Housemaid's Knee
- Prepatellar bursitis ('housemaid's knee') is inflammation of the superficial prepatellar bursa, which lies in FRONT of the patella, producing a localised, well-circumscribed, fluctuant SUPERFICIAL swelling over the kneecap; because the bursa is superficial and extra-articular, the knee joint itself is normal and the swelling must be distinguished from a true intra-articular EFFUSION (which is deep, fills the suprapatellar pouch and balloons around the joint line).
- The COMMONEST cause is CHRONIC microtrauma from repetitive KNEELING (the occupational 'housemaid's/carpet-layer's/roofer's knee'); other causes are acute trauma or haemorrhage, inflammatory and crystal arthropathies (gout, rheumatoid arthritis), and INFECTION (septic bursitis), with the olecranon and prepatellar bursae being the commonest sites of superficial bursitis.
- The single most important clinical task is to distinguish SEPTIC from NON-SEPTIC bursitis, because the superficial location makes the prepatellar bursa prone to infection (often from a breach in the overlying skin); features suggesting sepsis include marked warmth, tenderness, erythema, fever and cellulitis, and ULTRASOUND can help distinguish a bursitis from surrounding cellulitis while blood tests/MRI help separate infectious from non-infectious causes.
- If infection is suspected, ASPIRATE the bursa and examine the fluid with Gram stain, culture, cell count, glucose and crystal analysis; STAPHYLOCOCCUS AUREUS is the predominant organism in septic bursitis (with streptococci next), so empirical antibiotics should cover S. aureus, given orally in the well patient and intravenously in those who are febrile/acutely ill or have extensive cellulitis.
- CONVERSELY, a non-infected chronic MICROTRAUMATIC bursa should generally NOT be aspirated, because aspiration carries a risk of introducing infection (iatrogenic septic bursitis); microtraumatic and acute traumatic bursitis are treated conservatively (rest, ice, compression, activity modification/kneeling avoidance, analgesia), and intrabursal corticosteroid injection has weak evidence and is not routinely recommended for microtraumatic cases.
- MANAGEMENT therefore depends on the TYPE: acute traumatic/haemorrhagic - conservative (aspiration may shorten symptoms in selected cases); chronic microtraumatic - conservative and address the cause (knee protection); inflammatory/crystal - treat the underlying condition (steroid injection often used); and SEPTIC - anti-staphylococcal antibiotics (a course of adequate duration; a course shorter than about two weeks is associated with more failures), with surgical drainage/bursectomy reserved for bursitis not responding to antibiotics or for recurrent disease.
- “Prepatellar bursitis = superficial swelling IN FRONT of the patella ('housemaid's knee') - distinguish from an intra-articular effusion (deep). Commonest cause = chronic KNEELING microtrauma.
- “KEY task: septic vs non-septic. Aspirate if infection suspected (Gram/culture/crystals); S. aureus predominates. Ultrasound separates bursitis from cellulitis.
- “Do NOT routinely aspirate a non-infected microtraumatic bursa (iatrogenic infection). Septic -> anti-staph antibiotics (adequate duration); surgery for non-response/recurrence.
A localised, fluctuant superficial swelling in front of the patella ('housemaid's knee') - the knee joint is normal (not an intra-articular effusion). Commonest cause: chronic kneeling.
Septic or not? Aspirate if infection suspected (S. aureus); ultrasound separates bursitis from cellulitis. Don't routinely aspirate a non-infected microtraumatic bursa.
The Anatomy and the Anterior-Knee-Swelling Differential
- The anatomy: the prepatellar bursa lies superficial to the patella, between the skin and the patella / patellar tendon (a subcutaneous bursa, with subfascial/subtendinous extensions described). Because it is superficial, extra-articular and does not communicate with the joint, the knee joint is normal - unlike a true intra-articular effusion (deep, fills the suprapatellar pouch, ballottable patella, fluctuant around the joint line).
- The differential of anterior knee swelling:
- Infrapatellar bursitis ("clergyman's knee"): swelling over the tibial tubercle / patellar tendon from more upright kneeling, versus the prepatellar "housemaid's knee" from kneeling flat over the patella.
- Pes anserine bursitis (medial, below the joint line) and other periarticular bursae - see Pes Anserine Bursitis.
