Age-based treatment selection, non-accidental injury screen and alignment follow-up
- Age and weight guide treatment more than the fracture label alone.
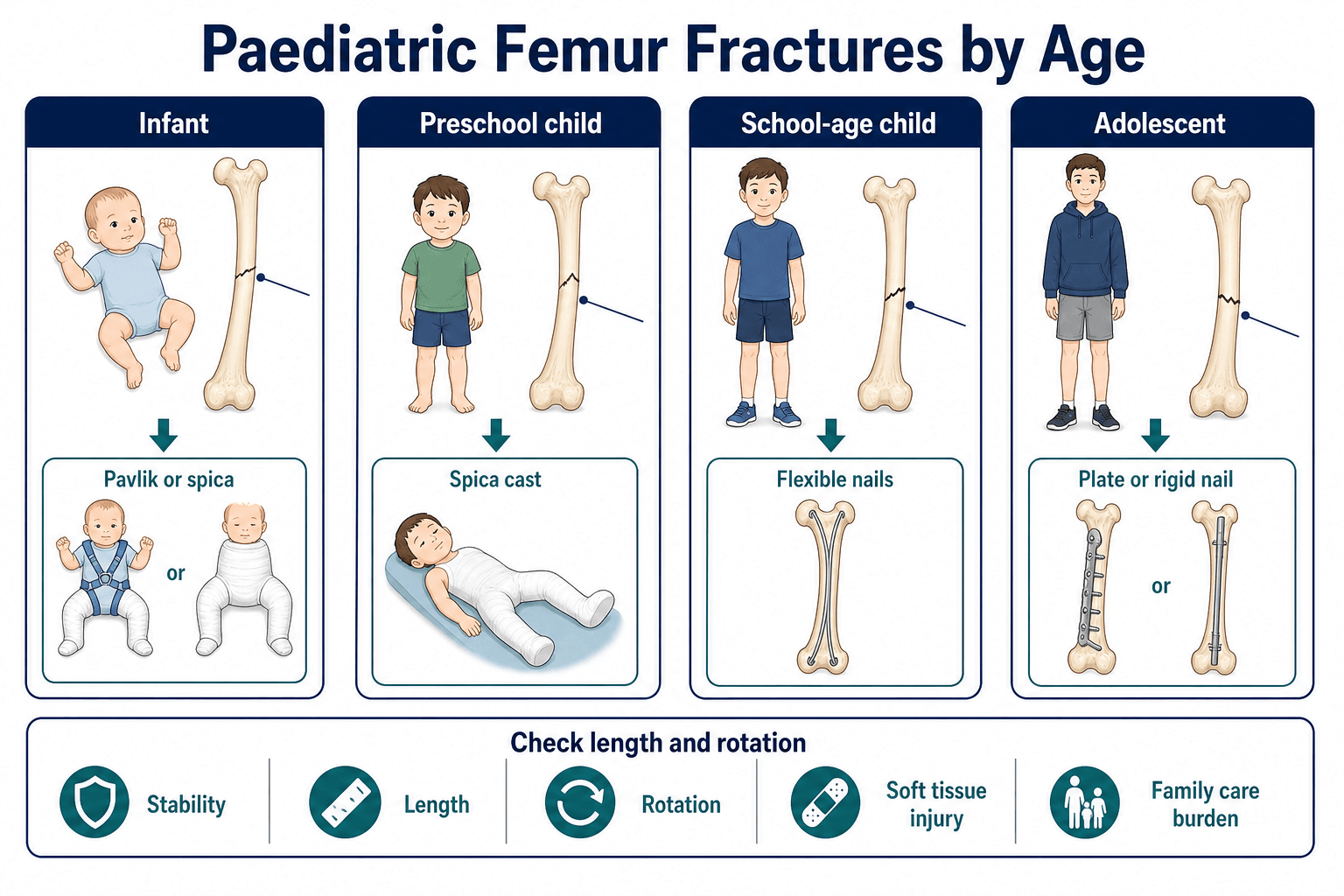
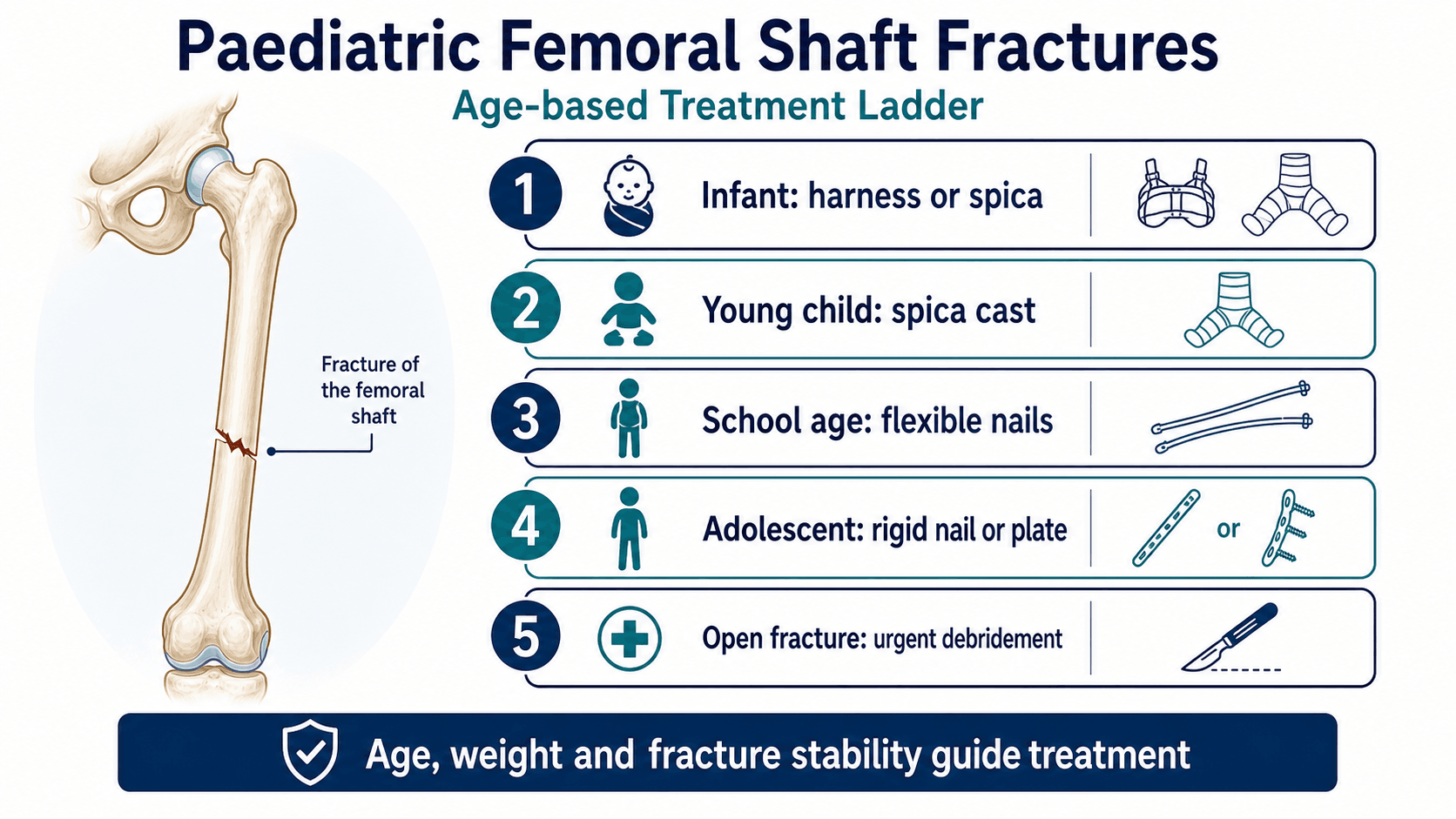
- Infants may be treated with Pavlik harness or spica depending age and pattern.
- Young children commonly do well with early spica when alignment is acceptable.
- School-age children often need flexible nails or plating depending length stability.
- Adolescents may need submuscular plating or rigid trochanteric-entry nails when appropriate.
- “Measure rotation clinically, not only on AP and lateral X-rays.
- “Length-unstable fractures are poor candidates for flexible nails alone.
- “High-energy femur fracture means look for chest, abdomen, head and other limb injuries.
- “Pain, anxiety and increasing analgesia can be compartment warning signs in children.
A femur fracture in a non-walking child is a safeguarding diagnosis until the history, developmental stage and injury pattern are reconciled. Do not focus only on implant choice.
