Ossification centres, anterior humeral line, radiocapitellar line and occult fracture signs
- Know the CRITOE ossification sequence and expected age range.
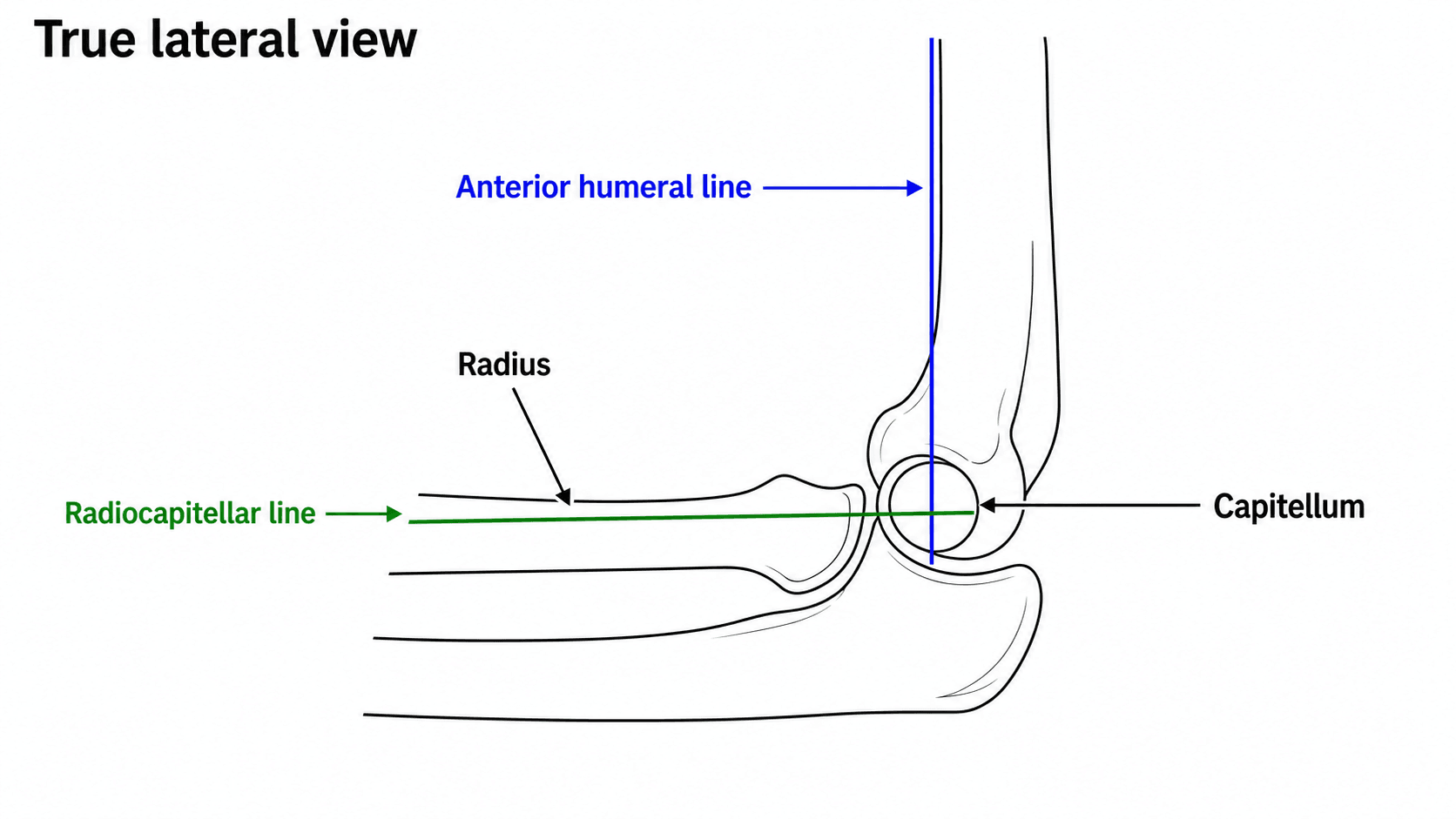
- The anterior humeral line should pass through the middle third of the capitellum in most children older than about four years.
- The radiocapitellar line should pass through the capitellum on every view.
- A posterior fat pad after trauma suggests intra-articular fracture until proven otherwise.
