Physis | articular surface | CT | 2 mm threshold | growth surveillance
Working Groups
Critical Must-Knows
- The distal tibial physis closes asymmetrically. Central closure occurs first, then medial, then lateral; this creates Tillaux and triplane patterns.
- Plain radiographs can underestimate displacement. CT is important for intra-articular and transitional fractures.
- Greater than 2 mm intra-articular gap or step is the practical threshold for anatomical reduction in Tillaux, triplane and SH-III/IV patterns.
- Repeated forceful reductions can harm the physis. If tissue blocks reduction, change strategy rather than persist.
- Growth arrest is not rare in high-risk patterns. Medial malleolus and high-energy distal tibial physeal injuries need surveillance.
Clinical Pearls
- "Ask for AP, mortise and true lateral ankle views; add tibia/fibula views when proximal pain or syndesmotic concern exists.
- "Tillaux is an anterolateral epiphyseal avulsion by the anterior inferior tibiofibular ligament.
- "Triplane is a multiplanar SH-IV pattern: epiphyseal, physeal and metaphyseal components.
- "A medial malleolus SH-III/IV fracture is a growth-arrest risk even after apparently good reduction.
Do not read paediatric ankle fractures like adult ankle fractures
A child with an ankle fracture has a physis, partly closing growth plate and different failure points. The adult question is often syndesmosis and malleoli; the paediatric question is physis, articular surface, remaining growth, reduction quality and growth arrest.
At a Glance: What Decides Treatment?
| Clinical Question | What To Check | Why It Changes Management |
|---|---|---|
| Is the ankle safe? | Open injury, skin tenting, swelling, pulses, sensation, pain escalation and compartment concern. | Unsafe soft tissues or compartment concern override routine casting pathways. |
| Is the joint involved? | Mortise view, articular step or gap, SH-III/IV pattern, Tillaux or triplane fracture. | Intra-articular incongruity usually needs CT and anatomical reduction. |
| Is the physis displaced? | Displacement, angulation, rotation, residual gap and tissue interposition. | Displaced physeal injuries need reduction; blocked or unstable reductions may need fixation. |
| How much growth remains? | Chronological age, skeletal maturity, remaining distal tibial growth and fracture type. | Higher remaining growth increases the importance of growth-arrest surveillance and counselling. |
| Is this a transitional fracture? | Adolescent age, external rotation mechanism, anterolateral epiphyseal fragment or multiplanar triplane geometry. | CT planning determines whether casting, percutaneous fixation or open reduction is safest. |
Rapid Recall
CMLPhyseal closure | TILLTillaux | STEPSurgery threshold |
|---|---|---|
C Central first Initial distal tibial physeal closure begins centrally. | T Transitional age Occurs during asymmetric physeal closure. | S Step Articular step-off on CT. |
M Medial next Medial closure leaves lateral physis vulnerable. | I Intra-articular SH-III pattern through epiphysis and physis. | T Two millimetres Common decision threshold for intra-articular injury. |
L Lateral last Anterolateral fragment becomes the Tillaux fragment. | L Lateral fragment Anterolateral epiphyseal fragment. | E Epiphysis Epiphyseal screws should avoid crossing the physis where possible. |
L Ligament pull AITFL traction creates the fragment. | P Plan CT Plan screw trajectory and approach from CT. | |
Central, medial, lateral closure creates transitional patterns. | Tillaux is the lateral epiphyseal avulsion. | STEP greater than 2 mm usually needs anatomical reduction. |
Overview/Epidemiology
Paediatric ankle fractures account for about 5% of all paediatric fractures and the distal tibial physis is one of the most important lower-limb growth plates injured in children. Management is high-stakes because the same injury can affect the joint surface, the physis or both.
The typical presentation is a child or adolescent with ankle pain, swelling and inability to weight bear after a twisting injury, fall, sport injury or higher-energy trauma. The key is to avoid the adult-ankle shortcut. In children, the ligament may remain intact while the physis or epiphysis fails. In adolescents, asymmetric distal tibial physeal closure creates transitional injuries such as Tillaux and triplane fractures.
