Treat the child first, then classify the pelvis or hip injury and the risk it creates
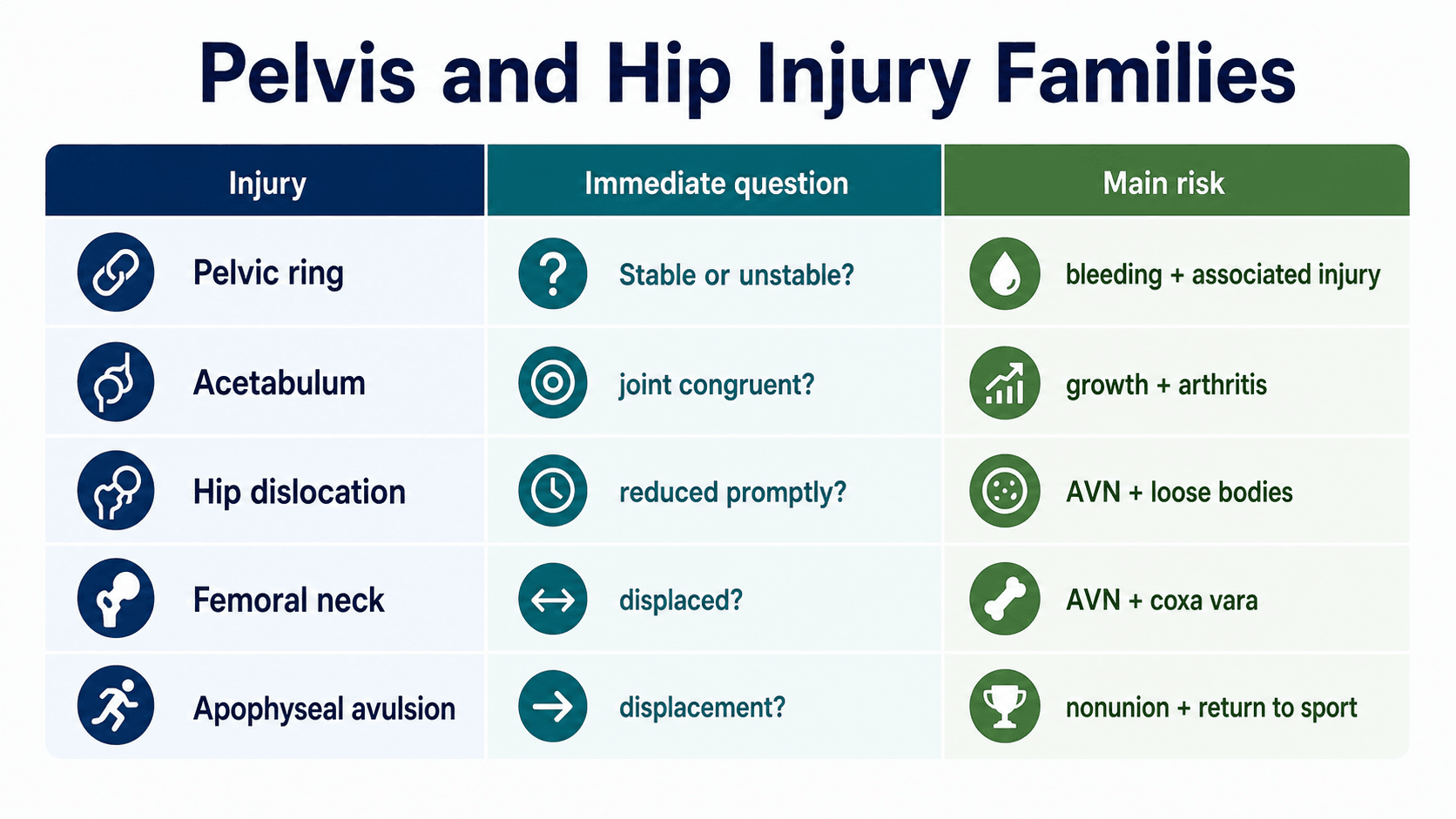
- Paediatric pelvis and hip trauma is not one diagnosis; it is a set of injury families with different priorities.
- The child with a pelvic ring injury may have abdominal, urogenital, vascular, head, chest or spine injury.
- A paediatric traumatic hip dislocation needs prompt reduction and post-reduction imaging.
- A displaced paediatric femoral neck fracture is a high-risk injury requiring urgent senior planning.
