FOOSH injuries, torus fractures, physeal patterns and safe immobilisation
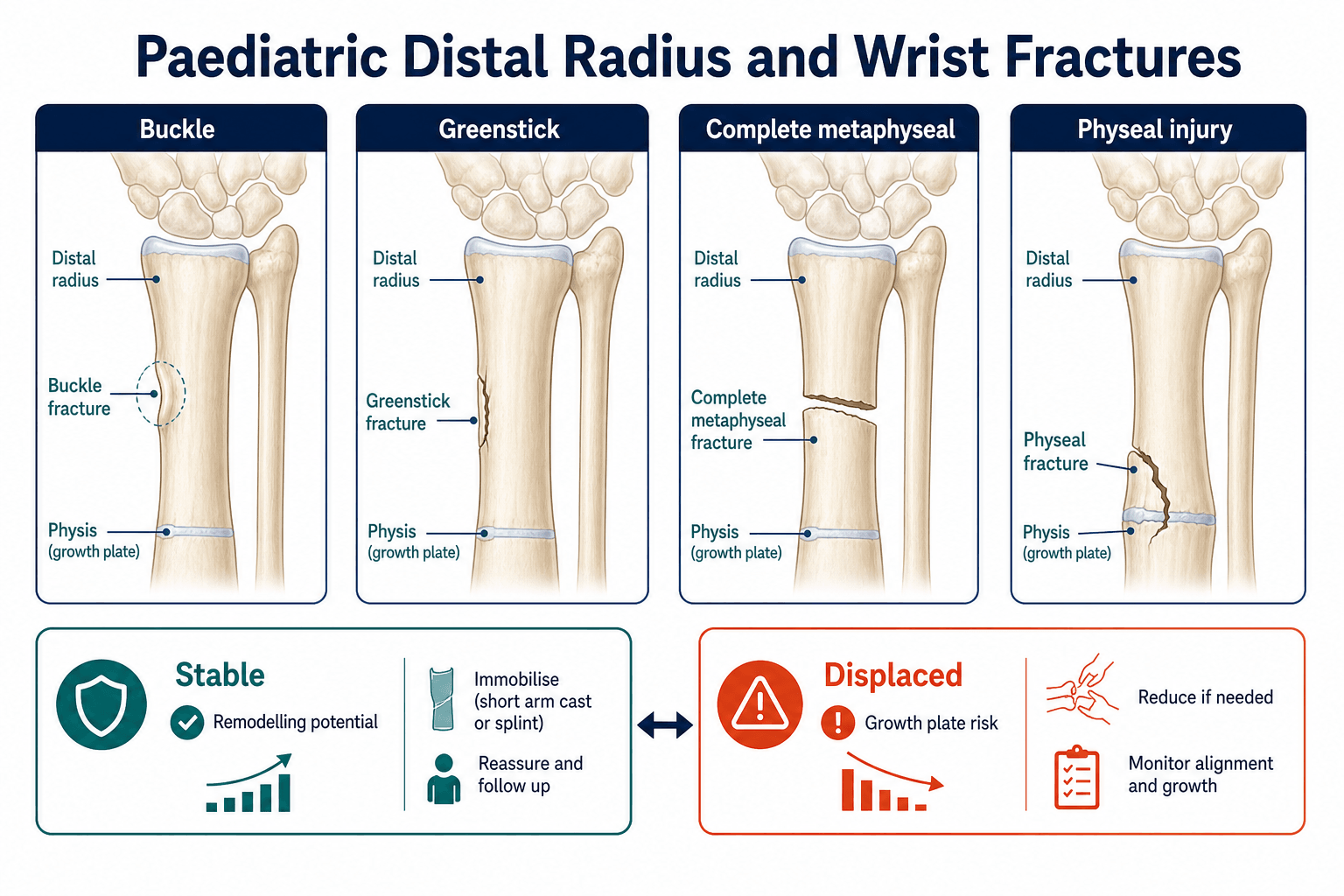
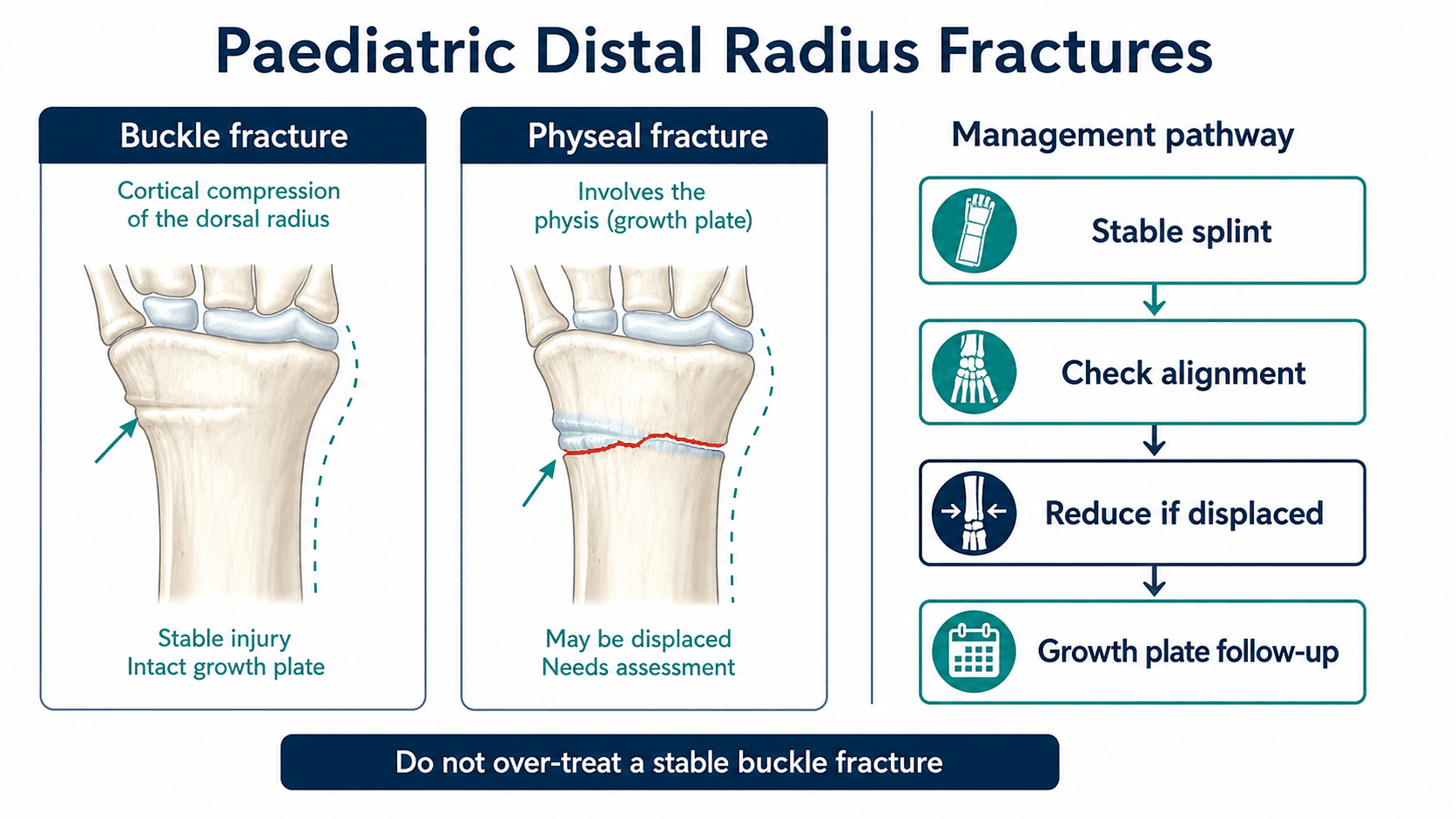
- Buckle fractures are stable compression injuries with no complete cortical break.
- Distal radius remodelling is strong, especially in younger children and sagittal-plane deformity.
- Physeal injuries need careful reduction attempts and follow-up for growth disturbance.
- A displaced complete fracture is not a buckle fracture.
- Cast tightness and median nerve symptoms must be actively checked.
- “Point tenderness over distal radius after FOOSH should be imaged.
- “Buckle fractures can often be treated with removable splint and clear advice.
- “Repeated forceful physeal reductions increase growth-plate risk.
- “Document median nerve before and after reduction.
Do not over-treat a true buckle fracture or under-treat a displaced physeal fracture. The difference is cortical stability, deformity, tenderness pattern and radiographic alignment.