The safe management sequence is:
The Surgeon’s Sequence
| Step | Question | Action |
|---|---|---|
| Safety | Is there open injury, threatened skin, vascular compromise or compartment concern? | Escalate urgently before routine fracture planning. |
| Pattern | Is this fibular, distal tibial physeal, medial malleolus, Tillaux or triplane? | Classify by physis and joint involvement. |
| Imaging | Can plain radiographs define the joint surface and fracture geometry? | Use CT for intra-articular and transitional fractures. |
| Reduction | Is alignment, physis and articular surface acceptable? | Cast, reduce, percutaneously fix or open depending on displacement and stability. |
| Follow-up | Is there remaining growth or high-risk medial malleolus injury? | Monitor for physeal bar, angular deformity and leg-length difference. |
Surgically Relevant Anatomy
The distal tibial physis contributes meaningfully to tibial growth and closes in an asymmetric pattern. Central closure begins first, followed by medial closure, with lateral closure last. During this transition, the partially closed physis cannot dissipate rotational force evenly.
The anterior inferior tibiofibular ligament attaches to the anterolateral distal tibial epiphysis. When the medial physis is closing and the lateral physis remains open, external rotation can avulse the anterolateral epiphyseal fragment: the Tillaux pattern. If the fracture propagates through the epiphysis, physis and metaphysis in different planes, the result is a triplane fracture.
Medial malleolus SH-III and SH-IV fractures cross the epiphysis and physis and can damage the germinal layer. Even small residual displacement may matter because the medial distal tibial physis can form a physeal bar.
Distal tibia
Physis plus joint surface. Reduction must protect both growth and articular congruity.
Distal fibula
Often lower-risk, but do not miss syndesmotic injury, physeal displacement or associated distal tibial injury.
Medial malleolus
SH-III/IV medial injuries carry meaningful physeal-bar risk and need longer surveillance.
Pathophysiology
The injury pattern depends on the child's age, mechanism and stage of physeal closure.
Why The Fracture Pattern Occurs
| Mechanism | Typical Pattern | Management Consequence |
|---|---|---|
| Supination-inversion | Distal fibular physeal injury or medial distal tibial injury depending force and age. | Examine both malleoli; do not assume lateral pain means simple sprain. |
| External rotation in an adolescent | Tillaux or triplane fracture during asymmetric distal tibial physeal closure. | CT defines the fragment and articular displacement. |
| High-energy axial or rotational trauma | Displaced distal tibial physeal injury, SH-IV fracture or complex triplane pattern. | Higher risk of growth disturbance and worse functional outcome. |
| Direct medial injury | Medial malleolus SH-III/IV fracture. | Anatomical reduction and growth-arrest surveillance are central. |
| Ligament-equivalent failure | The physis fails before adult-style ligament rupture. | Treatment decisions must consider growth plate and remaining growth. |
Classification
Distal Tibial Physeal Groups
| Type | Pattern | Treatment Meaning |
|---|---|---|
| SH-I | Through the physis; may be radiographically subtle. | Treat displacement and clinical tenderness; follow if distal tibia involved. |
| SH-II | Physis plus metaphyseal fragment. | Closed reduction if displaced; open if tissue blocks reduction. |
| SH-III | Epiphyseal intra-articular fracture extending to physis. | CT and anatomical reduction if displaced. |
| SH-IV | Epiphysis, physis and metaphysis. | CT-defined reduction and fixation; growth arrest risk. |
| SH-V | Crush injury to physis, often diagnosed late. | High suspicion and growth surveillance. |
Clinical Assessment
History
Ask for mechanism, energy, ability to weight bear, exact pain location, time since injury, reduction attempt, open wound, skin tenting, paraesthesia and prior ankle injury. Sporting adolescents with external rotation mechanisms are the classic group for transitional fractures.
Examination
Look, Feel, Move
| Step | How To Do It | Positive Finding |
|---|---|---|
| Look | Inspect swelling, bruising, deformity, skin tenting, open wounds and foot position. | Threatened skin, open injury or marked deformity needs urgent reduction or operative escalation. |
| Feel | Palpate distal tibial physis, medial malleolus, lateral malleolus, syndesmosis, proximal fibula, base of fifth metatarsal and midfoot. | Focal physeal or medial malleolar tenderness changes imaging and follow-up. |
| Move | Assess active toe motion and gentle ankle motion only if safe; do not stress a displaced fracture. | Painful block or gross instability supports significant fracture or joint involvement. |
| Neurovascular | Check dorsalis pedis/posterior tibial pulses, capillary refill, sensation in superficial/deep peroneal, tibial, sural and saphenous distributions. | Document before and after reduction. |
| Compartment risk | Assess escalating pain, pain with passive toe stretch, tense compartments and analgesic requirement. | Compartment concern is an emergency even if the X-ray looks manageable. |
Differential Diagnosis
The trap in children is the radiographically subtle injury. A tender physis with a "normal" film is a fracture until proven otherwise, and a presumed sprain in a skeletally immature ankle should be treated with suspicion.