- Compare clinical swelling, tenderness and neurovascular status with the radiograph.
- “Ask whether the X-ray is a true lateral before trusting the lines.
- “Radiocapitellar alignment must be checked on AP and lateral views.
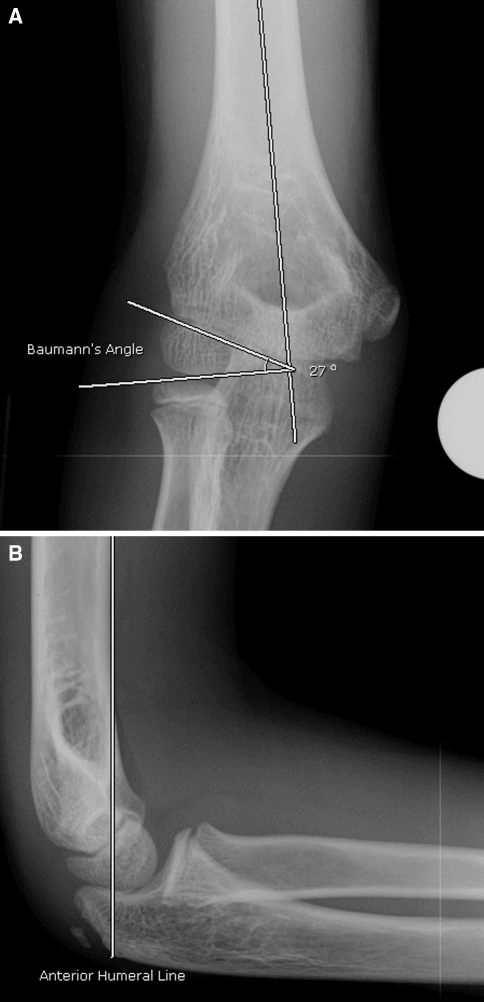
- “Baumann angle helps assess coronal alignment in supracondylar fractures.
- “The youngest children have the most cartilage and the least forgiving radiographs.
A normal-looking paediatric elbow X-ray can hide a fracture. Read the film with CRITOE, fat pads, anterior humeral line, radiocapitellar line and alignment before reassuring the family.
Images and Diagrams
| Question | Answer | Clinical use |
|---|---|---|
| First check? | Is this a true AP and true lateral? | Poor positioning makes every line unreliable |
| Key sequence? | Capitellum, radial head, internal epicondyle, trochlea, olecranon, external epicondyle | Avoid mistaking normal ossification for fracture |
| Danger sign? | Posterior fat pad after trauma | Treat as occult fracture when clinical story fits |
| Alignment lines? | AHL through capitellum and RCL through capitellum | Screens supracondylar and radiocapitellar injury |
CRITOEOssification Order
Hook:CRITOE keeps ossification centres in the expected order before calling a fracture fragment abnormal.
LINESAlignment Lines
Hook:LINES links each radiographic line to the structure it is meant to assess.
FATEffusion Signs
Hook:FAT keeps occult elbow injury on the table when the fracture line is not obvious.
Overview/Epidemiology
Paediatric elbow radiology is difficult because the anatomy visible on X-ray is only the ossified part of a much larger cartilaginous elbow. A fracture may pass through cartilage, an ossification centre may look like a fragment, and malalignment may be subtle unless the view is adequate and the landmarks are used correctly.
The safest approach is not to stare at the film hoping the fracture declares itself. Read every paediatric elbow in the same order: confirm the views, apply CRITOE, draw the anterior humeral line and radiocapitellar line correctly, inspect fat pads, search common fracture sites, and then match the radiograph to swelling, tenderness, nerve function and perfusion.
Common injuries include supracondylar humerus fracture, lateral condyle fracture, medial epicondyle avulsion or incarceration, radial neck fracture, olecranon injury and Monteggia lesion. Soft-tissue signs may be the only clue early. A posterior fat pad after trauma is not a normal finding to ignore; it should trigger concern for occult intra-articular injury when the clinical story fits.
The purpose of this topic is to make the learner safe: know what normal ossification can look like, know where to draw the lines, and know when a subtle film still needs immobilisation, repeat imaging or senior review.
