Anabolic Steroids, Stimulants & 'Doping'
- PERFORMANCE- and APPEARANCE-ENHANCING DRUGS/substances ('DOPING') include ANABOLIC-ANDROGENIC STEROIDS (AAS) and STIMULANTS, as well as GROWTH HORMONE, DIURETICS (for weight/masking), erythropoietin/blood doping, and various SUPPLEMENTS - an ethical and health issue in sport, and recognising their use is important so athletes receive appropriate care and education.
- ANABOLIC-ANDROGENIC STEROIDS increase muscle mass and strength but cause a wide range of SERIOUS, sometimes PERMANENT, ADVERSE EFFECTS: CARDIOVASCULAR (cardiomyopathy, hypertension, dyslipidaemia, thrombosis), HEPATIC (cholestasis and hepatic tumours, especially with oral 17-alpha-alkylated agents), RENAL disease, ENDOCRINE (testicular atrophy/hypogonadism, gynaecomastia, virilisation in women), and PSYCHIATRIC effects (aggression/'roid rage', mood disturbance, dependence), plus acne and premature physeal closure/stunted growth in adolescents.
- The key ORTHOPAEDIC adverse effect is TENDON RUPTURE - classically of the PECTORALIS MAJOR, and also the Achilles, quadriceps/patellar and biceps tendons - so unexpected or bilateral tendon ruptures in a muscular athlete should raise the possibility of AAS use.
- STIMULANTS (e.g. amphetamines, certain pre-workout agents) enhance alertness and performance but carry CARDIOVASCULAR risks (palpitations, hypertension, arrhythmia, and a contribution to sudden cardiac events) and increase the risk of HEAT illness/dehydration; signs of doping more broadly can mimic other health concerns (palpitations, acne, mood change, headaches, cramps).
- Doping can lead to SEVERE and sometimes PERMANENT ORGAN DAMAGE - including liver, kidney and heart disease - and recognising appearance/performance-enhancing substance use is important so that athletes (including adolescents) receive the care, treatment and EDUCATION needed to reduce these health risks.
- BE CAREFUL WITH THE MECHANISM - IT IS ASSERTED MORE OFTEN THAN DEMONSTRATED. The familiar explanation is that steroids strengthen MUSCLE disproportionately to TENDON, so the tendon fails. The bodybuilder series most often cited for the association proposes something different: that anabolic steroid use contributes to the injury through an EXCESSIVE UPWARD ADJUSTMENT OF THE ATHLETE'S LIFTING GOALS - a BEHAVIOURAL route, not a demonstrated change in tendon material properties. Both remain hypotheses; present the association confidently and the mechanism tentatively.
- CONTINUED STEROID USE DID NOT SPOIL THE REPAIR. In that series of 6 male bodybuilders with pectoralis major rupture, all treated surgically had EXCELLENT results by Bak criteria and returned to full activity at a mean of 5.4 MONTHS (5 to 7), with NO postoperative complications DESPITE CONTINUED anabolic steroid use, and suture-anchor fixation succeeded REGARDLESS OF THE CHRONICITY of the repair. That argues against both an assumption that ongoing use wrecks tendon healing and a reflex urgency about operating early - though with 6 patients and 16 months' mean follow-up it settles neither.
- THE CARDIAC RISK IS NOT ABSTRACT. In that same series of six, ONE PATIENT DIED OF MYOCARDIAL INFARCTION WITHIN A YEAR of surgery. A single death in six is not an incidence figure, but it is a reminder that the tendon is the visible problem while the cardiovascular disease is the one that kills - so the consultation should extend to cardiovascular assessment rather than ending at the repair.
- MANAGEMENT and the wider response are RECOGNITION (clinical signs, the orthopaedic clue of tendon rupture), honest counselling and treatment of the health consequences, compliance with the ANTI-DOPING (WADA) framework, and EDUCATION/PREVENTION - fostering an anti-doping culture among athletes, coaches and clinicians; the orthopaedic surgeon's role includes recognising the doping athlete behind a tendon rupture and addressing the underlying issue.
- “Doping = performance/appearance-enhancing substances: ANABOLIC-ANDROGENIC STEROIDS, STIMULANTS, GH, diuretics, supplements (WADA-prohibited).