Images and Diagrams
| Question | Answer | Clinical use |
|---|---|---|
| Stable injury? | Buckle fracture with intact opposite cortex | Splint or simple immobilisation with safety advice |
| Unstable injury? | Complete metaphyseal fracture, bayonet apposition or displaced physis | Reduction and closer follow-up may be needed |
| Key assessment? | Skin, deformity, median nerve and perfusion | Detects urgent problems before casting |
| Growth issue? | Distal radial physis contributes major forearm growth | Physeal injuries require surveillance |
WRISTAssessment
Hook:WRIST keeps the examination safe: skin, cortex, sensation, physis and cast symptoms.
BUCKLEStable Torus Injury
Hook:BUCKLE reinforces why true torus fractures need comfort, advice and confidence rather than fracture over-treatment.
PHYSISGrowth Plate Risk
Hook:PHYSIS keeps growth-plate injuries separate from stable buckle fractures.
Overview/Epidemiology
Paediatric distal radius injuries are among the most common fractures in childhood, usually after a fall on an outstretched hand. They range from a stable compression injury to a displaced fracture involving both cortices or the distal radial physis. The clinical skill is matching the amount of treatment to the true stability of the injury.
A buckle fracture is a compression bulge in the cortex. It is stable because there is no complete cortical disruption. It should not be treated like a displaced fracture. Conversely, a complete metaphyseal fracture or displaced physeal injury should not be softened into the word "buckle" just because the child is young.
Remodelling potential is excellent near the distal radial physis, especially in younger children and sagittal-plane deformity. It is less reliable in adolescents, coronal deformity, rotational deformity, unstable complete fractures and injuries close to skeletal maturity. Distal ulna physeal injury deserves special attention because growth disturbance can create ulnar variance and distal radioulnar joint problems.
The goals are simple: identify the pattern, protect the skin and nerves, avoid unnecessary follow-up for stable buckle fractures, reduce unacceptable deformity gently, use a well-moulded non-tight cast when needed, and give families clear cast and swelling return advice.
Pathophysiology
Most paediatric distal radius fractures occur after axial load through an extended wrist. The injury pattern depends on bone elasticity, cortical failure, periosteal hinge integrity and whether the force exits through the metaphysis or the physis.
| Pattern | Structural problem | What it means clinically |
|---|---|---|
| Buckle or torus | Compression crumples one cortex but the bone is not broken through. | Inherently stable when correctly diagnosed; treatment is for comfort and confidence. |
| Greenstick | The tension cortex fails and the compression cortex bends. | The intact cortex can preserve partial stability, but angulation can persist unless moulded or reduced. |
| Complete metaphyseal | Both cortices fail, often with dorsal angulation, translation or shortening. | This is an unstable fracture pattern compared with a buckle injury; reduction and follow-up depend on age and alignment. |
| Physeal | The distal radial or ulnar physis fails because the growth plate is weaker than surrounding ligaments. | Reduction should be gentle, and displaced injuries need surveillance for growth disturbance. |
Remodelling depends on age, plane of deformity and proximity to the distal radial physis. Younger children have more growth remaining. Sagittal-plane deformity remodels more predictably than coronal deformity, and rotation does not remodel reliably. Shortening or bayonet apposition may be acceptable in selected young children, but it should not be used as a blanket rule for adolescents near skeletal maturity.
Median nerve symptoms can occur from swelling, deformity or a tight cast. Distal ulna physeal injury carries growth-disturbance risk and should not be forgotten when the radius fracture dominates the X-ray.