- A true intra-articular effusion.
- Gouty tophus (see Gout and Crystal Arthropathy), a ganglion/cyst, a Morel-Lavallée lesion (see Morel-Lavallée Lesion), and rarely a soft-tissue tumour.
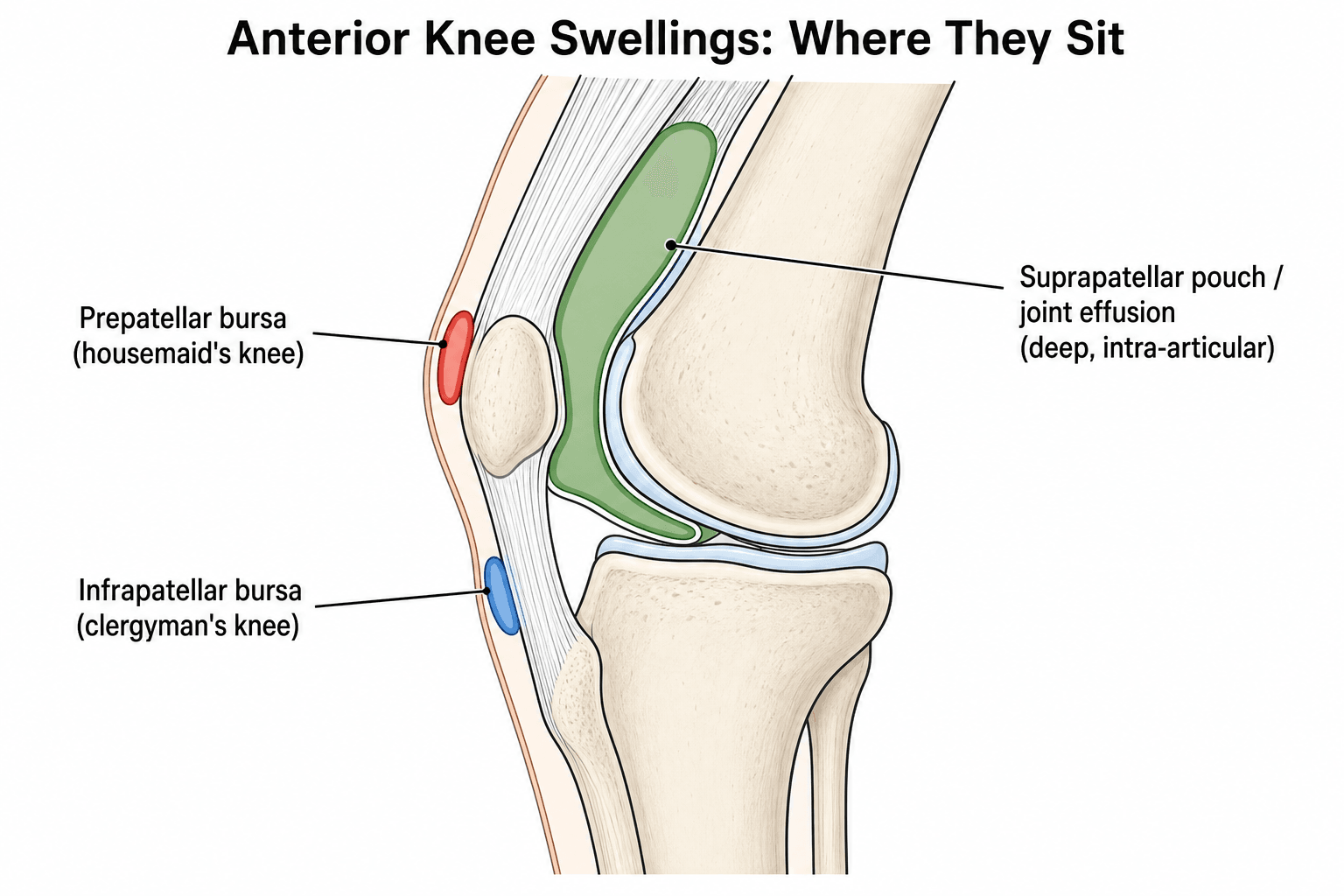
The prepatellar bursa is subcutaneous, in front of the patella, not communicating with the joint - so the knee is normal (vs a deep, ballottable effusion). Anterior-knee-swelling differential: prepatellar ("housemaid's knee", flat kneeling) vs infrapatellar ("clergyman's knee", upright kneeling), pes anserine bursitis, effusion, gouty tophus, ganglion, Morel-Lavallée.