Images and Diagrams
- Answer
- Age, weight, pattern and soft tissues
- Clinical use
- Chooses harness, spica, nails, plate or external fixation
- Answer
- Mechanism must fit developmental stage
- Clinical use
- Detects non-accidental injury and pathological fracture
- Answer
- Length, angulation and rotation
- Clinical use
- Rotation is least forgiving
- Answer
- Limb length difference and malrotation
- Clinical use
- Needs clinical and radiographic review
FEMURInitial Assessment
Hook:FEMUR keeps the decision anchored to fracture pattern, energy, maturity, urgency and rotation.
AGETreatment Ladder
Hook:AGE links treatment to growth, size, reliability and family practicality.
LARAAlignment
Hook:LARA keeps follow-up focused on length, alignment, rotation and activity recovery.
Overview/Epidemiology
Paediatric femoral shaft fracture treatment is a classic age-based topic, but age is only the start. The final plan depends on age, weight, skeletal maturity, fracture pattern, length stability, soft tissues, associated injuries, mechanism, safeguarding concerns and the family’s ability to manage immobilisation and follow-up.
Younger children heal quickly and remodel well, but they also need careful assessment of whether the mechanism fits developmental ability. School-age children sit in the transition zone where spica casting may be burdensome and operative stabilisation is often attractive. Adolescents behave more like adults mechanically, but many still have open physes, so implant entry point and growth safety remain important.
The major pattern distinction is length-stable versus length-unstable. A transverse or short oblique fracture may be well suited to flexible intramedullary nails in an appropriately sized child. A long oblique, spiral, comminuted or segmental fracture is more likely to shorten and may need submuscular plating, external fixation or another stability strategy.
Outcome is not just radiographic union. A good result includes acceptable length, rotation, angulation, hip and knee motion, skin integrity, family functioning, safe return to activity and no missed safeguarding or polytrauma issue.
Pathophysiology
The biology explains why children can often be treated differently from adults, but it also explains the complications.
- Clinical meaning
- Vascular bone and active periosteum produce reliable callus.
- Treatment implication
- Younger children can often be treated with harness or spica if alignment is acceptable.
- Clinical meaning
- Femoral overgrowth can occur after shaft fracture, especially in younger children.
- Treatment implication
- Some shortening may be accepted, but it should be deliberate and followed.
- Clinical meaning
- Rotational deformity remodels poorly.
- Treatment implication
- Assess rotation clinically after reduction or fixation, not only on AP/lateral X-rays.
- Clinical meaning
- Long oblique, spiral, comminuted and segmental patterns can shorten under load.
- Treatment implication
- Flexible nails alone may be insufficient; consider plating or a more stable construct.
- Clinical meaning
- Flexible nails are load-sharing; submuscular plates provide relative stability; rigid nails require safe entry points.
- Treatment implication
- Match construct to age, weight, fracture pattern and open physes.
- Clinical meaning
- Open fractures, severe swelling and polytrauma change priorities.
- Treatment implication
- Open-fracture care, external fixation or damage-control stabilisation may come before definitive fixation.
- Clinical meaning
- Cysts, tumour, metabolic bone disease and osteogenesis imperfecta change healing and fixation.
- Treatment implication
- Treat the lesion and bone-health diagnosis, not just the shaft fracture.
Classification
- Infant: Pavlik harness or spica for selected patterns.
- Toddler and preschool: early spica is common when reduction is acceptable.
- School-age child: flexible nails for length-stable fractures, plate for length-unstable patterns.
- Older adolescent: submuscular plate or trochanteric-entry rigid nail when maturity and anatomy permit.
Clinical Presentation
History
The history should place the fracture in the context of the whole child.
- Ask specifically
- Fall, twisting injury, road trauma, sport, high-energy crush or low-energy event.
- Why it matters
- High-energy trauma triggers whole-child assessment; low-energy fracture raises pathology or safeguarding questions.
- Ask specifically
- Walking status and whether the mechanism matches age and ability.
- Why it matters
- Femur fracture in a non-walking child needs safeguarding and bone fragility review.
- Ask specifically
- Head, chest, abdomen, pelvis, hip, knee or other limb pain.
- Why it matters
- Femur fracture can coexist with femoral neck fracture, floating knee, pelvic or visceral injury.
- Ask specifically
- Previous fractures, bone pain, cyst, metabolic bone disease, malignancy or osteogenesis imperfecta features.
- Why it matters
- Pathological fractures need diagnosis-specific treatment.
- Ask specifically
- Traction, splinting, analgesia, time since injury and transfer details.
- Why it matters
- Defines pain control, skin risk and urgency.