Differentiating the Paediatric Ankle Injury
| Diagnosis | Discriminating Features | How To Confirm or Exclude |
|---|---|---|
| Distal fibular SH-I | Focal physeal tenderness with a near-normal radiograph in a younger child after inversion. | Clinical diagnosis; treat tenderness over the physis as a fracture and review; MRI only if symptoms persist. |
| Lateral ligament sprain | Tenderness anterior to and below the malleolus rather than over the physis, usually an older adolescent. | More likely once the physis has closed; do not over-call sprain when physeal tenderness is present. |
| Tillaux fracture | Adolescent, external rotation, anterolateral epiphyseal tenderness. | Mortise radiograph plus CT for the anterolateral fragment and articular gap. |
| Triplane fracture | Adolescent with multiplanar pain; the metaphyseal fragment may be missed on the AP view. | CT defines epiphyseal, physeal and metaphyseal components. |
| Medial malleolus SH-III/IV | Medial joint-line tenderness, intra-articular line on the mortise view. | CT for displacement; flag for growth-arrest surveillance. |
| Osteochondral lesion of the talus | Persistent deep ankle pain, catching or effusion after a twist with normal alignment. | MRI; consider when symptoms outlast the expected fracture or sprain course. |
| Proximal fibula (Maisonneuve-type) | Proximal fibular tenderness with a syndesmotic or medial ankle injury. | Full-length tibia/fibula radiographs; check medial clear space and syndesmosis. |
Investigations
What to request
- AP, mortise and true lateral ankle radiographs.
- Tibia/fibula views if proximal fibular pain, high-energy mechanism, syndesmotic concern or Maisonneuve-type pattern is possible.
- Foot radiographs if midfoot, base of fifth metatarsal or talar tenderness is present.
- CT for suspected Tillaux, triplane, SH-III/IV, intra-articular displacement, unclear fracture geometry or pre-operative planning.
- MRI is not routine for clear fractures, but may help when radiographs are negative and symptoms remain disproportionate or when occult physeal injury is a concern.


How to interpret
Radiographic and CT Checklist
| Feature | How To Assess | Treatment Meaning |
|---|---|---|
| Mortise congruity | Check medial clear space, talar shift and joint line. | Incongruity suggests unstable or intra-articular injury. |
| Physeal displacement | Measure residual gap, translation and angulation after reduction. | Persistent gap may indicate periosteal/tissue interposition. |
| Articular step/gap | Measure on CT in coronal, sagittal and axial planes. | Greater than 2 mm is the common threshold for anatomical reduction. |
| Tillaux fragment | Look for anterolateral epiphyseal fragment attached to AITFL. | Screw trajectory is usually planned perpendicular to the fracture line while avoiding the physis when possible. |
| Triplane geometry | Define epiphyseal, physeal and metaphyseal components on CT. | Determines whether closed/percutaneous fixation is enough or open reduction is needed. |
| Medial malleolus | Assess SH-III/IV line and residual displacement. | High physeal-bar risk; reduction quality and follow-up matter. |
Management
Immediate Management
| Priority | Action | Reason |
|---|---|---|
| Analgesia and elevation | Control pain, elevate and splint. | Reduces swelling and allows safe reassessment. |
| Unsafe soft tissues | Urgent reduction for skin tenting or severe deformity; urgent theatre for open injury. | Prevents skin compromise and contamination complications. |
| Neurovascular check | Document pulses, capillary refill and sensation before and after reduction. | Identifies injury-related or iatrogenic deterioration. |
| Imaging after reduction | Repeat AP, mortise and lateral films after any reduction. | Confirms alignment and residual displacement. |
Operative Technique
Principles
The operation should reduce the joint surface, respect the physis, avoid repeated traumatic manipulation and provide enough stability for safe healing. CT determines the approach and screw trajectory in Tillaux and triplane injuries.