- Pelvic apophyseal avulsions are common in adolescent athletes and should not be confused with malignancy or infection when the history is acute and mechanical.
- “Do not let an obvious limb posture distract from primary survey and associated injury screening.
- “After hip dislocation reduction, a concentric reduction is not enough; look for loose bodies, femoral head injury and acetabular injury.
- “Delbet type, displacement and reduction quality matter more than the generic phrase hip fracture.
- “Low-energy femoral neck fracture in a child should trigger pathology or bone fragility thinking.
- “Apophyseal avulsion treatment is decided by displacement, function, sport demand, symptoms and chronicity.
Paediatric Pelvis and Hip Trauma
High-energy pelvic and hip trauma can coexist with abdominal injury, urogenital injury, head injury, spine injury and other limb fractures. Stabilise the child and define associated injuries before focusing on definitive orthopaedic reconstruction.
Overview and Epidemiology
Paediatric pelvis and hip trauma ranges from common sports-related apophyseal avulsion to rare, high-risk injuries such as traumatic hip dislocation, acetabular fracture and paediatric femoral neck fracture. The child's pelvis has open physes, apophyses, thick periosteum, relatively elastic bone and important growth centres. These features change fracture patterns and complications.
The mechanism matters. Low-energy adolescent sprinting or kicking injury suggests apophyseal avulsion. Fall from height, road trauma or crush injury should raise concern for pelvic ring injury, acetabular injury, hip dislocation, femoral neck fracture and associated injuries. A low-energy femoral neck fracture, especially without a clear major trauma mechanism, should prompt assessment for tumour-like lesion, metabolic bone disease, endocrine disease, infection or non-accidental injury in the right clinical setting.
Anatomy and Biomechanics
The paediatric pelvis and hip contain multiple growth-related weak points. The triradiate cartilage contributes to acetabular growth and is important in acetabular trauma. The proximal femoral physis, femoral neck and greater trochanteric apophysis influence proximal femoral growth and alignment. Pelvic apophyses are traction sites for powerful muscles, so adolescent athletes can sustain avulsion fractures through the physis or apophysis before the tendon fails.
The femoral head blood supply is vulnerable in paediatric femoral neck fractures and traumatic hip dislocation. Displacement, fracture location, intracapsular pressure and reduction quality all contribute to AVN risk. This is why the same child who otherwise heals fractures well can have devastating sequelae after proximal femoral trauma.
- Why it matters
- Acetabular growth centre
- Clinical implication
- Displaced acetabular injury can cause growth disturbance and incongruity
- Why it matters
- Vulnerable after dislocation and femoral neck fracture
- Clinical implication
- Reduction timing, reduction quality and long follow-up matter
- Why it matters
- Growth and head-neck relationship
- Clinical implication
- Transphyseal injury has high concern for AVN and growth arrest
- Why it matters
- Traction weak points in adolescents
- Clinical implication
- ASIS, AIIS, ischial tuberosity, iliac crest and lesser trochanter can avulse
- Why it matters
- Children can have major internal injury with subtle bony injury
- Clinical implication
- Do not rely on fracture displacement alone to judge trauma severity
The topic flags that triradiate cartilage injury causes growth disturbance, but the examinable framework is the Bucholz classification, which applies the Salter-Harris concept to this acetabular growth plate and predicts who develops acetabular dysplasia from premature closure:
- Bucholz Type I (Salter-Harris I/II pattern): the fracture runs through the hypertrophic zone, sparing the germinal layer - growth potential is preserved, so the prognosis for continued acetabular growth is good.
- Bucholz Type II (Salter-Harris IV pattern): the fracture crosses the germinal/metaphyseal portion - higher risk of bony bridge and growth arrest.
- Bucholz Type V (Salter-Harris V - crush): a compression/crush injury of the triradiate cartilage - the worst prognosis, often radiographically occult initially, leading to premature triradiate closure, a shallow dysplastic acetabulum, progressive subluxation and early arthritis, especially in the young child (under about ten years) who has the most growth remaining.
Why it matters: a crush (Type V) injury can look unremarkable on the initial film yet cause a maldeveloped acetabulum years later, so these children need long-term surveillance for acetabular dysplasia/subluxation and may need later reconstructive osteotomy.
Exam point: classify acetabular growth-plate trauma by Bucholz - the crush (Type V) injury in a young child is the dangerous one, causing premature triradiate closure and acetabular dysplasia, and mandating long growth surveillance even when early films look benign.