Pathophysiology
The distal humerus and proximal radius are partly cartilaginous in children. A safe interpretation depends on knowing which landmark is reliable for the child's age.
| Concept | Correct interpretation | Common error |
|---|---|---|
| Cartilage and ossification | The X-ray shows only ossified structures; the capitellum appears first and becomes the key lateral landmark. | Reading a child's elbow like an adult elbow. |
| Anterior humeral line | On a true lateral, draw along the anterior humeral cortex; it should intersect the capitellum in most children beyond early ossification. | Drawing a mid-shaft line or trusting an oblique lateral. |
| Radiocapitellar line | Draw along the central axis of the radial shaft and neck; it should pass through the capitellum on AP and lateral views. | Ignoring a missed capitellum when the forearm may hide a Monteggia lesion. |
| Fat pads | Posterior fat pad after trauma is abnormal; raised anterior fat pad supports effusion. | Reassuring the family despite swelling, pain and effusion. |
Classification
- Confirm patient age and side.
- Assess true AP and lateral adequacy.
- Identify CRITOE centres expected for age.
- Check anterior humeral line.
- Check radiocapitellar line on AP and lateral.
- Assess fat pads and soft-tissue swelling.
- Review cortex around supracondylar region, lateral condyle, medial epicondyle, radial neck and olecranon.
Clinical Presentation
History
The history guides which part of the elbow radiograph deserves extra attention.
- Fall on outstretched hand or hyperextension injury: supracondylar fracture and radial neck injury are common considerations.
- Direct lateral elbow pain: consider lateral condyle fracture, which can be subtle and clinically important.
- Medial pain after dislocation: look for medial epicondyle avulsion or an incarcerated fragment.
- Forearm pain or deformity: do not stop at the elbow; image the forearm for a Monteggia pattern.
- Pain escalation, paraesthesia, cool hand or colour change: treat as neurovascular warning symptoms.
- Time since injury and analgesia already given: swelling and compartment concern may evolve.
Examination
Inspect the elbow from the front and side. Marked swelling, deformity, skin puckering or bruising supports a significant injury even if the fracture line is subtle. Palpate systematically: supracondylar region, lateral condyle, medial epicondyle, radial head, olecranon, forearm and wrist.
Neurovascular documentation is part of elbow radiology assessment because the X-ray and the hand must be read together.
| Structure | Child-friendly test | Why it matters |
|---|---|---|
| Perfusion | Radial pulse, capillary refill, hand colour and temperature. | Detects pulseless pink or pulseless pale hand after supracondylar injury. |
| Anterior interosseous nerve | Thumb IP flexion and index DIP flexion. | AIN palsy is common in extension supracondylar fracture. |
| Radial nerve | Wrist or finger extension. | Assesses posterior interosseous/radial nerve function. |
| Ulnar nerve | Finger abduction or crossing. | Important in flexion-type supracondylar injuries and medial epicondyle patterns. |
| Sensation | Light touch where the child can cooperate. | Documents baseline and supports safe follow-up. |
Avoid forceful range of motion in an obviously fractured elbow. Compare the site of maximal tenderness with the radiograph. A child with lateral condyle tenderness and a barely visible lateral metaphyseal line should not be labelled as a simple sprain without follow-up.
The anterior humeral line is drawn along the anterior humeral cortex on a true lateral and should meet the capitellum; the radiocapitellar line follows the radial neck and should cross the capitellum on every adequate view.
Investigations
| Clinical question | Investigation | Decision it informs |
|---|---|---|
| Initial trauma assessment | AP and true lateral elbow radiographs | Allows CRITOE, AHL, RCL and fat-pad assessment |
| Subtle lateral condyle concern | Internal oblique view or repeat radiographs | Detects minimally displaced lateral condyle fracture |
| Monteggia concern | Forearm radiographs including elbow and wrist | Checks ulna alignment and radiocapitellar relation |
| Unclear cartilage injury | Ultrasound, MRI or CT in selected cases | Defines occult or intra-articular injury when management changes |
View quality
Start by asking whether the views are adequate. The lateral should be a true lateral with the distal humeral condyles superimposed. An oblique film can make the anterior humeral line and fat pads misleading. If the AP is rotated, Baumann angle and coronal alignment are less reliable.
Anterior humeral line
Draw the line along the anterior cortex of the distal humerus on the true lateral. In most children beyond early childhood, it should intersect the capitellum. If it passes anterior to the capitellum, suspect an extension supracondylar fracture. Do not draw it down the middle of the humeral shaft or through a random vertical line; it is an anterior cortex line.