- Ask specifically
- Spica care, transport, toileting, skin checks, sleep, stairs and car-seat issues.
- Why it matters
- A spica is safe only if the family can manage the child at home.
Examination
Perform a paediatric trauma assessment before discussing implant choice.
- Assess
- Airway, breathing, circulation, head, chest, abdomen, pelvis and other limbs.
- Why it matters
- A femur fracture may be one marker of major trauma.
- Assess
- Swelling, deformity, shortening, external rotation, open wound, bruising pattern and threatened skin.
- Why it matters
- Changes urgency, open-fracture pathway and fixation choice.
- Assess
- Distal perfusion plus sciatic, peroneal and tibial nerve function where testable.
- Why it matters
- Documents baseline and detects vascular or nerve injury.
- Assess
- Hip, knee, tibia and pelvis.
- Why it matters
- Avoid missed femoral neck fracture, distal physeal injury, floating knee or pelvic injury.
- Assess
- Pain behaviour, anxiety, increasing analgesia, swelling and pain with passive stretch when assessable.
- Why it matters
- Children may not describe classic compartment symptoms.
- Assess
- Foot progression, thigh-foot profile and hip rotation compared with the other side.
- Why it matters
- Malrotation is poorly seen on plain films and remodels poorly.
Treatment by age is shorthand. The real decision is age plus size, pattern, soft tissues, stability, safeguarding and family practicality.
Investigations
- Investigation
- AP and lateral femur including hip and knee
- Decision it informs
- Defines level, pattern, shortening and associated joint injury
- Investigation
- Trauma imaging as indicated by paediatric trauma team
- Decision it informs
- Finds head, chest, abdomen, pelvis or other limb injuries
- Investigation
- Full-length radiographs and lesion-specific MRI or labs
- Decision it informs
- Identifies cyst, tumour or bone fragility
- Investigation
- Clinical profile, CT only when necessary
- Decision it informs
- Quantifies malrotation when clinical assessment is unreliable
- Always include hip and knee on femur imaging.
- Look for distal femoral physeal injury and femoral neck injury in high-energy trauma.
- A spiral femur fracture is not automatically abuse, but the mechanism must fit.
- Post-treatment X-rays should confirm length, angulation and implant position.
- Follow-up imaging checks union and maintenance of alignment.
Differential Diagnosis
- Clue
- High-energy injury, hip/knee pain or fracture line near joint.
- Why it matters
- Needs different reduction accuracy, fixation and complication follow-up.
- Clue
- Cyst, lytic lesion, previous pain, low-energy mechanism or abnormal bone quality.
- Why it matters
- Treat the lesion and fracture together.
- Clue
- Non-ambulant child, inconsistent story, delay or other injuries.
- Why it matters
- Activate safeguarding pathway while treating pain and fracture.
- Clue
- Osteogenesis imperfecta, metabolic bone disease or recurrent fractures.
- Why it matters
- Changes fixation, follow-up and family counselling.
- Clue
- Young child localises poorly and may appear to have thigh pain.
- Why it matters
- Prevents over-investigation or missing tibial tenderness.
- Clue
- Road trauma, fall from height or crush injury.
- Why it matters
- Look for head, chest, abdomen, pelvis and floating knee injuries.
Management
Treatment is a ladder, not a single rule. Start with analgesia, splintage, skin and neurovascular care, and whole-child assessment. Then choose definitive treatment based on age, size, pattern and context.
- Usual direction
- Pavlik harness or spica for selected closed injuries.
- When to change course
- Safeguarding, pathological fracture, polytrauma or unacceptable alignment changes the pathway.
- Usual direction
- Early spica is common when reduction is acceptable and family care is practical.
- When to change course
- Obesity, polytrauma, open injury, unacceptable shortening or family constraints may favour operative treatment.
- Usual direction
- Flexible intramedullary nails in suitable size/weight.
- When to change course
- Avoid flexible nails alone for unstable long oblique, spiral, comminuted or segmental patterns.
- Usual direction
- Submuscular plate or other stable construct.
- When to change course
- Flexible nails risk shortening, malalignment and reoperation.
- Usual direction
- Submuscular plate or lateral trochanteric-entry rigid nail depending anatomy.
- When to change course
- Avoid piriformis entry in skeletally immature children because of femoral head blood supply risk.
- Usual direction
- Antibiotics, tetanus, debridement and damage-control or definitive stabilisation as appropriate.
- When to change course
- Soft tissues and physiology decide timing more than age alone.