Pathophysiology
Pelvic ring injuries occur when force overcomes ring elasticity and ligamentous restraint. Stable injuries may involve isolated pubic rami or iliac wing fractures. Unstable patterns can involve anterior and posterior ring disruption, vertical displacement, bleeding and major associated injury. In children, haemodynamic instability is often from associated injury rather than pelvic bleeding alone, but severe pelvic haemorrhage still occurs.
Traumatic hip dislocation occurs when force drives the femoral head out of the acetabulum. Posterior dislocation is classically associated with dashboard-type mechanisms, but children can dislocate with lower energy because their soft tissues are more elastic. The longer the hip remains dislocated, the greater the concern for femoral-head perfusion and chondral injury.
Paediatric femoral neck fractures are uncommon but dangerous. The fracture line, displacement and treatment can compromise femoral-head perfusion, and poor reduction or inadequate fixation can produce nonunion or coxa vara. Apophyseal avulsions are traction injuries: the muscle-tendon unit pulls off an apophyseal fragment during sprinting, kicking or sudden eccentric contraction.
Classification Systems
- Examples
- Rami, iliac wing, APC, LC, vertical shear, complex ring injury
- Treatment-driving feature
- Haemodynamics, posterior ring stability and associated injury
- Examples
- Wall, column, transverse, triradiate cartilage involvement
- Treatment-driving feature
- Joint congruity, displacement and growth risk
- Examples
- Posterior, anterior, inferior, fracture-dislocation
- Treatment-driving feature
- Time to reduction, concentricity and loose bodies
- Examples
- Delbet I to IV
- Treatment-driving feature
- Location, displacement, verticality and vascular risk
- Examples
- ASIS, AIIS, ischial tuberosity, iliac crest, lesser trochanter
- Treatment-driving feature
- Displacement, sport demand, chronicity and nerve symptoms
For the pelvic ring the topic borrows adult terms (APC/LC/vertical shear), but the examinable paediatric scheme is the Torode and Zieg classification, which stratifies by stability and the risk of associated injury and bleeding:
- Type I - avulsion fracture: apophyseal avulsion of the bony pelvis (e.g. ASIS, AIIS, ischium) - benign, the sports injury family above.
- Type II - iliac wing fracture: from a direct lateral force (including iliac apophyseal avulsion/"bucket-handle"-type) - generally stable.
- Type III - simple ring fracture: a stable ring injury (e.g. pubic rami, or a ring fracture without an unstable segment) - the ring is not unstable.
- Type IV - ring disruption (unstable): an unstable ring - bilateral pubic (straddle) fractures, anterior and posterior ring disruption, or a fracture involving the acetabulum. This group carries the highest energy, transfusion, associated-injury and mortality risk.
The revised Torode-Zieg splits Type III into IIIa (stable, isolated anterior ring) and IIIb (anterior ring fracture with a non-displaced posterior ring injury) because IIIb behaves with more morbidity than a truly isolated anterior fracture.
Exam point: classify a child's pelvic ring injury by Torode-Zieg (I avulsion / II iliac wing / III stable ring / IV unstable ring-disruption) - Type IV is the resuscitation-and-associated-injury group, and the revised IIIa/IIIb split recognises that an occult posterior injury raises the risk.
Clinical Assessment
Start with primary survey, analgesia and immobilisation. In high-energy trauma, ask about mechanism, speed, height, crush, seatbelt, pedestrian impact, loss of consciousness, abdominal pain, urinary symptoms, perineal pain, neurological symptoms and pain in other limbs. Document haemodynamic status, abdominal findings, perineal bruising, blood at urethral meatus, rectal tone when indicated, lower-limb neurological function and distal perfusion.
For hip dislocation, document limb position and sciatic nerve function before reduction if this does not delay urgent care. For femoral neck fracture, avoid repeated painful movement. For apophyseal avulsion, the history is usually a sudden sport-related pop or sharp pain at a specific apophyseal site, followed by difficulty running or kicking.
