trial of posterior decompression with instrumented fusion for K-line negative patients to achieve indirect decompression via cervical alignment correction, avoiding anterior dural ossification risk entirely.
The floating method avoids dural injury but leaves residual OPLL anterior to the cord, and the time course of anterior migration (weeks to months) means decompression is not immediate. Direct OPLL resection achieves immediate decompression but carries high CSF leak risk when dural ossification is present. No randomised trial has compared these techniques head-to-head.
Bisphosphonates, vitamin K2 (menatetrenone), etidronate, and other agents have shown limited and conflicting evidence for slowing OPLL progression. No pharmacological therapy is currently recommended in any major guideline. Research into BMP pathway inhibitors and anti-osteogenic agents is ongoing but not yet clinically available.
Laminoplasty preserves motion but risks closure over time and does not address kyphotic alignment. Laminectomy with fusion corrects alignment but sacrifices motion segments and increases adjacent segment disease risk. The choice remains surgeon-dependent as no large RCT has definitively favoured one over the other for OPLL specifically.
MCQ Practice Points
Q: What is the prevalence of OPLL in the Japanese adult population? A: 1.9 to 4.3 percent based on population CT screening studies. This is approximately 10-20 times higher than in Caucasian populations. The condition is also common in Korean and Chinese populations, suggesting a shared genetic predisposition.
Q: What are the four CT types of OPLL according to the Japanese Investigation Committee classification? A: Continuous, segmental, mixed, and localised (circumscribed). Segmental type is the most common (approximately 40 percent), followed by continuous (approximately 28 percent), mixed (approximately 28 percent), and localised (approximately 2-5 percent). The classification is based on sagittal CT reformats.
Q: What is the K-line and how does it guide surgical approach selection in OPLL? A: The K-line is a straight line connecting the midpoints of C2 and C7 vertebral bodies on the lateral cervical radiograph. K-line positive (OPLL does not cross the line) = posterior laminoplasty is appropriate. K-line negative (OPLL crosses the line) = posterior decompression alone is insufficient; anterior or combined approach is needed. The K-line reflects whether the cord can shift posteriorly away from the OPLL mass.
Q: What CT signs predict dural ossification in OPLL and what is their surgical significance? A: The double-layer sign (two hyperdense layers with intervening hypodense band on axial CT) and the single-layer sign (homogeneous ossified mass without visible dura) both predict dural ossification. When present, direct OPLL resection will almost certainly create a dural defect and CSF leak. The floating method (thinning the OPLL without resection) is the preferred surgical technique when these signs are identified.
Q: When is anterior surgery preferred over posterior surgery for OPLL myelopathy? A: Anterior surgery is preferred when: K-line negative (OPLL crosses K-line), cervical kyphosis, localised OPLL (1-2 levels), high canal occupancy (greater than 60 percent) with focal compression, and failed posterior decompression. Posterior surgery is preferred when: K-line positive, multi-level involvement (3 or more levels), preserved cervical lordosis, and segmental type OPLL.
Q: What is the pathogenesis of OPLL and which genetic locus is most strongly associated? A: OPLL develops through endochondral ossification of the PLL, driven by osteogenic differentiation of ligamentous mesenchymal cells under the influence of BMP-2, BMP-4, BMP-7, Runx2, and Sox9. The strongest genetic association is with the COL6A1 gene (collagen type VI alpha 1) polymorphism. OPLL shares pathogenic pathways with DISH and OLF.
Clinical Imaging
OPLL Radiographic and CT Appearances
OPLL is best visualised on CT sagittal reformats, where ossification appears as a hyperdense strip along the posterior vertebral body margin, distinct from the vertebral cortex. On lateral radiographs, OPLL may be visible as a radiodense band posterior to the vertebral bodies. MRI demonstrates the ossified mass as low signal on both T1 and T2 sequences, with associated cord compression and often T2 hyperintensity within the cord parenchyma indicating myelomalacia. The combination of CT (for bone detail and classification) and MRI (for cord signal and compression) is essential for surgical planning.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old Japanese man presents with progressive hand clumsiness and gait disturbance over 8 months. Examination reveals hyperreflexia in all four limbs, positive Hoffmann sign bilaterally, and a spastic gait. mJOA score is 11. MRI shows cervical cord compression from C3 to C5 with T2 signal change in the cord. CT demonstrates a continuous type OPLL with canal occupancy of 55 percent. The OPLL mass does not cross the K-line on lateral radiograph. No dural ossification signs are seen on axial CT. What is your diagnosis and management plan?”