- “Anabolic steroids: strength gain BUT serious harms - cardiovascular (cardiomyopathy/hypertension/dyslipidaemia), hepatic (cholestasis/tumours - oral 17-alkylated), endocrine (hypogonadism/gynaecomastia/virilisation), psychiatric ('roid rage'/dependence), adolescent physeal closure.
- “KEY orthopaedic clue: increased TENDON RUPTURE risk (pectoralis major, Achilles, quadriceps) - suspect AAS in an unexpected/bilateral tendon rupture in a muscular athlete. Stimulants -> cardiovascular/heat risk. Response = recognition + anti-doping (WADA) + education/prevention; severe/permanent organ damage.
Anabolic steroids: cardiovascular (cardiomyopathy/hypertension), hepatic (cholestasis/tumours), endocrine (hypogonadism/gynaecomastia/virilisation), psychiatric ('roid rage'/dependence); adolescent physeal closure.
Increased tendon rupture risk (pectoralis major, Achilles, quadriceps) - suspect AAS in an unexpected/bilateral rupture in a muscular athlete. Stimulants -> cardiovascular/heat risk.
Substances, Harms & Response
'Doping' is the use of performance/appearance-enhancing substances - principally anabolic-androgenic steroids (AAS) and stimulants, also growth hormone, diuretics and supplements. AAS increase muscle mass and strength but cause serious, sometimes permanent harms: cardiovascular (cardiomyopathy, hypertension, dyslipidaemia, thrombosis), hepatic (cholestasis/tumours - oral 17-alkylated agents), renal, endocrine (hypogonadism, gynaecomastia, virilisation), psychiatric ('roid rage', mood, dependence), and physeal closure in adolescents. The key orthopaedic clue is an increased tendon rupture risk - classically the pectoralis major (also Achilles, quadriceps/patellar) - so an unexpected or bilateral tendon rupture in a muscular athlete should raise AAS use. Stimulants add cardiovascular and heat risk. The response is recognition, treatment of harms, anti-doping (WADA) compliance and education/prevention.
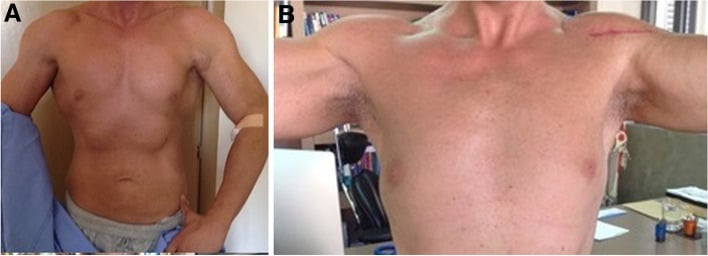
For the orthopaedic surgeon, performance-enhancing drug use often becomes relevant through its musculoskeletal consequence. Anabolic-androgenic steroid use is associated with tendon rupture, whether because muscle strength outpaces the tendon or, as the published bodybuilder series suggests, because the athlete keeps raising the load - so an unexpected, spontaneous or bilateral tendon rupture - classically of the pectoralis major, but also the Achilles, quadriceps/patellar or biceps - in a notably muscular athlete should prompt consideration of anabolic-steroid use. Recognising this matters not only for the injury but for the athlete's wider health, because doping can cause severe and sometimes permanent organ damage - cardiomyopathy and other cardiovascular disease, hepatic cholestasis and tumours, renal disease - and serious endocrine and psychiatric effects, with stimulants adding cardiovascular and heat-illness risk; in adolescents, anabolic steroids can cause premature physeal closure and stunted growth. The clinician's role is therefore to recognise the doping athlete, treat the injury and the health consequences honestly, counsel and educate, and work within the anti-doping framework to foster an anti-doping culture - rather than treating the tendon rupture in isolation.
The tendons involved each have their own page: pectoralis major rupture is the classic, with Achilles tendon rupture, quadriceps tendon rupture and distal biceps rupture the others to know. The cardiovascular risk that killed one patient in the cited series belongs with sudden cardiac death in athletes.
The Other Doping Classes: EPO, Growth Hormone, Beta-Blockers, Diuretics
- Erythropoietin (EPO) / blood doping. EPO, blood transfusion, or hypoxia-mimetics raise the red-cell mass/haematocrit → more oxygen-carrying capacity and endurance; the harm is raised blood viscosity (hyperviscosity) → thrombosis (DVT/PE, stroke, myocardial infarction) - implicated in athlete deaths - plus hypertension.