- Look for
- Pelvic pain, instability, abdominal tenderness, perineal bruising
- Specific documentation
- Haemodynamics, associated injuries, urogenital signs, neurology
- Look for
- Fixed hip posture, severe pain, shortening
- Specific documentation
- Sciatic nerve function before and after reduction
- Look for
- Groin pain, inability to weight bear, painful log roll
- Specific documentation
- Avoid forceful motion; document distal neurovascular status
- Look for
- Local tenderness at ASIS, AIIS, ischium or iliac crest
- Specific documentation
- Sport mechanism, displacement symptoms, hamstring or hip flexor weakness
Screen for abdominal injury, urogenital injury, head injury, chest injury, spine injury, femoral shaft fracture, knee injury and open wounds. A pelvic fracture in a child is a marker of significant trauma until proven otherwise.
- Discriminating features
- Clear mechanism, acute onset, focal bony tenderness, often able to localise
- Key investigation
- Radiographs then CT or MRI as indicated
- Discriminating features
- Adolescent, often overweight, groin or referred knee pain, obligatory external rotation on flexion, minor or no trauma
- Key investigation
- AP and frog-lateral pelvis radiographs
- Discriminating features
- Fever, refusal to weight bear, raised inflammatory markers, hip held flexed and externally rotated, no clear trauma
- Key investigation
- Inflammatory markers, ultrasound, aspiration, MRI
- Discriminating features
- Insidious limp in younger child, painless or mild pain, no acute trauma
- Key investigation
- Radiographs, MRI for early disease
- Discriminating features
- Low-energy mechanism, lytic or sclerotic lesion, pain preceding injury
- Key investigation
- Radiographs, MRI, oncology or metabolic workup
- Discriminating features
- Inconsistent history, delayed presentation, injury not matching developmental stage
- Key investigation
- Skeletal survey, safeguarding referral
- Discriminating features
- Gradual onset, tenderness without fracture, normal radiographs
- Key investigation
- Clinical diagnosis, MRI if uncertain
A child with hip pain, fever and refusal to weight bear is septic arthritis until proven otherwise; do not anchor on a minor trauma history. Conversely, a low-energy femoral neck fracture should prompt a search for an underlying lesion, metabolic bone disease or non-accidental injury.
Investigations
Initial imaging usually includes AP pelvis in trauma, plus targeted hip and femur views if pain localises to the hip or proximal femur. CT is used for pelvic ring displacement, acetabular fracture, posterior wall injury, intra-articular fragments, post-reduction hip dislocation assessment and complex trauma planning. MRI is useful for occult injury, chondral injury, femoral-head perfusion concern, marrow oedema, labrum, soft tissue and occult femoral neck fracture.
In apophyseal avulsion, plain radiographs often diagnose displaced fragments. MRI is useful when radiographs are negative but symptoms strongly localise to an apophysis, or when differentiating avulsion from infection or tumour-like conditions.
- Investigation
- AP pelvis and targeted radiographs
- Reason
- Fast initial classification and fracture screening
- Investigation
- CT with reconstructions
- Reason
- Defines posterior ring, acetabulum, joint congruity and fragments
- Investigation
- Post-reduction radiographs plus CT or MRI when indicated
- Reason
- Detects loose bodies, fragments and incongruity
- Investigation
- MRI and targeted laboratory or tumour workup where indicated
- Reason
- Avoids missing stress, pathological or infection-related fracture
- Investigation
- MRI
- Reason
- Shows oedema, avulsion and soft-tissue injury
Management Decisions
Stable pelvic ring injuries are usually treated with analgesia, protected weight-bearing and mobilisation. Unstable injuries require trauma-team resuscitation, haemorrhage control, pelvic binder or external stabilisation when indicated, and specialist fixation planning.
- Treatment direction
- Analgesia, mobilisation as tolerated or protected weight-bearing
- Key check
- Associated injury still needs screening
- Treatment direction
- Primary survey, transfusion strategy, binder if appropriate, operative or interventional control
- Key check
- Bleeding may be pelvic, abdominal or both
- Treatment direction
- Specialist pelvic fixation planning
- Key check
- CT-based classification and growth-aware implants
- Treatment direction
- Antibiotics, debridement, contamination control and multidisciplinary care
- Key check
- Perineal, rectal and urogenital injury
Surgical Technique
Technique depends on the injury family. The common principle is that paediatric fixation should restore alignment and stability while respecting growth plates, cartilage, soft-tissue envelope and future growth.