Acceptable deformity by age (what "acceptable alignment" actually means)
Remodelling potential falls with age, so the tolerated deformity narrows as the child gets older. Younger children also overgrow, so bayonet shortening of up to ~1.5–2 cm is deliberately accepted in the under-10s. Rotation remodels poorly at every age and is not "accepted" — it must be corrected.
- Varus/valgus
- 30°
- Anterior/posterior angulation
- 30°
- Shortening
- 15 mm
- Varus/valgus
- 15°
- Anterior/posterior angulation
- 20°
- Shortening
- 20 mm
- Varus/valgus
- 10°
- Anterior/posterior angulation
- 15°
- Shortening
- 15 mm
- Varus/valgus
- 5°
- Anterior/posterior angulation
- 10°
- Shortening
- 10 mm
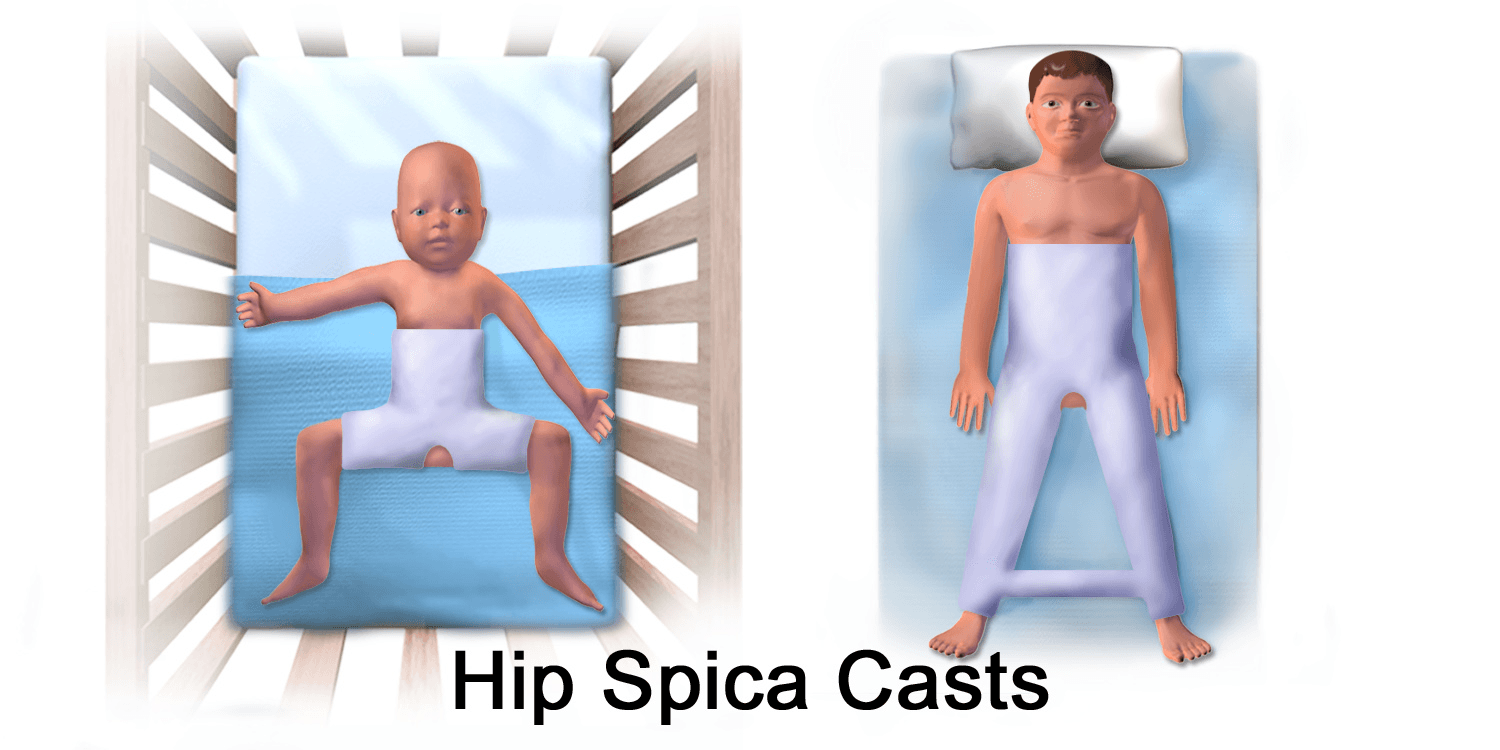
Applying an early hip spica with excessive traction and the knee/hip in marked (90-90) flexion — particularly using a leg-holder and traction during casting — can cause leg (calf) compartment syndrome of the casted limb, a recognised and limb-threatening complication. The modern trend is less flexion, no excessive traction, and a single-leg ("walking") spica for isolated low-energy femoral fractures, with vigilant neurovascular and skin checks after casting.