Classification
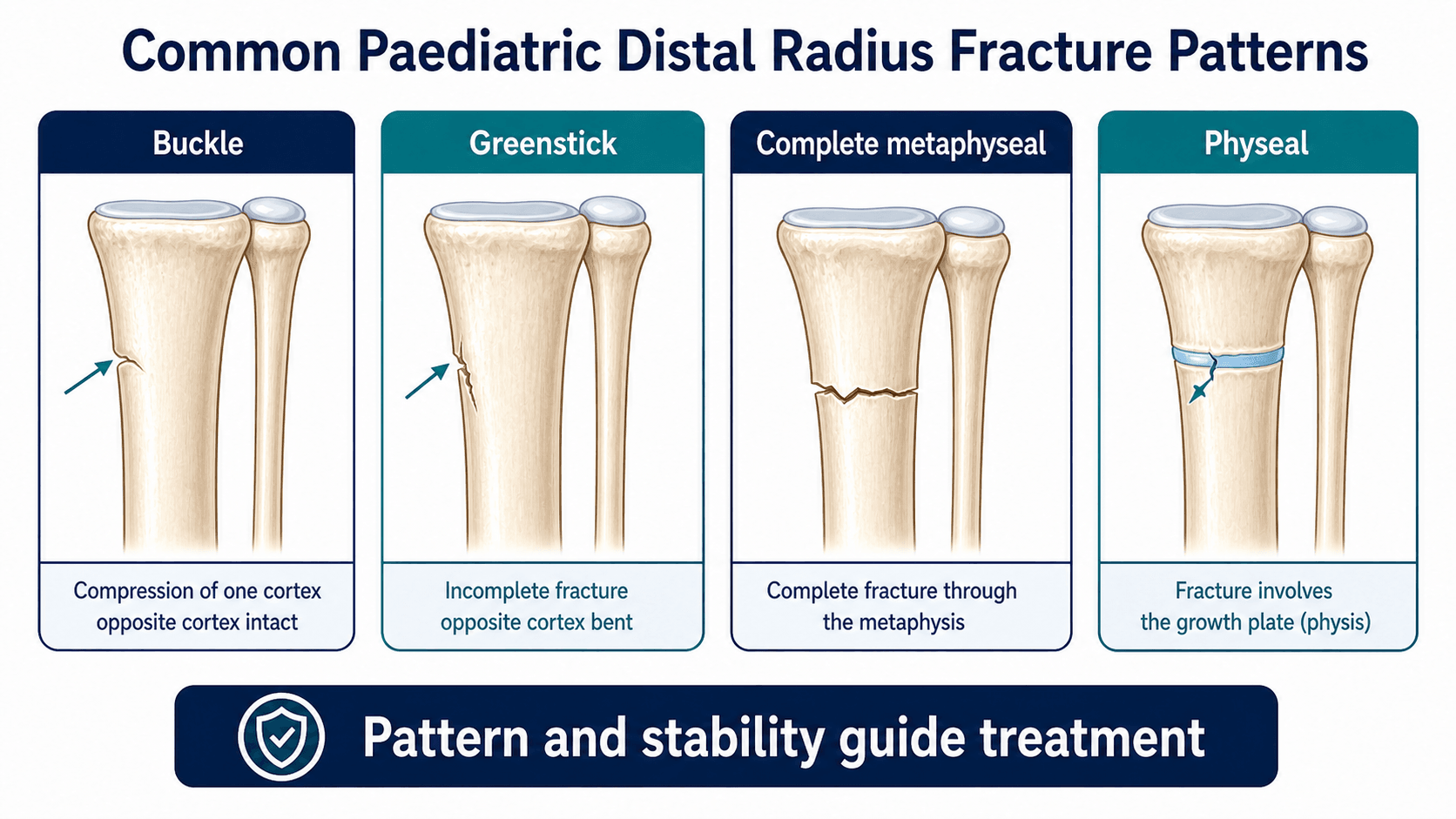
- Buckle: stable cortical bulge without complete break.
- Greenstick: one cortex broken and the other bent.
- Complete metaphyseal: both cortices disrupted, may angulate or shorten.
- Physeal: Salter-Harris pattern involving distal radial or ulnar physis.
Clinical Presentation
History
The history should separate a stable low-energy wrist injury from a displaced fracture, associated injury or safeguarding concern.
| Question | Useful details | Why it matters |
|---|---|---|
| Mechanism | Fall on outstretched hand, sport, scooter, trampoline, fall from height, direct blow or crush. | Higher-energy mechanisms increase the chance of complete fracture, associated elbow injury, open injury or neurovascular concern. |
| Pain location | Distal radius, distal ulna, snuffbox, whole forearm or elbow. | Focal distal radial pain fits buckle or distal radius fracture; snuffbox or elbow pain changes imaging. |
| Function after injury | Refusal to use the hand, visible deformity, finger movement and ability to tolerate a splint. | Deformity and severe pain make a simple buckle fracture less likely. |
| Neurological symptoms | Numbness or paraesthesia in thumb, index or middle fingers. | Suggests median nerve irritation from swelling, deformity or tight immobilisation. |
| Current cast or splint symptoms | Increasing pain, swollen fingers, colour change, numbness or inability to move fingers. | This is a cast safety problem until proven otherwise. |
| Bone health and safeguarding | Recurrent fractures, very low-energy injury, inconsistent history, delay in presentation or non-mobile child. | May require metabolic bone or child protection assessment. |
Examination
Inspection separates a comfortable stable injury from a deformed unstable fracture. Do not force wrist movement when the diagnosis is clinically obvious.