Radiocapitellar line
Draw the line through the centre of the radial shaft and neck. It should pass through the capitellum on AP and lateral views. If it misses the capitellum on an adequate film, look for Monteggia injury, radial head dislocation, elbow dislocation or radial neck injury. If the film is poor, repeat or obtain adequate imaging before dismissing the finding.
Fat pads and occult injury
A posterior fat pad after trauma is abnormal. A raised anterior fat pad supports effusion. In a swollen painful elbow, effusion without a visible fracture line should still be treated seriously: immobilise, safety-net and arrange follow-up or repeat imaging.
Ossification Centres
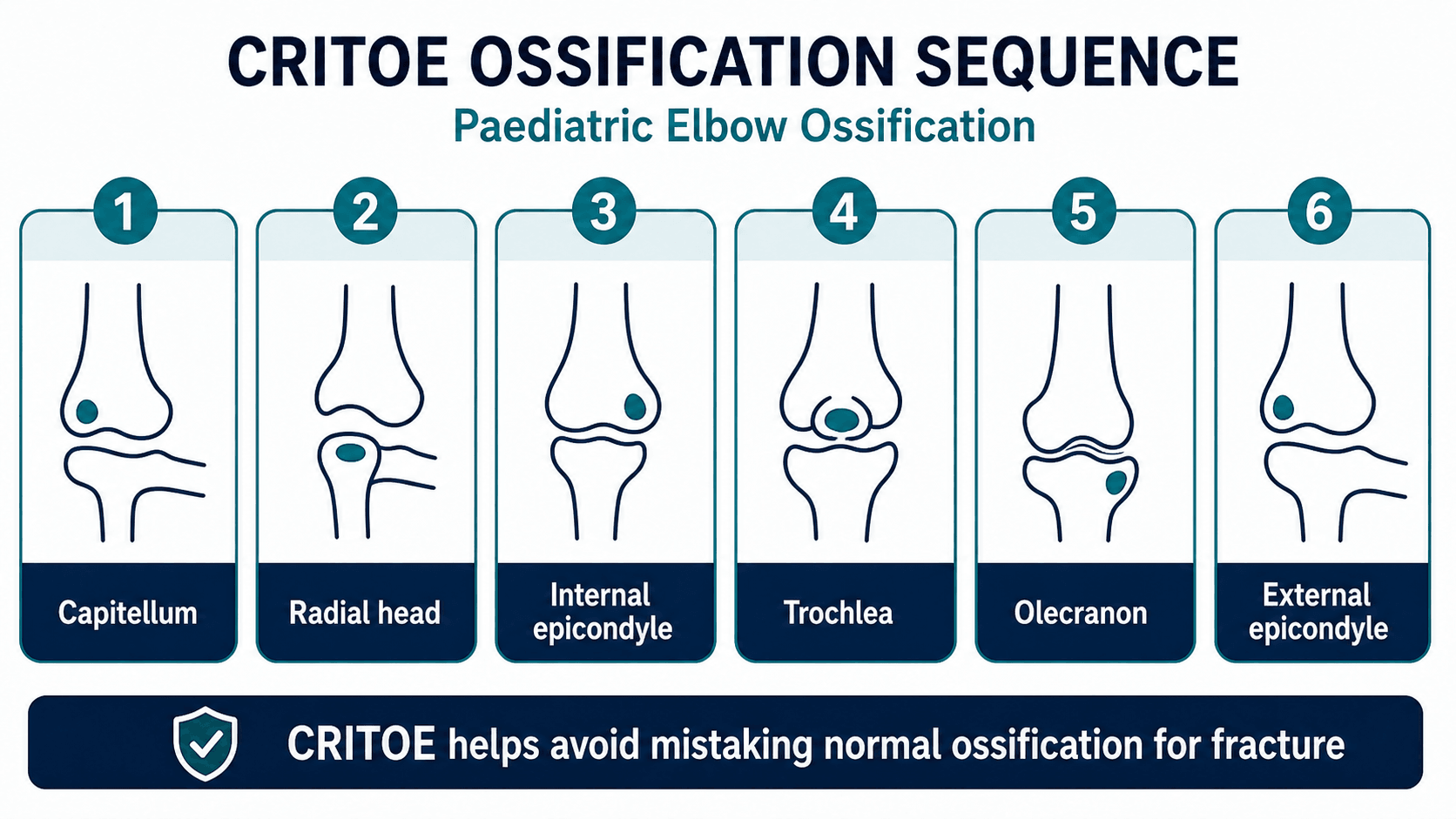
CRITOE describes the usual order in which ossification centres appear around the paediatric elbow: capitellum, radial head, internal epicondyle, trochlea, olecranon and external epicondyle. Exact ages vary, but the order is clinically useful.