- Provide analgesia and temporary splintage or traction.
- Screen for non-accidental injury when age and mechanism require it.
- Use Pavlik harness in selected infants.
- Use early spica for many toddler and preschool fractures with acceptable alignment.
- Educate family on skin care, hygiene, transport and return precautions.
Complications
Early
- Compartment syndrome.
- Skin breakdown or cast problems.
- Loss of reduction or shortening.
- Open fracture infection.
- Associated injuries missed in polytrauma.
Late
- Malrotation.
- Limb length discrepancy from overgrowth or shortening.
- Knee stiffness after flexible nailing or immobilisation.
- Refracture after early implant removal.
- AVN risk with inappropriate rigid nail entry.
The X-ray heals faster than the child returns to normal life. Rotation, limb length, gait and family burden all need review.
Decision-Making in Practice
Age-based paediatric femoral shaft fracture treatment is a shortcut for a larger decision: age, weight, fracture stability, soft tissues, mechanism, family care capacity and associated injuries. The wrong operation for the wrong age or fracture pattern creates malunion, malrotation, skin problems or avoidable reoperation.
- What it suggests
- Rapid healing and high remodelling, but safeguarding must be considered
- Treatment implication
- Pavlik harness or spica in selected cases
- What it suggests
- Spica often effective if alignment and care are practical
- Treatment implication
- Early spica versus selective surgery
- What it suggests
- Transverse or short oblique pattern in suitable weight range
- Treatment implication
- Flexible intramedullary nails are often appropriate
- What it suggests
- Long oblique, spiral, comminuted or segmental fracture
- Treatment implication
- Submuscular plate or other stable construct may be better than flexible nails alone
- What it suggests
- Near adult size and maturity
- Treatment implication
- Trochanteric-entry rigid nail or plating depending physis and anatomy
- What it suggests
- Soft-tissue injury, contamination or unstable physiology
- Treatment implication
- Debridement, antibiotics and damage-control fixation when needed
- Safe answer
- Check clinically after reduction or fixation.
- Common failure
- Accepting AP/lateral alignment while missing malrotation.
- Safe answer
- Match fixation to length stability, weight and comminution.
- Common failure
- Flexible nails in a fracture that predictably shortens.
- Safe answer
- Confirm transport, toileting, skin checks, sleep, stairs and seating.
- Common failure
- Discharge with a cast the family cannot safely manage.
- Safe answer
- Mechanism, age, delay and associated injuries must reconcile.
- Common failure
- Focusing on fracture treatment while missing child safety.
- Safe answer
- Shortening, overgrowth, malrotation, angulation, infection, stiffness and refracture risk.
- Common failure
- Stopping follow-up at union only.
Clinical Reasoning Notes
- Practical meaning
- Use age and size to narrow the safe options.
- Pitfall
- Choosing your favourite implant before assessing the child.
- Practical meaning
- Look for head, chest, abdomen, pelvis, femoral neck and knee injuries.
- Pitfall
- Treating the femur while missing polytrauma.
- Practical meaning
- Skin, toileting, transport, sleep and seating must be safe.
- Pitfall
- Calling spica non-operative but ignoring family burden.
- Practical meaning
- Use them where the fracture can resist shortening.
- Pitfall
- Using nails for unstable comminution without a plan for length.
- Practical meaning
- Compare clinical rotation, not only radiographs.
- Pitfall
- Missing malrotation until gait review.
- Practical meaning
- Review gait, limb length, rotation, stiffness, implant irritation and return to activity.
- Pitfall
- Assuming callus equals recovery.
Common pitfalls
- Choosing treatment from age alone.
- Missing non-accidental injury.
- Ignoring femoral neck or knee associated injury.
- Using flexible nails for an unstable comminuted fracture without plan for shortening.
- Not checking rotation.
- Discharging a spica family without practical education.
Guidelines, Registries & Global Practice
Paediatric femoral shaft fractures are common worldwide, but implants, resources and pathways differ. The principles below let you defend a plan in any examination system.