| Area | What to check | Decision it informs |
|---|---|---|
| Skin and swelling | Bruising, open wound, threatened skin, cast pressure, finger swelling and colour. | Open or threatened-skin injuries need urgent escalation; tight casts must be split or removed. |
| Deformity | Dorsal or volar angulation, translation, shortening and forearm shape. | Visible deformity usually means complete or physeal fracture, not a simple buckle injury. |
| Bony tenderness | Distal radius, distal ulna physis, DRUJ, snuffbox, forearm shaft and elbow. | Guides radiograph field and prevents missed ulna, scaphoid, Galeazzi-equivalent or elbow injury. |
| Median nerve | Thumb, index and middle-finger sensation; thumb opposition or flexion when age-appropriate. | Document before and after reduction because swelling or deformity can compromise the nerve. |
| Perfusion | Radial pulse, capillary refill, warmth and finger movement. | Confirms vascular safety and helps detect evolving compartment or cast problems. |
| Compartment signs | Pain out of proportion, pain with passive finger stretch, increasing analgesia need and tense swelling. | Requires urgent review; do not dismiss it as expected fracture pain. |
The clinical and radiographic question is stability: a buckle fracture is a compression bulge, not a complete fracture wearing a nicer name.
Investigations
| Clinical question | Investigation | Decision it informs |
|---|---|---|
| Initial assessment | AP and lateral wrist radiographs including distal radius and ulna | Classifies buckle, metaphyseal or physeal injury |
| Possible elbow or forearm injury | Forearm or elbow radiographs as indicated | Detects associated injury |
| Post-reduction | Repeat AP and lateral films | Confirms alignment and cast quality |
| Persistent snuffbox pain | Scaphoid views or MRI in selected adolescents | Avoids missed carpal injury |
- Look at both cortices before calling a buckle fracture.
- Assess dorsal or volar tilt, translation, shortening and associated ulna fracture.
- Do not miss distal ulna physeal injury.
- In adolescents, consider carpal injury if pain is not explained by distal radius findings.
- Repeat imaging depends on stability, age, reduction and local fracture protocol.
Differential Diagnosis
| Diagnosis | Clue | Clinical consequence |
|---|---|---|
| Wrist sprain | Diffuse pain without focal bony tenderness or radiographic abnormality. | Use cautiously; focal distal radial tenderness in a child is a fracture until assessed properly. |
| Scaphoid fracture | Snuffbox tenderness, pain with axial thumb loading, adolescent age group. | May need scaphoid views, immobilisation and interval imaging or MRI. |
| Distal ulna physeal injury | Ulnar-sided physeal tenderness or associated distal ulna fracture. | Carries growth-arrest and ulnar-variance risk; do not focus only on the radius. |
| Galeazzi equivalent | Distal radial fracture with DRUJ pain, distal ulna physeal injury or ulnar head prominence. | Requires DRUJ and ulna assessment, not just routine distal radius management. |
| Non-accidental injury | Inconsistent history, delay, non-mobile child or additional injuries. | Escalate safeguarding assessment. |
| Pathological fracture | Very low-energy mechanism, recurrent fractures or abnormal bone lesion. | Consider metabolic bone disease or benign bone lesion work-up. |
Management
The first management decision is whether the injury is truly stable. A true buckle fracture can be managed simply because it is a stable compression injury. A displaced complete or physeal fracture needs alignment assessment, reduction decision, cast quality and follow-up.
| Pattern | Usual treatment direction | Follow-up focus |
|---|---|---|
| True buckle fracture | Removable splint, soft bandage or simple immobilisation according to local protocol; analgesia and written advice. | Return if pain worsens, fingers swell or function does not recover as expected; routine repeat X-rays are often unnecessary when diagnosis is secure. |
| Minimally angulated greenstick or metaphyseal fracture | Short-arm cast or splint/cast strategy depending stability, age, pain and local protocol. | Confirm that alignment remains acceptable if there is displacement risk. |
| Displaced complete metaphyseal fracture | Analgesia or sedation, closed reduction when alignment is unacceptable, well-moulded cast and post-reduction films. | Early review for redisplacement, especially with poor cast moulding, both-bone injury or older child. |
| Displaced distal radial physeal fracture | Gentle reduction if unacceptable; avoid repeated forceful attempts; immobilise and document neurovascular status. | Monitor reduction and later growth, particularly after high-energy injury or repeated manipulation. |
| Distal ulna physis or DRUJ concern | Assess DRUJ stability and ulnar physis; treat associated instability rather than ignoring it. | Watch for ulnar variance, wrist pain and forearm rotation problems. |
| Open, neurovascular or compartment concern | Urgent orthopaedic management, cast release when tight, antibiotics and theatre when open. | Safety takes priority over routine fracture pathway. |
- Explain that this is a stable compression injury.