| Situation | Safe interpretation | Risk if missed |
|---|---|---|
| Separate medial epicondyle | May be a normal ossification centre depending on age and position. | Calling normal anatomy a fracture. |
| Missing or displaced medial epicondyle after dislocation | Look for avulsion or incarceration in the joint. | Missing a fragment that may require surgery. |
| Fragmented trochlea | Can be normal during ossification. | Overcalling fracture without clinical correlation. |
| Very young child | Much of the distal humerus is cartilage and displacement may be underestimated. | False reassurance from an apparently subtle film. |
| Uncertain centre versus fragment | Compare the other side only if it changes management and does not delay urgent care. | Delaying treatment for a clinically important injury. |
Differential Diagnosis
The differential is really a list of injuries that look subtle on a paediatric elbow film. The job of the reader is to separate normal developmental anatomy from a treatment-changing fracture.
| Differential | Discriminating feature | Pitfall / consequence |
|---|---|---|
| Normal ossification centre | Smooth, corticated, in expected CRITOE position for age; symmetrical clinical exam | Overcalling a fracture; unnecessary immobilisation or surgery |
| Occult supracondylar fracture | Posterior fat pad with normal or near-normal AHL; focal supracondylar tenderness | Reassuring on the fat pad sign alone; 43 percent of fat-pad occult fractures are supracondylar |
| Lateral condyle fracture | Lateral metaphyseal fragment; widened on internal oblique view; lateral ecchymosis | AP view underestimates displacement; late slip under cast leads to non-union |
| Medial epicondyle avulsion / incarceration | Absent medial epicondyle in expected position; fragment within the joint after dislocation | Forgetting CRITOE order and missing an incarcerated fragment requiring surgery |
| Radial neck fracture | Subtle radial head/neck angulation; effusion; radiocapitellar line still intact | Calling it normal when angulation is mild |
| Monteggia lesion | Radiocapitellar line misses the capitellum plus ulna plastic deformation or fracture | Stopping at the elbow and not imaging the whole forearm |
| Pulled elbow (radial head subluxation) | Toddler, axial-traction mechanism, arm held pronated, often normal radiograph | Over-imaging, or conversely missing a true fracture by assuming pulled elbow |
Management
- Confirm adequate views.
- Apply CRITOE.
- Check AHL and RCL.
- Inspect fat pads.
- Search common fracture sites.
- Correlate with focal tenderness and neurovascular status.
Complications
Early
- Missed supracondylar fracture.
- Missed pulseless pink or pulseless pale hand.
- Missed lateral condyle displacement.
- Incarcerated medial epicondyle after dislocation.
- Compartment syndrome from swelling or tight cast.
Late
- Cubitus varus after malunited supracondylar fracture.
- Lateral condyle non-union and fishtail deformity.
- Elbow stiffness.
- Chronic radial head dislocation after missed Monteggia lesion.
- Growth disturbance or angular deformity.
A paediatric elbow X-ray is never just a picture. It is a structured search for alignment, ossification, effusion and the injuries that change treatment.
Decision-Making in Practice
Paediatric elbow radiology is a structured search, not a glance for an obvious fracture. The safest reader checks image quality, ossification sequence, alignment lines, fat pads, common fracture sites and the forearm relationship before deciding the film is normal.
| Step | What to check | Why it matters |
|---|---|---|
| Views | True AP and true lateral, with forearm films when Monteggia is possible | Poor views create false reassurance |
| Ossification | CRITOE order and expected age variation | Normal ossification centres can mimic fracture |
| Alignment | Anterior humeral line and radiocapitellar line drawn through correct landmarks | Detects supracondylar injury and radial head dislocation |
| Effusion | Posterior fat pad or elevated anterior fat pad | Treat occult fracture seriously when clinical signs match |
| Specific sites | Lateral condyle, medial epicondyle, radial neck, olecranon and Monteggia pattern | These are commonly missed and treatment-changing |
The anterior humeral line should pass through the middle third of the capitellum on a good lateral view in most children beyond early ossification. The radiocapitellar line should follow the central axis of the radial neck and pass through the capitellum on every view. If either line seems abnormal, first check whether the view is true; then assume injury until proven otherwise.