Global epidemiology
- Femoral shaft fractures account for roughly 1.5 to 2% of all paediatric fractures, with a bimodal age distribution: a peak in toddlers (often low-energy or non-accidental) and a second peak in adolescents (high-energy).
- There is a consistent male predominance and a strong association of the youngest fractures with non-accidental injury (see Clarke et al, Injury 2012).
- In a non-ambulant infant, abuse rather than implant choice is the dominant clinical question.
Side-by-side guidance
- Emphasis
- Age-banded clinical practice guideline; mandatory abuse evaluation under 36 months; flexible nailing as an option ages 5 to 11.
- Practical signal
- Best-known structured age framework, though several recommendations are weak/inconclusive.
- Emphasis
- Open-fracture and major-trauma standards stress early senior review, analgesia, neurovascular documentation and safeguarding.
- Practical signal
- Process and safeguarding standards rather than implant prescription.
- Emphasis
- Construct-stability principles: relative versus absolute stability, canal fill, submuscular plating technique and safe nail entry.
- Practical signal
- Strong technical guidance for length-unstable and complex fractures.
- Emphasis
- Reinforces age-based selection with growing role of operative fixation in school-age children.
- Practical signal
- Broadly convergent with AAOS, with regional implant preferences.
Registry and outcome notes
- Paediatric femoral shaft fractures are not tracked in arthroplasty registries (NJR, AJRR, AOANJRR), so evidence comes from institutional series and meta-analyses rather than implant-survival registries.
- The most robust comparative evidence is from systematic reviews of flexible nailing versus submuscular plating (Hu et al 2023; Liu et al 2024), which show comparable union and complication trade-offs rather than a single superior implant.
High-resource versus limited-resource practice
- Typical pathway
- Early spica, flexible nails, submuscular plates and image intensifier readily available.
- Reason
- Shorter admissions and early mobilisation are prioritised.
- Typical pathway
- Greater reliance on traction (gallows for infants, skin/skeletal traction for older children) and delayed spica.
- Reason
- Fewer theatre slots, implants and intensifier access make non-operative care safer and more practical.
- Typical pathway
- Safeguarding screening for non-ambulant children and whole-child trauma assessment are non-negotiable.
- Reason
- Child safety and missed polytrauma do not depend on resources.
Controversies and Areas of Uncertainty
The age-based framework hides several genuinely contested decisions. These are the points examiners use to separate a safe trainee from a thinking one.
- Arguments on each side
- Classic teaching warns against flexible nails over about 49 kg; newer series (Atassi) report good results in lighter unstable fractures with full canal fill.
- Pragmatic position
- Weight is a relative, not absolute, contraindication; combine weight, pattern and canal fill rather than a single cut-off.
- Arguments on each side
- Meta-analyses show plating has fewer complications and less implant irritation; nails have shorter surgery and less blood loss.
- Pragmatic position
- Default to plating for comminuted/heavier patterns; reserve nails for length-stable or lighter children, locking the nails if unstable.
- Arguments on each side
- Immediate spica shortens admission; some advocate short traction first to limit unacceptable shortening.
- Pragmatic position
- Immediate spica is reasonable when shortening is under 2 cm and the family can manage care.
- Arguments on each side
- Some accept up to 2 cm shortening anticipating overgrowth; others find overgrowth unpredictable.
- Pragmatic position
- Accept small shortening deliberately and follow limb length; do not rely on overgrowth to rescue a poor reduction.
- Arguments on each side
- Trochanteric/lateral entry reduces but does not abolish AVN and abductor risk; piriformis entry is unsafe in the immature femur.
- Pragmatic position
- Use lateral trochanteric entry only near skeletal maturity; never piriformis entry with an open physis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you choose treatment for paediatric femoral shaft fracture?”
“A nine-month-old has a femur fracture after a vague fall story. What do you do?”
“A 10-year-old weighing 45 kg has a comminuted, length-unstable mid-shaft femoral fracture. How would you fix it and why?”
Age Ladder
- Infant harness/spica
- Toddler spica
- School-age flexible nails or plate
- Adolescent plate or rigid nail selected
Assess
- Trauma survey
- Skin
- Nerves and vessels
- Mechanism fit
- Pattern stability
Complications
- Malrotation
- LLD
- Cast sores
- Knee stiffness
- Infection
Do Not Miss
- NAI
- Open fracture
- Femoral neck injury
- Floating knee
- Pathological fracture
Evidence Signals
AAOS clinical practice guideline anchors age-based care
- Children younger than 36 months with a femoral shaft fracture should be evaluated for child abuse.