Technique by Pattern
| Operation | PIPADRAW Sequence | Pitfalls |
|---|---|---|
| Closed reduction and casting | Position supine; analgesia/anaesthesia; traction and reverse mechanism; check AP/mortise/lateral; cast; repeat films. | Repeated forceful attempts can injure the physis or soft tissues. |
| Percutaneous fixation | Supine; image intensifier AP/mortise/lateral; reduce closed; insert cannulated screw or K-wire according to fragment; confirm joint and physis. | Do not accept a poor reduction just because fixation is percutaneous. |
| Tillaux ORIF | Anterolateral approach if closed reduction fails; identify fragment; clear interposed tissue; reduce anterolateral epiphysis; fix with epiphyseal screw parallel to joint/physis where possible. | Screw trajectory must not enter the joint; CT planning is essential. |
| Triplane fixation | CT plan; reduce epiphyseal joint component first; fix epiphyseal fragment; then reduce/fix metaphyseal component if needed. | Treating only the metaphyseal fragment can leave the joint incongruent. |
| Medial malleolus fixation | Medial approach; protect saphenous structures; reduce SH-III/IV fragment anatomically; fix with screw trajectory planned to minimise physeal damage. | Residual displacement increases bar risk; follow-up is mandatory. |
Intra-operative reduction check
For Tillaux and triplane injuries, the operative endpoint is not just a screw in bone. The endpoint is a congruent mortise, less than 2 mm residual articular displacement, stable fixation and a documented plan for growth follow-up.
Post-Operative Care and Rehabilitation
Aftercare
| Situation | Typical Plan | What To Monitor |
|---|---|---|
| Cast treatment | Non-weight bearing initially, then progress according to pain, healing and local protocol. | Loss of reduction, pain, swelling and late growth disturbance. |
| Percutaneous fixation | Protected non-weight bearing, wound/pin review if relevant, radiographs. | Reduction maintenance, hardware symptoms and healing. |
| ORIF | Below-knee immobilisation, non-weight bearing until early healing, then progressive motion. | Joint congruity, screw position, infection, stiffness and physeal bar. |
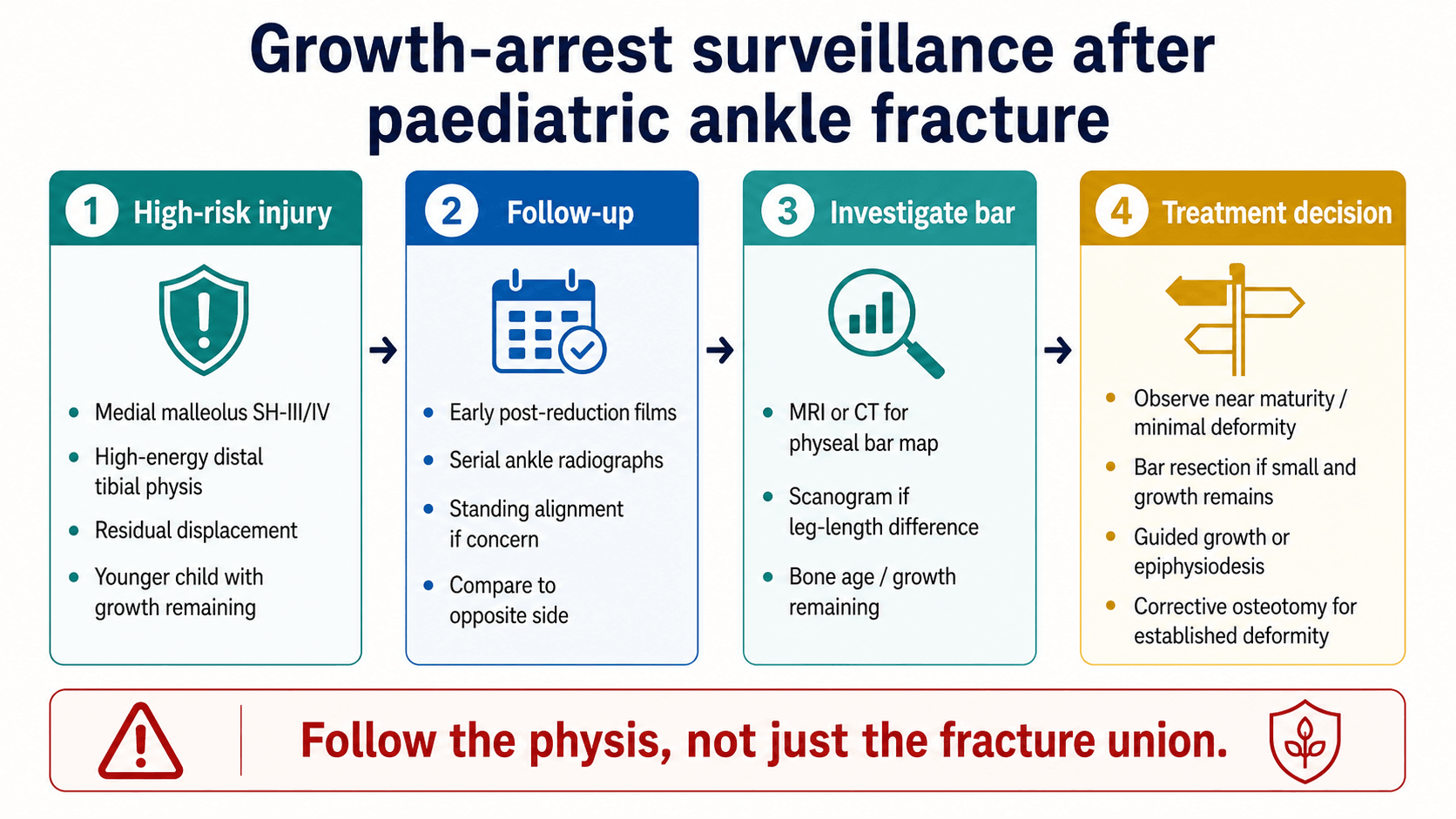
| High growth remaining | Serial standing alignment and ankle radiographs. | Physeal bar, angular deformity and leg-length difference. |
Children with intra-articular displacement, high-energy trauma, medial malleolus injury or meaningful remaining growth should not disappear after fracture union. They need a surveillance plan until growth arrest risk is acceptably low.