- Core steps
- Position on radiolucent table, obtain AP and lateral imaging, reduce anatomically, fix with screws or plate construct depending age and pattern
- Critical technical points
- Avoid joint penetration, avoid physeal damage when possible, compress fracture and protect blood supply
- Core steps
- Use approach that allows direct reduction, clear interposed tissue, reduce under vision, confirm fluoroscopically
- Critical technical points
- Do not accept varus or rotational malreduction
- Core steps
- Indicated for irreducible dislocation, incarcerated fragment or nonconcentric reduction
- Critical technical points
- Avoid repeated closed-force attempts; inspect and remove obstacles
- Core steps
- Specialist approach based on fracture and triradiate involvement
- Critical technical points
- Aim for congruent joint while minimising growth-plate injury
- Core steps
- Direct approach to fragment, protect nearby nerves, reduce and fix with screw or suture construct
- Critical technical points
- Do not overtreat small avulsions; ischial tuberosity requires sciatic nerve awareness

Complications
Avascular necrosis is the feared complication after paediatric femoral neck fracture and traumatic hip dislocation. It can present late, so early normal imaging is not enough.
Triradiate cartilage injury, proximal femoral physeal injury and pelvic growth asymmetry can produce deformity or early arthritis.
Urogenital injury, abdominal injury, head injury, spine injury and ipsilateral limb injuries are high-value misses in high-energy trauma.
Persistent pain, coxa vara, nonunion, stiffness, chondrolysis, nerve injury and failure to return to sport can matter more to the child than radiographic union alone.
- Prevention strategy
- Prompt hip reduction, anatomical femoral neck reduction, stable fixation
- Surveillance
- Serial radiographs and clinical review over time
- Prevention strategy
- Avoid varus reduction and unstable fixation
- Surveillance
- Neck-shaft angle and gait follow-up
- Prevention strategy
- Adequate reduction, compression and protected loading
- Surveillance
- Pain, radiographs and CT when union uncertain
- Prevention strategy
- Restore joint congruity and remove loose bodies
- Surveillance
- Pain, range and imaging as symptoms evolve
- Prevention strategy
- Identify displaced/high-demand injuries and rehabilitate progressively
- Surveillance
- Persistent pain and sport limitation
Postoperative Care
Postoperative care must match stability and biology. Pelvic ring injuries need pain control, mobilisation planning, venous thromboembolism risk assessment in adolescents, skin care and associated injury care. Hip dislocation follow-up includes range, pain, weight-bearing progression and surveillance for AVN. Femoral neck fracture care requires protected weight-bearing, serial radiographs, monitoring for joint penetration or loss of fixation, and long-term review for AVN, coxa vara, nonunion and growth disturbance.
- Early follow-up
- Pain, mobility, associated injuries, stability
- Late follow-up
- Asymmetry, gait, chronic pain
- Early follow-up
- Concentric reduction, fragments, nerve recovery
- Late follow-up
- AVN, chondrolysis, stiffness
- Early follow-up
- Reduction, fixation, protected loading
- Late follow-up
- AVN, coxa vara, nonunion, growth disturbance
- Early follow-up
- Pain control and gait
- Late follow-up
- Return to sport, nonunion, persistent weakness
Outcomes and Prognosis
Stable pelvic ring injuries and minimally displaced apophyseal avulsions usually do well with non-operative care and rehabilitation. Unstable pelvic injuries, acetabular injuries, hip dislocations and femoral neck fractures have outcome risk because they involve joint congruity, femoral-head perfusion, growth centres and associated trauma.
Poor prognostic features include delayed hip reduction, nonconcentric reduction, associated femoral head or acetabular fracture, displaced Delbet I or II femoral neck fracture, poor reduction quality, unstable fixation, triradiate cartilage injury, high-energy polytrauma and delayed diagnosis of apophyseal avulsion with nonunion.
Guidelines, Registries & Global Practice
Paediatric pelvic ring fractures account for roughly 1 to 5 percent of all paediatric fractures and well under 1 percent of paediatric fractures involve the acetabulum or femoral neck. Traumatic hip dislocation in children is rare; in younger children it can follow low-energy trauma because of soft-tissue elasticity, whereas adolescents typically need high-energy mechanisms. These are uncommon injuries, so high-quality randomised data are scarce and most guidance derives from cohort studies, registries and expert consensus.