- Use removable wrist splint or simple immobilisation according to local protocol.
- Encourage finger, elbow and shoulder movement.
- Avoid contact sport until pain-free and advised timeframe completed.
- Give return advice rather than routine intensive fracture surveillance when truly stable.
Complications
Early
- Median nerve symptoms.
- Cast tightness, swelling or pressure injury.
- Loss of reduction.
- Compartment syndrome, rare but serious.
- Missed associated elbow or carpal injury.
Late
- Malunion with residual deformity.
- Distal radial or ulnar physeal arrest.
- Wrist stiffness from over-immobilisation.
- Refracture after early return to sport.
- Cosmetic deformity or functional limitation if alignment unacceptable.
The common error is mismatch: too much treatment for a buckle fracture or too little respect for an unstable physeal or complete fracture.
Decision-Making in Practice
Paediatric distal radius injuries should be separated into stable buckle fractures, greenstick or complete metaphyseal fractures, and physeal injuries. These are different problems. A buckle fracture is a stability and comfort problem; a displaced physeal injury is a reduction, growth and follow-up problem.
| Injury | Key assessment | Treatment direction |
|---|---|---|
| Buckle or torus fracture | Cortical buckling without cortical breach, no physeal extension, stable alignment | Removable splint or soft bandage with simple safety-netting is often enough |
| Greenstick/metaphyseal fracture | Angulation, translation, age and remodeling potential | Cast, moulded reduction or fixation depending stability |
| Distal radial physeal fracture | Salter-Harris pattern, displacement, reduction quality and growth remaining | Gentle reduction, immobilisation and growth follow-up when displaced |
| Distal ulnar physeal injury | Associated ulnar physeal damage or DRUJ symptoms | Higher vigilance for growth arrest and ulnar variance problems |
| Safeguarding concern | Non-mobile child, inconsistent history or additional injuries | Escalate child protection assessment before routine discharge |
The practical error is over-treating stable buckle fractures while under-recognising physeal injuries. True torus fractures should not need repeated X-rays, prolonged casting or fracture-clinic congestion when diagnosis is secure and the family has clear return advice. Conversely, a displaced physeal injury needs reduction quality, neurovascular status, cast mould, re-displacement risk and later growth assessment considered.
Return to sport depends on pain-free wrist motion, tenderness resolution and injury pattern. A buckle fracture returns earlier than a displaced physeal fracture or complete metaphyseal fracture.
Controversies and Areas of Uncertainty
Several questions in paediatric distal radius care remain genuinely unresolved, and examiners reward candidates who can state both sides rather than quote a single number.
| Controversy | One side | Other side |
|---|---|---|
| Bayonet apposition in young children | Off-ended (bayonet) complete fractures with good alignment can remodel without formal reduction in younger children. | Some surgeons still reduce to restore length, citing variable remodelling and parental expectation. |
| Acceptable angulation limits | Traditional teaching cites roughly 15 to 20 degrees sagittal in younger children, more with more growth remaining. | Remodelling studies show even higher angulation can correct, so thresholds are guides, not hard rules. |
| Reduction versus immobilisation in situ for greenstick | Completing or moulding the fracture may reduce redisplacement. | Gentle moulding without completing the fracture avoids extra injury and is often sufficient. |
| Pinning displaced metaphyseal fractures | Percutaneous wiring reduces redisplacement and remanipulation. | Long-term functional benefit is unproven and pinning adds anaesthetic, scar and hardware risks. |
| Routine repeat radiographs for buckle fractures | Some protocols still image at review. | High-level evidence supports discharge without routine repeat imaging when the diagnosis is secure. |
| Need for any radiograph in minor wrist injury | Imaging confirms the pattern and excludes physeal or complete fracture. | A validated clinical decision rule to avoid radiography in minor injuries is an explicit research priority from the FORCE programme. |
Guidelines, Registries & Global Practice
Paediatric distal radius fractures are a worldwide problem and the single most common skeletal injury requiring intervention in children. Practice varies more by health-system resource and local protocol than by true biological difference, so the global picture matters for any exam answer.