Complications and Failure Management
Complications
| Complication | Risk Pattern | Management |
|---|---|---|
| Physeal bar / growth arrest | Medial malleolus SH-III/IV, high-energy distal tibial physis, residual displacement. | Serial radiographs; consider bar resection, guided growth, epiphysiodesis or osteotomy depending bar size and growth remaining. |
| Angular deformity | Partial distal tibial arrest. | Measure mechanical/anatomic axis and ankle orientation; guided growth or osteotomy if progressive/significant. |
| Leg-length difference | Complete or partial arrest with meaningful remaining growth. | Scanogram, bone age and prediction; shoe raise, epiphysiodesis or length correction depending magnitude. |
| Post-traumatic arthritis | Residual intra-articular incongruity after SH-III/IV, Tillaux or triplane fracture. | Prevention is anatomical reduction; established arthritis is managed symptomatically or reconstructively. |
| Stiffness | Prolonged immobilisation or intra-articular injury. | Motion after healing, physiotherapy and gradual return to activity. |
| Compartment syndrome | High-energy injury, severe swelling, displaced distal tibial injury. | Emergency recognition and fasciotomy if diagnosed. |
Evidence Signals
Guidelines to management
- Paediatric ankle fractures represent about 5% of all paediatric fractures.
- Distal tibial physeal injuries account for approximately 15-20% of all physeal injuries.
- CT is recommended with low threshold for suspected intra-articular or transitional fractures.
- Intra-articular displacement greater than 2 mm needs anatomical reduction and stabilisation.
Physeal ankle fracture review
- Distal tibial physeal fractures require attention to growth arrest risk.
- Classification, displacement and remaining growth guide treatment.
- Anatomic reduction is central for intra-articular patterns.
Dias-Tachdjian classification (landmark)
- Analysed 71 paediatric ankle fractures and proposed a mechanism-based classification by foot position and direction of force.
- Supination-inversion was the commonest mechanism, present in almost half of cases.
- Correlation with the Salter-Harris system is essential because varus deformity is common after SH-III and SH-IV injuries.
Controversies and Areas of Uncertainty
Examiners reward a candidate who can hold a clear default position while acknowledging genuine debate. The honest answer to most of these is anatomical reduction of the displaced joint, with the nuance below.