- Growth hormone (hGH). Claimed anabolic/recovery benefit (the ergogenic evidence is actually weak); harms are acromegalic soft-tissue/bony overgrowth (coarse features, enlarged jaw/hands/feet), carpal tunnel syndrome, arthralgia/joint swelling and fluid retention, and insulin resistance/diabetes - several of these orthopaedically relevant.
- Beta-blockers. Reduce heart rate and tremor, so they are banned specifically in precision/aiming sports (archery, shooting) where a steady hand matters - they are not ergogenic in endurance or power sport.
- Diuretics. Used both to make weight (rapid fluid loss) and as masking agents (diluting the urine to hide other prohibited drugs); harms are dehydration, electrolyte disturbance and cramps.
Q: Beyond anabolic steroids and stimulants, what are the other doping classes and their effects/harms?
A: EPO/blood doping raises red-cell mass/haematocrit → endurance, but hyperviscosity → thrombosis (DVT/PE/stroke). Growth hormone claims anabolic benefit (weak evidence); harms = acromegalic overgrowth, carpal tunnel, arthralgia, insulin resistance. Beta-blockers reduce tremor → banned in aiming/precision sports (archery/shooting). Diuretics are used to make weight and as masking agents (diluting urine).
The WADA Anti-Doping Framework
- The Prohibited List. WADA (World Anti-Doping Agency) publishes an annual Prohibited List of banned substances and methods (some prohibited at all times, others in-competition only); a substance is included if it meets at least two of three criteria - performance enhancement, health risk, or violating the spirit of sport.
- Strict liability. The athlete is responsible for any prohibited substance found in their sample regardless of intent or how it got there - so a violation needs no proof of fault, which is why contaminated supplements are a real hazard.
- Therapeutic Use Exemption (TUE). Allows an athlete to use an otherwise-prohibited substance for a legitimate medical condition (e.g. insulin for diabetes) if the criteria are met and it is approved in advance.
- Athlete Biological Passport (ABP). Longitudinal monitoring of an athlete's own biological markers over time - a haematological module (haemoglobin/reticulocytes for blood doping/EPO) and a steroidal module (urinary steroid profile) - detecting doping indirectly through deviations from the athlete's baseline rather than the drug itself; testing is both in- and out-of-competition.
Q: What are the key elements of the WADA anti-doping framework?
A: The Prohibited List (banned substances/methods, at-all-times or in-competition; included if it meets at least two of performance-enhancement/health-risk/spirit-of-sport). Strict liability - the athlete is responsible for anything in their sample regardless of intent (hence the supplement-contamination hazard). Therapeutic Use Exemption (TUE) for a legitimate medical need (e.g. insulin). The Athlete Biological Passport - longitudinal monitoring (haematological + steroidal modules) detecting doping indirectly via baseline deviations; in- and out-of-competition testing.
What the Bodybuilder Series Actually Found
The tendon-rupture association is repeated everywhere with a confident mechanism attached: steroids build muscle faster than tendon, so the tendon fails. The series most often cited for that association reaches a different conclusion. In six male bodybuilders who ruptured the pectoralis major during weightlifting, the authors suggest anabolic steroid use contributes through an excessive upward adjustment of the athlete's lifting goals - the athlete simply loads more - rather than through any demonstrated change in tendon material properties. They also observed that the injury was probably not related to limb dominance. Neither mechanism is proven, so the honest position is a confident association with a tentative explanation.
All six were treated surgically and had excellent results by Bak criteria, returning to full activity at a mean of 5.4 months (5 to 7). There were no postoperative complications despite continued anabolic steroid use, and suture-anchor fixation succeeded regardless of the chronicity of the repair. That cuts against both the assumption that ongoing use ruins tendon healing and any reflex urgency about operating early - though six patients at 16 months' mean follow-up settle neither question.
Within a year of surgery, one patient in that series died of a myocardial infarction. One death in six is not an incidence, but it is the proportion worth carrying: the tendon is the visible problem and the cardiovascular disease is the one that kills. A pectoralis rupture in a heavily muscled lifter is a reason to ask about cardiovascular symptoms and arrange assessment, not simply to book the repair.