“A 48-year-old Korean woman with known OPLL presents with rapidly progressive cervical myelopathy over 3 months. MRI shows severe cord compression at C4-C5 with multi-level T2 signal change. CT demonstrates mixed type OPLL with 70 percent canal occupancy at C4-C5, and the OPLL mass crosses the K-line. Axial CT at C4 shows a double-layer sign. mJOA is 8. What is your surgical plan and how do you manage the dural ossification risk?”
Epidemiology and Pathogenesis
- Japanese prevalence 1.9-4.3 percent; East Asian populations affected 10-20 times more than Caucasians
- Endochondral ossification of PLL driven by BMP signalling; COL6A1 gene strongest genetic association
- Male-to-female ratio 2:1; onset age 40-60 years; C3-C5 most commonly affected levels
- Associated conditions: DISH (25-40 percent), diabetes mellitus, metabolic syndrome, hypoparathyroidism
CT Classification (Japanese Investigation Committee)
- Segmental (most common, approximately 40 percent): ossification behind vertebral bodies only
- Continuous (approximately 28 percent): ossification spans bodies and discs
- Mixed (approximately 28 percent): combination of continuous and segmental
- Localised (approximately 2-5 percent): ossification at disc level only, rarest type
K-line and Surgical Planning
- K-line: straight line from C2 to C7 mid-vertebral body points on lateral radiograph
- K-line positive (OPLL anterior to line): posterior laminoplasty is appropriate
- K-line negative (OPLL crosses line): anterior or combined approach required
- K-line predicts whether posterior cord shift can achieve decompression
Dural Ossification
- Double-layer sign: two ossified layers with hypodense band on axial CT = dural ossification
- Single-layer sign: homogeneous ossified mass without visible dura = high dural risk
- CSF leak rate 5-32 percent with anterior approach; floating method reduces risk
- Pre-operative recognition essential: plan dural repair, lumbar drain, or floating method
Surgical Approaches
- Posterior laminoplasty: K-line positive, multi-level, lordosis preserved; C5 palsy risk 5-15 percent
- Anterior corpectomy: K-line negative, focal disease, kyphosis; CSF leak and graft complications
- Floating method: thin OPLL with diamond burr, allow anterior migration; for dural ossification cases
- Combined approach: severe multi-level OPLL with kyphosis or failed prior surgery
Prognosis and Outcomes
- Best outcomes: K-line positive, mJOA greater than 12, myelopathy duration less than 12 months, no T2 signal
- Poor outcomes: K-line negative, mJOA less than 10, long-standing myelopathy, multi-level T2 signal change
- Duration of myelopathy is the most important modifiable prognostic factor
- OPLL progression rate 10-30 percent at 5 years post-operatively; no proven pharmacological prevention
Evidence Base and Key Trials
Ossification of the posterior longitudinal ligament of the cervical spine: etiology and natural history
- Comprehensive review of OPLL pathogenesis highlighting endochondral ossification driven by BMP signalling
- Japanese prevalence of 1.9 to 4.3 percent confirmed on population CT screening studies
- COL6A1 gene polymorphism identified as the strongest genetic association with OPLL
- Natural history: 1-3 percent annual risk of progression to symptomatic myelopathy in asymptomatic individuals
A new concept for making decisions regarding the surgical approach for cervical ossification of the posterior longitudinal ligament: the K-line
- K-line positive patients achieved significantly better neurological recovery after laminoplasty than K-line negative patients
- K-line negative patients had mean Japanese Orthopaedic Association recovery rate approximately 25 percentage points lower than K-line positive patients
- K-line provides a simple pre-operative radiographic tool for surgical approach selection
- K-line negative status predicted inadequate posterior shift of the spinal cord on post-operative MRI
Anterior cervical corpectomy and fusion versus posterior laminoplasty for the treatment of oppressive myelopathy owing to cervical ossification of posterior longitudinal ligament: a meta-analysis
- Anterior corpectomy and fusion provided significantly greater Japanese Orthopaedic Association (JOA) improvement than posterior laminoplasty for OPLL myelopathy
- Anterior approach had higher complication rates, particularly CSF leak and dysphagia, compared to posterior laminoplasty
- Posterior laminoplasty had shorter operative time, lower blood loss, and fewer overall complications
- No significant difference in fusion rate or long-term neurological recovery between approaches
Significance of the double-layer and single-layer signs in the ossification of the posterior longitudinal ligament of the cervical spine
- The double-layer sign (two ossified layers with intervening hypodense band on axial CT) and single-layer sign are key predictors of dural ossification in OPLL
- CSF leak occurred significantly more often in patients with positive CT signs of dural ossification compared to those without
- Pre-operative recognition of these CT signs allows surgical planning to include the floating method rather than direct OPLL resection
- The double-layer sign had higher specificity for intra-operative dural defect than the single-layer sign