Where the Evidence Is Still Debated
| Question | What Is Agreed | What Remains Uncertain |
|---|---|---|
| How much residual gap is acceptable? | Greater than 2 mm displacement on CT is the practical threshold for anatomical reduction. | Outcomes data (Choudhry/Crawford) suggest displacement under about 2.5 mm after sound reduction is tolerated; the safe upper limit is not defined. |
| Closed percutaneous versus open fixation for triplane? | The articular surface must be congruent however it is achieved. | Closed reduction with percutaneous screws gives good results when reduction is perfect, but the threshold to convert to open is judgement-based. |
| Is CT needed for every transitional fracture? | CT is standard for SH-III/IV, Tillaux and triplane planning. | Radiation stewardship versus information gain in clearly undisplaced patterns; some centres use limited-sequence MRI. |
| Should screws cross the physis? | Avoid crossing the physis where the geometry allows. | In transitional fractures the physis is closing, so a transphyseal screw is often acceptable; in young children it is avoided. |
| How long to follow for growth arrest? | Medial malleolus SH-III/IV and high-energy distal tibial injuries need prolonged surveillance. | Optimal frequency and total duration vary; at least 12 months is supported for medial malleolus injuries, longer with substantial growth remaining. |
Guidelines, Registries & Global Practice
Global epidemiology
Paediatric ankle fractures account for about 5% of all paediatric fractures, and distal tibial physeal injuries make up roughly 15-20% of all physeal injuries, making the distal tibia the most commonly injured lower-limb physis in children. Transitional fractures (Tillaux and triplane) cluster in the roughly 18-month window before physeal closure, which completes at about 14 years in girls and 16 years in boys. Boys are affected more often overall; girls sustain transitional fractures at a younger age than boys.
Side-by-side guidance
There is no single global ankle-specific paediatric guideline; practice is built from major-society principles plus the paediatric trauma literature. The points below describe how the relevant bodies frame the same problem.
How Major Bodies Frame Paediatric Ankle and Physeal Injury
| Body / Source | Emphasis | Practical Position |
|---|---|---|
| AO Foundation (Paediatric) | Mechanism, Salter-Harris pattern and physis-sparing fixation. | Anatomical reduction of intra-articular fragments; implants chosen to minimise physeal injury; CT for transitional patterns. |
| AAOS / POSNA literature (US) | Classification-driven management and growth-arrest risk. | Low threshold for CT in intra-articular and transitional fractures; surveillance for premature physeal closure. |
| BOA / BOAST (UK, paediatric trauma principles) | Timely senior-led care, neurovascular documentation and open-fracture pathways. | Soft-tissue and neurovascular assessment first; defined escalation for open or deformed injuries. |
| EFORT / European paediatric trauma consensus | Standardised physeal-injury assessment and follow-up. | Reduce the joint, protect the physis and follow to skeletal maturity in high-risk patterns. |
Registries
Unlike arthroplasty, paediatric ankle fractures are not tracked by implant registries; the evidence base is observational cohorts and systematic reviews (for example the 2025 triplane review pooling 34 studies). National paediatric trauma networks and major-trauma audits, rather than implant registries, are the closest surveillance structures.
High-resource versus limited-resource practice
Practice Variation by Setting
| Element | Well-resourced setting | Limited-resource setting |
|---|---|---|
| Imaging | CT routine for transitional and SH-III/IV fractures; MRI available for occult injury. | Reliance on good-quality mortise and lateral radiographs; intra-operative arthrogram or image intensifier to judge congruity. |
| Fixation | Cannulated screws and image intensifier readily available. | K-wires and careful closed reduction where screws are scarce; sound reduction still prioritised. |
| Follow-up | Structured growth-arrest surveillance to maturity. | Surveillance limited by access; clear safety-netting and return advice become essential. |
Clinical Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 14-year-old has lateral ankle pain after an external rotation injury. X-rays suggest a Tillaux fracture. CT shows 1.5 mm articular gap."
"A 13-year-old has a triplane ankle fracture. CT shows a displaced epiphyseal component with 4 mm joint step and a metaphyseal fragment."
"A 10-year-old has a displaced medial malleolus SH-III fracture. It is reduced and fixed. At five months the radiograph shows asymmetric physeal closure."