- Early spica casting or traction with delayed spica is an option for children aged 6 months to 5 years with shortening less than 2 cm.
- Flexible intramedullary nailing is recommended as a treatment option for children aged 5 to 11 years.
- Pre-operative and post-operative documentation should screen for neurovascular injury and leg-length discrepancy.
AAOS guideline adherence is high but did not change outcomes
- Retrospective review of 361 paediatric diaphyseal femur fractures across 2007 to 2012.
- Publication of the 2009 AAOS guideline produced little overall change in treatment selection.
- The only significant shift was a decrease in flexible nailing in children aged 5 to 11 years, contrary to that specific recommendation.
Flexible nails perform well even in length-unstable patterns
- 101 paediatric femoral shaft fractures (mean age 7 years, mean weight 29 kg) treated with flexible elastic nailing.
- 51 of 101 (50%) were length-unstable patterns; all fractures united.
- No revision for malunion: 3 had malrotation greater than 15 degrees, none had leg-length inequality over 1 cm.
- No patient, fracture or treatment characteristic (including instability) predicted complications.
Locking flexible nails controls shortening in unstable fractures
- 107 length-unstable femoral shaft fractures fixed with Enders rods; 37 (35%) locked with a distal cortical screw.
- Locked rods migrated only 1.3 to 1.9 mm versus 12.1 mm for unlocked rods (p less than 0.05).
- Non-locked cases had significantly more limp, clinical shortening and painful palpable rods at follow-up.
- Locking added no extra operative time, blood loss or complications.
Submuscular bridge plating is reliable for complex fractures
- 51 patients (mean age 10 years); 67% high-energy and 55% unstable patterns.
- All fractures united with maintenance of length and alignment, allowing early functional treatment without casting.
- Only 2 significant complications (4%): one plate fracture and one refracture of a pathological fracture after early removal.
- Leg-length discrepancy ranged from 23 mm short to 10 mm long in 4 patients (8%).
ESIN versus submuscular plate: meta-analysis of school-age fractures
- 8 studies, 561 patients comparing elastic stable intramedullary nailing (ESIN) with submuscular plate (SMP).
- ESIN had shorter operative time and less blood loss.
- ESIN had higher implant irritation (OR 6.49), more malalignment (OR 2.60) and more overall complications (OR 4.14).
- No significant difference in limb-length discrepancy, infection, delayed union or unplanned revision.
A femur fracture in a non-ambulant infant is a red flag for abuse
- Incidence of 53 fractures per 10,000 children under 2 years over a 2-year period.
- Femur and skull fractures in the youngest children were most strongly associated with child-protection referral.
- Risk factors for abuse: age under 12 months, non-ambulatory status, delayed presentation, inconsistent history and other injuries.
- Time interval between injury and presentation was unrecorded in 34% of cases, a key documentation failure.
Evidence Base
ESIN versus plate: complication trade-offs
- 10 studies, 775 paediatric diaphyseal femur fractures (428 ESIN, 347 plate).
- ESIN had shorter surgery, less blood loss, but longer fracture healing time.
- Prominent/irritating implants were markedly more common with ESIN (RR 3.36).
- Infection and angulation deformity rates were similar between constructs.
Stainless-steel flexible nails for unstable fractures need cortical abutment
- 41 stable versus 40 unstable femoral shaft fractures fixed with single-lateral Ender nails.
- All fractures healed at a mean of 1.4 months with no infections or refractures.
- Only minor angular deformities, with no clinically detectable malalignment in either group.
- One Winquist grade IV comminuted fracture developed a 3 cm leg-length difference.
AAOS guideline checklist adherence in practice
- 313 children reviewed after embedding AAOS-based checklists into the EMR order set.
- 89.9% received age-appropriate treatment consistent with the AAOS guideline after implementation.
- Complication rates were identical (12%) before and after checklist implementation.
- Standardised checklists improved process documentation but not outcomes.
Paediatric biology principle: remodelling, overgrowth and rotation
- Coronal and sagittal angulation remodel with growth, especially near the physis and in younger children.
- Rotational deformity does NOT remodel and must be corrected at treatment.
- Femoral overgrowth of roughly 1 to 2 cm can follow shaft fracture in young children, supporting a small deliberate shortening (under 2 cm) in some spica-treated cases.