- Focus
- Polytrauma sequence
- Practical recommendation
- Treat the child first: airway, breathing, circulation and haemorrhage control precede definitive fracture care; a paediatric pelvic fracture is a marker of major trauma
- Focus
- Paediatric femoral neck fracture and hip dislocation
- Practical recommendation
- Urgent anatomical reduction and stable fixation for displaced necks; prompt reduction of dislocations with post-reduction cross-sectional imaging
- Focus
- Major trauma in children and non-accidental injury
- Practical recommendation
- Network-based major-trauma pathways, senior decision-making, low threshold for safeguarding assessment in low-energy or inconsistent injuries
- Focus
- Fixation principles
- Practical recommendation
- Growth-aware fixation that respects physes and triradiate cartilage while achieving stable, anatomical reduction
- Focus
- Apophyseal avulsion and acetabular injury
- Practical recommendation
- Predominantly non-operative avulsion care with selective fixation; specialist planning for displaced acetabular and triradiate injuries
Registry evidence specific to paediatric pelvis and hip trauma is limited because implant survival registries (NJR, AOANJRR, AJRR, the Swedish and Norwegian registries) are built around arthroplasty rather than paediatric fracture fixation. Population-based trauma registries and large single-centre series therefore carry the epidemiological weight, and they consistently show that displacement, Delbet type, reduction quality and associated injuries — not geography — determine outcome.
- Typical pathway
- On-site paediatric orthopaedics, CT/MRI, interventional radiology and intensive care
- Pragmatic priority
- Early cross-sectional imaging, definitive fixation and structured AVN surveillance
- Typical pathway
- Initial stabilisation then transfer
- Pragmatic priority
- Resuscitate, control pain, obtain essential radiographs, avoid repeated forceful reduction and discuss early transfer
- Typical pathway
- Plain radiographs, limited CT/MRI, restricted implant range
- Pragmatic priority
- Prioritise prompt hip reduction and life-saving haemorrhage control; manage displaced necks and acetabular injuries with the best available stable fixation and clinical follow-up
Across all settings the common thread is the same: stabilise the child, classify the injury family, achieve prompt and accurate reduction of the hip and femoral neck, respect growth centres, and commit to long-term avascular-necrosis and growth surveillance. Where local expertise or imaging is lacking, early discussion and transfer beat repeated reduction or fixation attempts.
References
- 1Berdini M, Procaccini R, Carola D, Marinelli M, Gigante A. "Modified Stoppa Approach for ORIF of a Paediatric Transverse Acetabular Fracture: Case Report and Systematic Review of Internal Fixation in Children". Children. 2026PubMed
- 2Dong B, Li F, Li C. "Risk factors for avascular necrosis in pediatric femoral neck fractures: a systematic review and meta-analysis". Journal of Orthopaedic Surgery and Research. 2025PubMed
- 3Chen YP, Lin CH, Hong CK, Yao SH, Chen CH. "Plate Versus Screw Fixation in Treating Pediatric Femoral Neck Fractures: A Systematic Review". Journal of Pediatric Orthopedics. 2026PubMed
- 4De Salvo S et al.. "Radiological, clinical and functional outcome of children with traumatic hip dislocation: a multicenter review of 66 cases". Archives of Orthopaedic and Trauma Surgery. 2025PubMed
- 5Lu Y et al.. "Iatrogenic femoral neck fractures or separation of the proximal femoral epiphysis during closed reduction of irreducible femoral head fracture-dislocations in children: a review of 12 cases". Journal of Orthopaedics and Traumatology. 2026PubMed
- 6Molina LL et al.. "Outcomes of Conservative Versus Surgical Treatment of Adolescent Pelvic and Hip Avulsion Fractures: A Systematic Review and Meta-Analysis". Journal of Pediatric Orthopedics. 2026PubMed
- 7Ferraro SL et al.. "Acute Pelvic and Hip Apophyseal Avulsion Fractures in Adolescents: A Summary of 719 Cases". Journal of Pediatric Orthopedics. 2023PubMed
- 8Van Wagoner C et al.. "Associated Urogenital Injuries Following Pelvic Trauma in Pediatrics: A 15-Year Single-Center Retrospective Study". Cureus. 2026PubMed
Controversies and Areas of Uncertainty
Because these injuries are rare, much of practice rests on cohort data and expert opinion rather than randomised trials. Several genuine areas of debate recur in vivas.