Global epidemiology
- Distal forearm fractures account for roughly a quarter to a third of all childhood fractures, with peak incidence around the pubertal growth spurt.
- Boys are affected more often than girls overall, mirroring activity exposure; in the FORCE cohort 61 percent were boys.
- Rising incidence has been linked to increased sport participation, higher body mass index and reduced bone mineral density in some populations.
- Distal ulnar physeal injuries show growth disturbance in around one in five cases, and intra-articular (Salter-Harris III/IV) distal radius fractures in around two in five.
Side-by-side guidance
| Body / source | Torus (buckle) fractures | Displaced and physeal fractures |
|---|---|---|
| BOA / BOAST (UK) | Supports minimal immobilisation and discharge with safety-netting; reflects FORCE findings. | Timely reduction of unacceptable alignment, neurovascular documentation and structured follow-up. |
| AAOS / POSNA (US) | Removable splint or simplified care for stable torus fractures. | Closed reduction for unacceptable alignment; pinning for unstable or recurrently displaced fractures; physis guides decisions. |
| AO Foundation | Recognises torus as stable; protective immobilisation for comfort. | Reduction and well-moulded casting; emphasises cast index and Kirschner-wire fixation when unstable. |
| EFORT / European consensus | Aligns with minimal-immobilisation evidence for true torus injuries. | Accept remodelling in younger children; reserve fixation for instability or maturity. |
Registry and trial evidence
- Paediatric fracture care is driven by trial evidence rather than implant registries (registries dominate adult arthroplasty, not childhood fractures).
- The FORCE equivalence RCT (965 children, 23 UK hospitals) is the landmark dataset supporting bandage-and-discharge for torus fractures.
- Cohort data from North American children's hospitals define the growth-arrest risk that justifies physeal surveillance.
High- versus limited-resource practice
- In well-resourced systems the debate is about doing less: removable splints, no routine repeat films and reduced clinic visits for buckle fractures.
- In limited-resource settings the priorities are accurate triage to avoid missing displaced or physeal fractures, safe casting where image-guided fixation is unavailable, and clear caregiver safety-netting because follow-up may be difficult.
- Across all settings the universal non-negotiables are neurovascular assessment, recognition of the physis and a well-moulded, non-tight cast when immobilisation is used.
Evidence Signals
FORCE trial: bandage equivalent to rigid immobilisation for torus fractures
- Multicentre equivalence RCT of 965 children aged 4 to 15 across 23 UK hospitals.
- Pain at 3 days was equivalent: 3.21 vs 3.14 points, adjusted difference -0.10 (95% CI -0.37 to 0.17), within the prespecified margin of 1.0.
- No between-group difference in pain or function across 6 weeks of follow-up.
FORCE HTA: bandage is also cost-effective and complication-equivalent
- Complications were rare and equivalent: 5 (1.0%) with bandage versus 3 (0.6%) with rigid immobilisation.
- No difference in functional recovery, quality of life or school absence over 6 weeks.
- The offer of a bandage reduced treatment cost and was highly likely to be cost-effective.
Plint RCT: removable splint improves function over casting for buckle fractures
- RCT of 113 children aged 6 to 15 with distal radius and/or ulna buckle fractures (87 analysed).
- Removable splint gave better physical functioning (ASKp score) at day 14 and less difficulty with bathing, with no difference in pain.
- There were no refractures in either group.
Cochrane review: evidence supports removable splintage for buckle fractures
- Ten trials involving 827 children; four compared removable splintage versus below-elbow cast for buckle fractures.
- No short-term deformity in any buckle-fracture trial and no refracture at 6 months in the reporting trial.
- Below-elbow casts did not increase redisplacement versus above-elbow casts; percutaneous wiring reduced redisplacement of displaced fractures.
Current concepts: physis guides treatment of all distal radius fractures
- Distal radius fractures are the most common skeletal injury requiring intervention in children.
- Proximity to the physis and remaining skeletal growth guide treatment for all patterns, not just physeal fractures.
- Even among experts there is little consensus on optimal treatment of displaced metaphyseal fractures.
Distal ulna physeal fractures: ~20% growth disturbance
- Fifty-six children with distal ulnar physeal fracture; growth disturbance in 11 (19.6%), with complete arrest in 8 (14.3%).