Mnemonics & Memory Aids
STEROIDS
Hook:STEROIDS: Stimulants/Steroids, Tendon rupture, Endocrine effects, 'Roid rage, Organ damage, Identify the athlete, Doping (WADA)/education, Stimulant CV/heat risk.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A very muscular gym athlete sustains a pectoralis major rupture with little provocation. What should you suspect, and what are the wider concerns?”
The substances
- Anabolic-androgenic steroids; stimulants
- Growth hormone; diuretics (weight/masking); erythropoietin/blood doping; supplements
- WADA-prohibited; an ethical and health issue in sport
Anabolic-steroid harms
- Cardiovascular: cardiomyopathy, hypertension, dyslipidaemia, thrombosis
- Hepatic (cholestasis/tumours - oral 17-alkylated); renal disease
- Endocrine (hypogonadism/gynaecomastia/virilisation); psychiatric ('roid rage'/dependence); adolescent physeal closure
Orthopaedic relevance
- TENDON RUPTURE (pectoralis major, Achilles, quadriceps/patellar, biceps) - association firm, mechanism debated
- Suspect AAS in an unexpected/bilateral rupture in a muscular athlete; repair did well despite continued use (6 cases)
- One of those six died of a myocardial infarction within a year - assess the cardiovascular risk too
- Stimulants: cardiovascular (palpitations/arrhythmia) + heat-illness risk
Response
- Recognition (signs can mimic other conditions)
- Treat injury + health consequences; honest counselling
- Anti-doping (WADA) framework + education/prevention (anti-doping culture)
Evidence & Key Studies
Appearance- and performance-enhancing drugs and substances - recognition and prevention
- Commonly used appearance/performance-enhancing substances ('doping') include anabolic-androgenic steroids, stimulants, diuretics, growth hormone and supplements.
- Signs and symptoms can mimic other health concerns (palpitations, stunted growth, acne, severe headaches, muscle cramps, dizziness, dehydration), and some effects are severe and long-term.
- Doping can lead to severe and sometimes permanent organ damage, including liver, kidney and heart disease; recognition, treatment and education/prevention (fostering an anti-doping culture) are important.
Pectoralis major rupture in body builders: a case series including anabolic steroid use
- Six male bodybuilding athletes who sustained a pectoralis major rupture during weightlifting, with the location and type of injury, the history and type of anabolic steroid use, the method of repair and the outcome recorded. Mean follow-up was 16 months (12 to 24).
- All patients treated surgically had excellent results by Bak criteria and returned to full activity at a mean of 5.4 months (5 to 7). No postoperative complications occurred despite continued anabolic steroid use, and suture-anchor fixation gave excellent results regardless of the chronicity of the repair. One patient died of a myocardial infarction within a year of surgery.
- The authors suggest anabolic steroid use may contribute to the injury through an excessive upward adjustment of the athlete's lifting goals rather than a demonstrated change in tendon properties, and that the rupture is probably not related to limb dominance. With six patients this is a case series, so it establishes what can happen rather than how often, and cannot support a rupture risk estimate.
The common performance/appearance-enhancing substances (anabolic-androgenic steroids, stimulants, diuretics, growth hormone, supplements), the fact that their signs can mimic other conditions, and that doping can cause severe and sometimes permanent organ damage (liver, kidney, heart) with recognition, treatment and education/prevention being important, come from the cited Siegmund review. The specific adverse- effect profile of anabolic-androgenic steroids (cardiovascular/hepatic/endocrine/psychiatric, adolescent physeal closure), the key orthopaedic association with TENDON RUPTURE (pectoralis major, Achilles, quadriceps), the cardiovascular/heat risks of stimulants, and the anti-doping (WADA) framework are standard, well-established teaching. The surgical outcomes, the finding that continued steroid use did not compromise repair, the death from myocardial infarction and the proposed behavioural mechanism come from the Stefanou series of six patients, which is too small to give any rate. The Siegmund citation is a nursing review rather than a study. No cohort quantifies the tendon-rupture risk attributable to anabolic steroids, no controlled study demonstrates altered human tendon material properties from them, and no evidence establishes whether stopping steroids before or after tendon repair changes the outcome - so none of those figures is quoted here.