- The debate
- Older teaching urged reduction within 6 to 24 hours; recent meta-analysis found no overall association with timing, though delayed reduction worsened long-term AVN in subgroup analysis
- Pragmatic position
- Still reduce urgently: displacement and reduction quality dominate, but avoidable delay is hard to defend
- The debate
- Some series favour closed reduction and internal fixation for lower AVN; others argue open reduction guarantees anatomical alignment
- Pragmatic position
- Accept a high-quality closed reduction; convert to open reduction rather than accept varus, rotation or persistent displacement
- The debate
- Capsulotomy or aspiration may lower intracapsular pressure and theoretically protect perfusion, but evidence is weak and inconsistent
- Pragmatic position
- Reasonable in displaced intracapsular Delbet I and II fractures; not proven, so individualise
- The debate
- Recent review suggests plates reduce AVN and physeal closure in displaced and Delbet III/IV patterns, but data are low level
- Pragmatic position
- Choose by pattern and child size; protect the physis where possible
- The debate
- Commonly quoted 15 to 20 mm thresholds are not validated; outcomes are good with both treatments
- Pragmatic position
- Decide on displacement plus symptoms, demand and chronicity, not a single number
At a Glance Table
- Most likely injury family
- Pelvic ring injury
- Immediate question
- Is the child haemodynamically unstable or bleeding?
- Do not miss
- Urogenital, abdominal, head, chest and spine injury
- Most likely injury family
- Posterior hip dislocation
- Immediate question
- Can it be reduced promptly and safely?
- Do not miss
- Sciatic nerve injury, femoral head injury, loose body
- Most likely injury family
- Paediatric femoral neck fracture
- Immediate question
- What is the Delbet type and displacement?
- Do not miss
- AVN, coxa vara, nonunion, pathological fracture
- Most likely injury family
- ASIS or AIIS avulsion
- Immediate question
- How displaced and what sport demand?
- Do not miss
- Misdiagnosis as muscle strain or tumour
- Most likely injury family
- Acetabular or triradiate injury
- Immediate question
- Is the joint congruent and growth plate involved?
- Do not miss
- Growth disturbance, arthritis, intra-articular step
RISKFirst Pass
Hook:In paediatric pelvis and hip trauma, identify the risk created by the injury.
REDUCEHip Dislocation Priorities
Hook:A dislocated paediatric hip is a time-sensitive problem.
AVNFemoral Neck Red Flags
Hook:AVN is the complication that drives urgency.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old is brought after a road trauma with pelvic pain and hypotension. The AP pelvis shows pelvic ring disruption. How do you manage this?”