Paediatric Ankle Fractures: Decision Sheet
Clinical summary
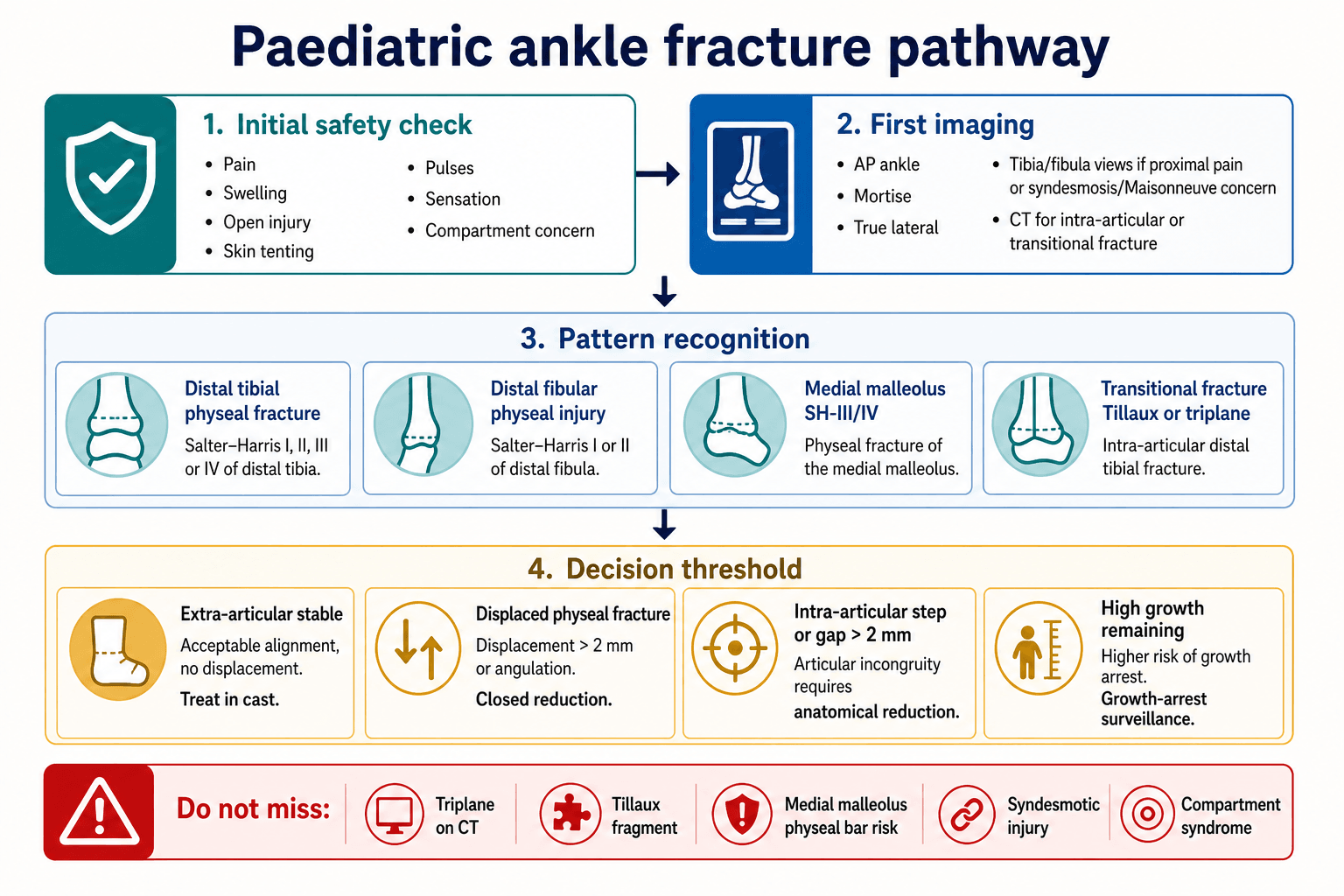
Assess
- •Check skin, swelling, pulses, sensation and compartment risk.
- •Order AP, mortise and true lateral ankle radiographs.
- •Add tibia/fibula views for proximal pain or syndesmotic concern.
Image
- •Use CT for Tillaux, triplane, SH-III/IV or unclear intra-articular displacement.
- •Measure articular step and gap on CT.
- •Look specifically at the medial malleolus and distal tibial physis.