- Displaced and Salter-Harris III/IV fractures had higher arrest rates (34.8% vs 3.2%; 50% vs 11.1%).
- Less than 2 years of growth remaining markedly raised arrest risk (46.2% vs 9.5%).
Intra-articular distal radius fractures carry high growth-arrest risk
- Twenty-eight skeletally immature patients with Salter-Harris III/IV distal radius fractures.
- Growth disturbance occurred in 12 (43%), substantially higher than rates after extra-articular physeal fractures.
- All four children aged 10 or younger developed arrest requiring skeletal rebalancing procedures.
Clinical Reasoning Notes
| Step | Question | Safe answer |
|---|---|---|
| 1 | Is it truly a buckle fracture? | Check both cortices and the physis. A complete fracture or displaced physis should not be discharged as a buckle injury. |
| 2 | Is the child neurovascularly safe? | Document median nerve and perfusion before and after reduction or cast application. |
| 3 | Is the alignment acceptable for this child? | Younger children remodel more; adolescents and rotational deformity are less forgiving. |
| 4 | Can the fracture redisplace? | Complete fractures, associated ulna fractures and poor cast moulding need closer follow-up than stable buckle fractures. |
| 5 | Is there a growth-plate issue? | Name distal radial and distal ulnar physeal injuries explicitly and arrange surveillance when risk is meaningful. |
| 6 | Does the family know when to return? | Increasing pain, swollen fingers, numbness, colour change or inability to move fingers is urgent. |
Common pitfalls
| Pitfall | Why it is unsafe | Better practice |
|---|---|---|
| Calling a complete fracture a buckle fracture | The child may be discharged without reduction or redisplacement follow-up. | Confirm no complete cortical breach and no physeal extension. |
| Ignoring the distal ulna physis | Growth arrest can later cause ulnar variance and DRUJ symptoms. | Examine and report distal ulna tenderness and radiographic injury. |
| No neurovascular check after reduction | Median nerve deterioration may be missed. | Document sensation, motor function and perfusion before and after manipulation. |
| Overly tight circumferential cast during swelling | Can worsen pain, nerve symptoms or compartment risk. | Use appropriate padding, moulding and cast splitting when swelling risk is high. |
| Repeated forceful physeal reduction | May increase iatrogenic growth-plate injury. | Use adequate analgesia/sedation, gentle technique and senior help if reduction fails. |
| No safety advice | Families may wait despite cast pain, numbness or swollen fingers. | Give clear written and verbal return precautions. |
Evidence Base
Remodelling continues even above the 15 degree threshold
- Forty distal radius malunions in 33 children (aged 3 to 14) healed at 15 degrees angulation or more.
- All fractures remodelled; mean dorsovolar malunion fell from 23 to 8 degrees and radioulnar from 21 to 10 degrees.
- Remodelling speed (mean 2.5 degrees per month) decreased exponentially over time and rose with greater initial angulation.
Distal radius-ulna fractures: review of principles and complications
- Management must include neurovascular assessment, soft-tissue evaluation and explicit attention to the radial and ulnar physes.
- Treatment ranges from casting with radiographic follow-up to urgent reduction and surgical fixation.
- Both early (median nerve, compartment) and late (growth arrest) complications can affect outcomes.
Late manipulation of physeal fractures risks iatrogenic arrest
- Nonsurgical management is most common because of marked remodelling potential.
- Physeal fractures presenting more than 10 days after injury should not be manipulated because of increased physeal-arrest risk.
- Substantial angulation or displacement warrants closed reduction with or without percutaneous pinning.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A seven-year-old has a distal radius buckle fracture after FOOSH. How do you manage it?”
“A child has a displaced distal radial Salter-Harris II fracture. What are your priorities?”
“A 13-year-old has a completely displaced, dorsally angulated complete metaphyseal distal radius fracture with bayonet apposition. The wrist is swollen and the child reports tingling in the thumb. How do you proceed?”
Buckle
- Compression bulge
- Stable
- No complete cortex break
- Splint
- Return advice
Displaced
- Deformity
- Both cortices or physis
- Reduction if unacceptable
- Moulded cast
- Repeat X-ray
Check
- Skin
- Median nerve
- Perfusion
- Finger movement
- Cast tightness
Do Not Miss
- Distal ulna physis
- Scaphoid in adolescent
- Galeazzi equivalent
- Compartment signs