“A 9-year-old has a posterior hip dislocation after a fall. What is your treatment sequence?”
“A 15-year-old sprinter has sudden pain at the ischial tuberosity with a displaced apophyseal avulsion. How do you decide treatment?”
“An 11-year-old has a displaced transcervical (Delbet II) femoral neck fracture after a fall from height. How do you manage this and what do you tell the family?”
First Priorities
- Primary survey, analgesia and associated injury screening.
- AP pelvis plus targeted hip and femur imaging.
- CT for complex pelvic ring, acetabular and post-reduction hip questions.
- MRI for occult injury, chondral injury, AVN concern and subtle apophyseal injury.
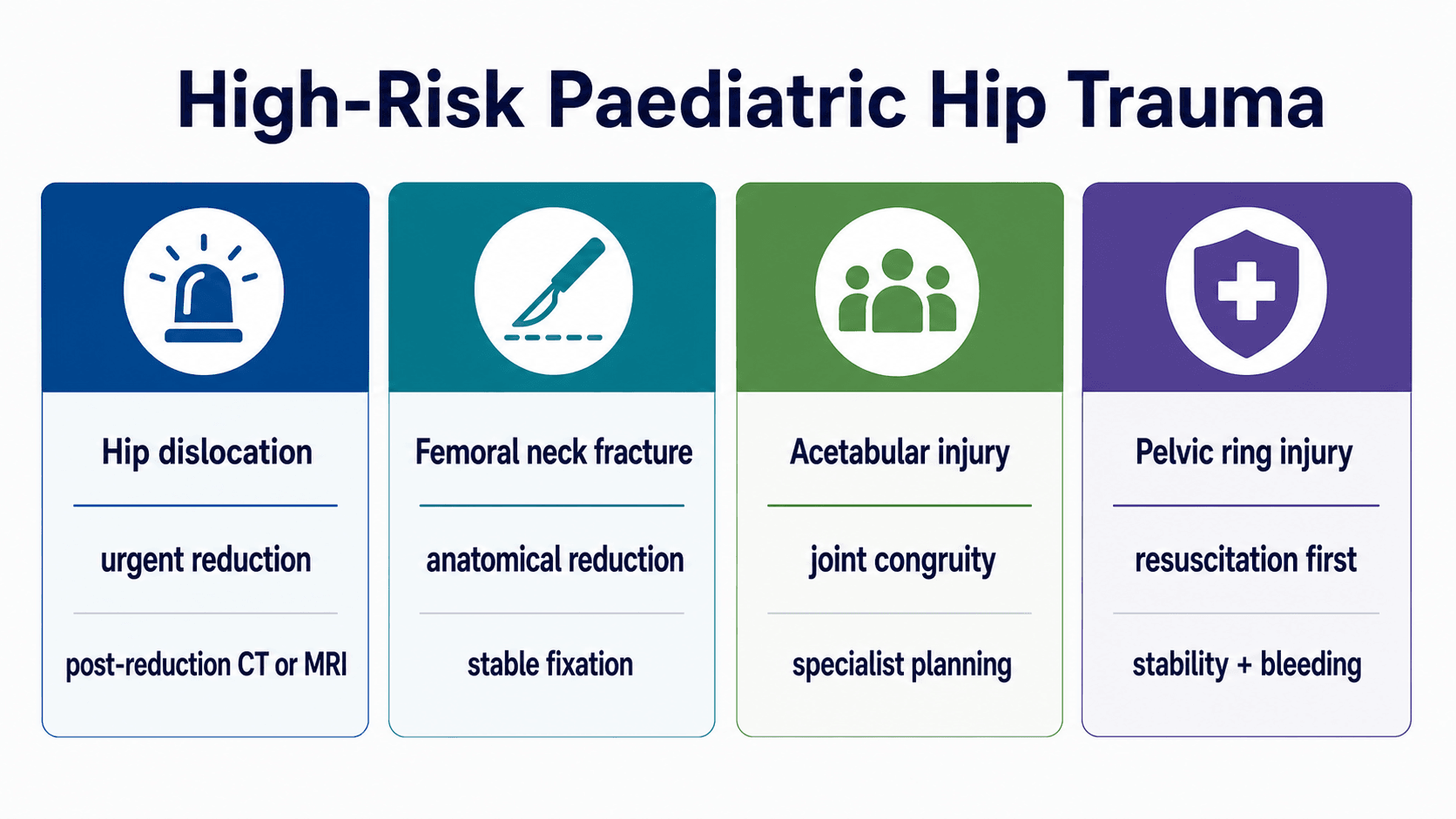
High-Risk Injuries
- Hip dislocation: urgent reduction and post-reduction imaging.
- Femoral neck fracture: Delbet type, displacement, anatomical reduction and stable fixation.
- Acetabular fracture: joint congruity and triradiate cartilage risk.
- Unstable pelvic ring injury: resuscitation, bleeding and associated injuries.
Common Sports Injury
- Apophyseal avulsion commonly affects ASIS, AIIS, ischial tuberosity, iliac crest and lesser trochanter.
- Most are treated non-operatively.
- Surgery is considered for selected displaced, high-demand, neurological or chronic symptomatic cases.
Complications
- AVN after hip dislocation or femoral neck fracture.
- Coxa vara and nonunion after femoral neck fracture.
- Growth disturbance after acetabular or physeal injury.
- Post-traumatic arthritis, stiffness and return-to-sport failure.
“A strong paediatric pelvis and hip trauma approach starts with resuscitation, then separates pelvic ring, acetabular, hip dislocation, femoral neck and apophyseal injuries by the risk each creates.”
Evidence Base
Risk factors for AVN after paediatric femoral neck fracture
- Initial displacement was the strongest predictor of avascular necrosis (RR 2.98, 95% CI 2.04 to 4.35).
- Delbet type I or II fractures (RR 1.96), poor reduction quality (RR 2.43) and age 12 years or older (RR 1.40) all increased AVN risk.
- In long-term follow-up of at least 5 years, delayed reduction raised AVN risk (RR 2.63) and closed reduction outperformed open reduction (RR 0.40).
Plate versus screw fixation for paediatric femoral neck fractures
- Functional outcomes by Ratliff criteria were comparable between plate and screw fixation overall.
- Plate fixation showed lower rates of avascular necrosis and premature physeal closure, with a slightly higher coxa vara rate.
- The advantage of plate fixation was clearest in displaced fractures and Delbet type III or IV patterns.