A posterior fat pad after trauma is not a normal variant. It should trigger careful search for occult supracondylar, lateral condyle, radial neck or other elbow injury, plus immobilisation and follow-up when the clinical picture fits.
Evidence Signals
Posterior fat pad sign carries a high occult-fracture rate
- Meta-analysis of 10 studies, 250 children with a positive fat pad sign and follow-up imaging.
- Pooled occult fracture rate was 44.6 percent (95% CI 30.4 to 59.7).
- Most common occult sites: supracondylar humerus 43 percent, proximal ulna 19 percent, proximal radius 17 percent, lateral condyle 14 percent.
Age-dependent reliability of elbow alignment lines
- 200 normal paediatric elbows; the anterior humeral line passed through the middle third of the capitellum in 88.5 percent overall.
- Reliability rose with age: the AHL hit the middle third in only 25 percent of children aged 0 to 3 years versus 100 percent by 16 to 18 years.
- The radiocapitellar line crossed the middle third on the lateral view in 93 percent but only 74.5 percent on the AP view.
Anterior humeral line index outperforms Gartland for posteriorly hinged fractures
- 50 supracondylar fractures rated by 11 observers using both the Gartland classification and an AHL index.
- Interobserver agreement was higher for the AHL index (kappa 0.68) than for Gartland type (kappa 0.36); Gartland type 2 had the lowest agreement (kappa 0.27).
- AHL intraobserver reliability was almost perfect (kappa 0.83).
AHL-to-capitellum distance is the most reliable sagittal measure
- 42 children with supracondylar fractures; AC distance, Baumann angle and tilting angle were compared.
- AC distance had the highest interobserver reliability (0.84) versus Baumann angle (0.79) and tilting angle (0.46).
- Loss of correction was smaller after cross pinning than after lateral pinning.
Baumann angle alone is unreliable and view-dependent
- 141 children aged 3 to 10 years; Baumann angle ranged widely from 52 to 90 degrees.
- Around 16 percent of measurements fell outside published normal limits; one third of films were of inadequate quality.
- Out-of-range Baumann angles were far more common on inadequate films (31.1 versus 6.2 percent).
Lateral condyle fractures need oblique views and serial imaging
- 27 children with apparently non-displaced or minimally displaced lateral condyle fractures on AP radiographs.
- Internal oblique radiographs reclassified 16 of 27 as displaced over 2 mm, changing them to operative management.
- Early follow-up oblique films detected further displacement under cast in conservatively treated patients.
Developmental anatomy underpins safe elbow trauma interpretation
- Accurate reading of paediatric elbow trauma demands knowledge of developmental anatomy, ossification timing and radiographic landmarks.
- Both acute fractures and chronic overuse injuries are reviewed with their imaging signatures.
- Radiography plus MRI are framed as complementary tools for occult and chronic injury.
Secondary ossification centres are the main source of diagnostic error
- Paediatric elbow injuries are commonly misdiagnosed because of the secondary ossification centres unique to children.
- Knowing the normal appearance and sequence of ossification centres is described as crucial for accuracy.
- CT, ultrasound and MRI are useful adjuncts when radiographs are inconclusive.
Clinical Reasoning Notes
Read every paediatric elbow film in the same order. The order matters because the common failures are predictable: trusting a poor lateral, forgetting CRITOE, drawing the anterior humeral line on the wrong cortex, drawing the radiocapitellar line away from the radial neck, overlooking a posterior fat pad, or stopping at the elbow when the problem is a Monteggia lesion.
The anterior humeral line and radiocapitellar line are not slogans. They are physical landmark checks. If a diagram shows the line in the wrong place, it teaches the wrong anatomy. The anterior humeral line follows the anterior distal humeral cortex. The radiocapitellar line follows the radius, not the ulna, and it must reach the capitellum.
When the radiograph and examination disagree, respect the patient. A child with marked swelling, focal bony tenderness and a posterior fat pad needs immobilisation and review even if the fracture line is not visible. A child with nerve symptoms or poor perfusion needs urgent escalation even before the radiology report returns.