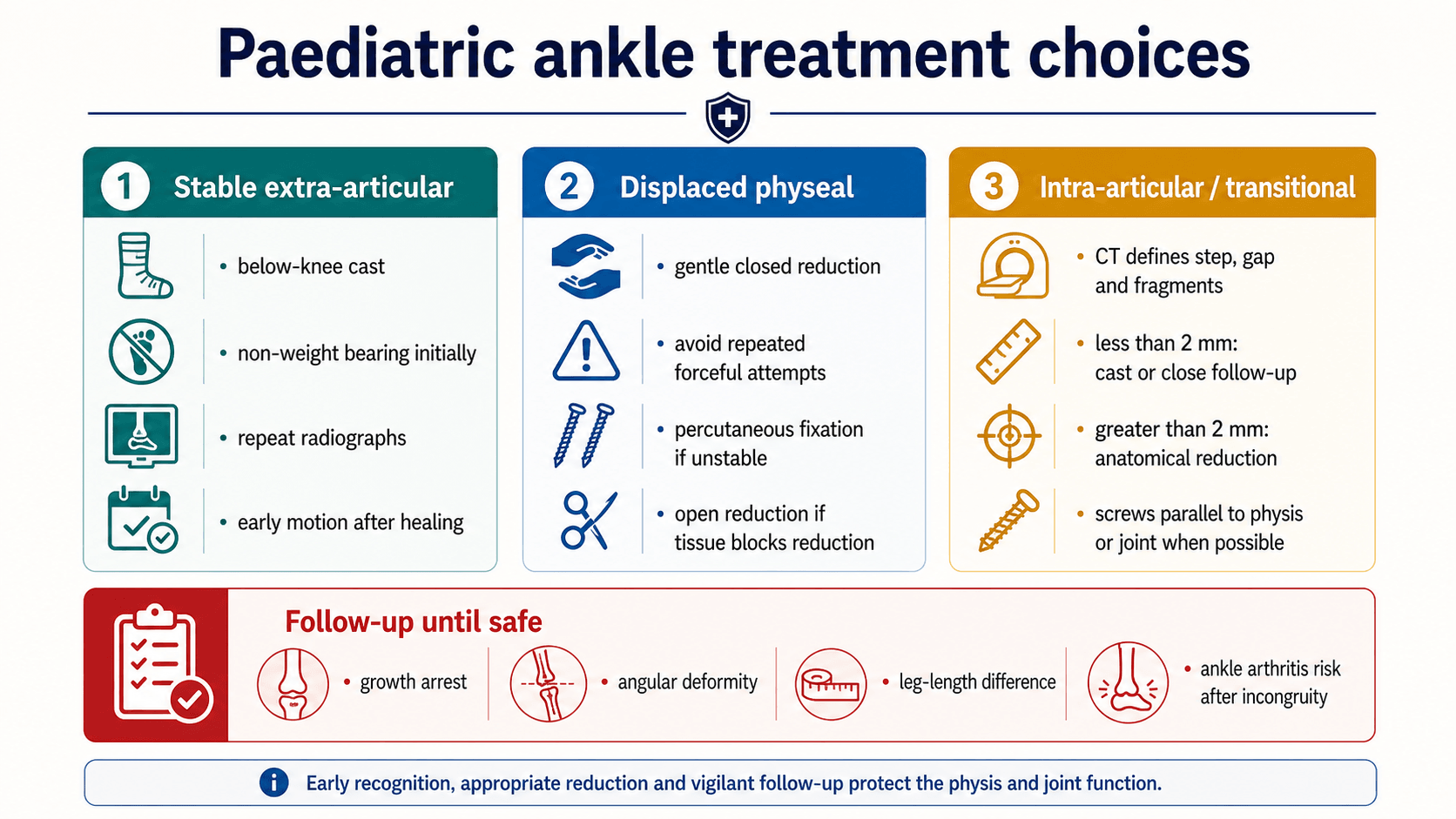
Treat
- •Stable extra-articular injuries can usually be casted.
- •Displaced physeal injuries need gentle reduction; fixation if unstable or blocked.
- •Intra-articular/transitional injuries greater than 2 mm usually need anatomical reduction.
Follow
- •Monitor high-risk injuries for growth arrest.
- •Medial malleolus SH-III/IV injuries need prolonged surveillance.
- •Treat physeal bar according to bar size, deformity and remaining growth.