Common pitfalls
- Drawing AHL through the wrong cortex.
- Drawing RCL away from the radial neck.
- Ignoring view quality.
- Missing a posterior fat pad.
- Forgetting the medial epicondyle after dislocation.
- Not imaging the forearm in suspected Monteggia injury.
Guidelines, Registries & Global Practice
Global epidemiology
- Supracondylar humerus fracture is the most common paediatric elbow fracture, accounting for roughly 55 to 70 percent of elbow fractures in children, with a peak incidence between 5 and 7 years of age and a fall on the outstretched hand the usual mechanism.
- Lateral condyle fractures are the second most common (around 12 to 20 percent of paediatric elbow fractures); medial epicondyle avulsions follow, often associated with elbow dislocation.
- The Kappelhof meta-analysis confirms that when a post-traumatic fat pad sign is present, the occult fracture rate is high (44.6 percent), reinforcing effusion as a globally relevant warning sign.
- Distribution is broadly consistent across high- and low-resource settings, though delayed presentation and missed lateral condyle and Monteggia injuries are reported more often where access to follow-up imaging is limited.
Side-by-side guidance
| Body | Emphasis | Practical point |
|---|---|---|
| AAOS / POSNA (US) | AP and true lateral as first-line; advanced imaging only when it changes management | Comparison views of the contralateral elbow are discouraged as routine |
| BOA / BOAST (UK) | Documented neurovascular status, timely senior review and clear escalation for displaced or vascular injuries | Pulseless hand is a time-critical pathway, not a radiology decision |
| AO Foundation | Structured assessment of alignment lines and fat pads; AO/OTA paediatric coding for fracture description | Use reproducible measures (AHL position, Baumann angle) on adequate views |
| EFORT / European consensus | Caution interpreting lines and angles in the very young because ossification is incomplete | Serial radiographs and clinical correlation over single-film reassurance |
Registry and resource notes
- Paediatric elbow fractures are not tracked by arthroplasty registries; the evidence base is built from trauma series, meta-analyses and observer-reliability studies rather than implant registries.
- High-resource settings can readily obtain internal oblique views, ultrasound and MRI for equivocal cases; the priority in limited-resource settings is a true AP and lateral, disciplined use of alignment lines and fat pads, and robust safety-netting with planned re-review when advanced imaging is unavailable.
Controversies and Areas of Uncertainty
- Comparison views of the opposite elbow. Routine contralateral films were once common to "check" an ossification centre. Most paediatric bodies now discourage this because of the extra radiation dose and limited yield; reserve it for genuinely ambiguous cases where it will change management and does not delay urgent care.
- Which sagittal measure to trust. The Baumann angle is widely taught but is highly view-dependent and unreliable in isolation. The anterior humeral line position and the AHL-to-capitellum distance have better reproducibility, so several authors argue these should lead sagittal assessment.
- Grading the posteriorly hinged (Gartland type 2) fracture. Interobserver agreement on Gartland type 2 is poor. The AHL index has been proposed as a more reproducible way to decide which extension injuries need reduction, but it is not yet a universal standard.
- Imaging the occult fracture. When a fat pad sign is the only finding, practice varies between immobilise-and-review, early MRI, or ultrasound. With a 44.6 percent occult fracture rate the safe default is to treat as a fracture; advanced imaging is reserved for cases where confirming or excluding injury changes management.
- The very young elbow. In children under about four years, normal alignment lines frequently miss the middle third of the capitellum, so the under-fours remain the group where over- and under-calling are both most likely.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has elbow trauma and a posterior fat pad but no obvious fracture. What does this mean?”
“The radiocapitellar line does not cross the capitellum. What are you worried about?”
“A three-year-old has fallen on an outstretched hand. The elbow is swollen and tender but the anterior humeral line appears to pass just anterior to the capitellum. How do you interpret this?”
Sequence
- Confirm view
- CRITOE
- AHL
- RCL
- Fat pads
Lines
- AHL through capitellum on lateral
- RCL through capitellum on AP and lateral
- Baumann angle for coronal alignment
Occult Clues
- Posterior fat pad
- Anterior sail sign
- Focal tenderness
- Subtle cortical break
Do Not Miss
- Supracondylar fracture
- Lateral condyle fracture
- Medial epicondyle incarceration
- Monteggia lesion
- Neurovascular injury