Reading the Aspirate: Septic vs Non-Septic in a Bursa
- No septic-arthritis WBC cut-off: bursal fluid has no single agreed white-cell threshold, and an infected bursa often has a much lower count than an infected joint - the joint's ~50,000 figure does not apply, so a "low" count does not exclude infection; a high count with neutrophil predominance supports it.
- Gram stain is insensitive: it is positive in only about half of septic bursitis, so a negative Gram stain does not exclude infection - culture is the gold standard (and the diagnosis may rest on the clinical picture and antibiotic response when cultures are negative).
- Low glucose in the bursal fluid (relative to serum) supports infection.
- Crystals do not exclude sepsis: gout/CPPD crystals can be present, but crystals and infection can coexist, so still send culture even when crystals are seen.
- Integrate with the clinical picture: treat as septic if the picture fits even with equivocal or culture-negative fluid (full septic-bursitis management is in Septic Bursitis).
Where you put the needle matters as much as whether you aspirate. Enter through healthy skin, away from the most inflamed area, and take an oblique rather than a perpendicular track. Two reasons: needling through cellulitic skin drives surface organisms into the bursa, and a puncture at the point of maximum tension over a subcutaneous bursa can fail to seal and become a chronic sinus. A discharging sinus over the patella is considerably harder to treat than the bursitis was, because the skin there is thin, poorly vascularised and loaded every time the patient kneels.
Anatomical reasoning tells you the prepatellar bursa is extra-articular, but the bedside test is dynamic and takes seconds: passive knee movement is preserved and relatively comfortable in bursitis, because the inflamed structure lies in front of the patella and is not stretched by moving the joint. In septic arthritis any movement is agonising, because a distended, inflamed capsule is loaded through range.
That distinction matters more than it first appears. A hot, swollen, erythematous knee in a febrile patient prompts a septic-joint pathway; if the pathology is actually a superficial bursa, the joint is normal and does not need an arthrotomy. Conversely, a knee that resists all movement is not a bursitis, whatever the anterior swelling looks like. (The joint's own pathway is in Septic Arthritis Pathophysiology.)
Interpret bursal fluid differently from a joint: there is no reliable WBC cut-off (the ~50,000 septic-joint figure does not apply, so a low count does not exclude infection), the Gram stain is positive in only ~half (culture is the gold standard), low glucose supports infection, and crystals do NOT exclude concurrent sepsis - always culture and treat on the clinical picture.
Recognition, Causes & the Septic Question
Prepatellar bursitis is inflammation of the superficial bursa in front of the patella - 'housemaid's knee'
- giving a localised, fluctuant superficial swelling over the kneecap with a normal underlying knee joint (distinguish it from a deep intra-articular effusion). The commonest cause is chronic kneeling microtrauma; others are acute trauma/haemorrhage, gout/rheumatoid disease, and infection. The crucial clinical task is to decide whether it is septic, because the superficial bursa is prone to infection from a skin breach: warmth, marked tenderness, erythema, fever and cellulitis suggest sepsis. Ultrasound helps distinguish bursitis from cellulitis, and if infection is suspected the bursa is aspirated (Gram stain, culture, cell count, glucose, crystals); Staphylococcus aureus predominates. A non-infected microtraumatic bursa should NOT routinely be aspirated, because of the risk of iatrogenic septic bursitis.

Management by Type
- Acute traumatic/haemorrhagic: conservative - rest, ice, compression, elevation, analgesia; aspiration may shorten symptoms in selected cases.
- Chronic microtraumatic (kneeling): conservative and address the cause (knee protection / avoid kneeling); generally do NOT aspirate (iatrogenic infection risk); intrabursal corticosteroid has weak evidence and is not routinely recommended.
- Inflammatory/crystal (gout, RA): treat the underlying condition; intrabursal corticosteroid is often used.
- Septic: anti-staphylococcal antibiotics for an adequate duration (a course shorter than about two weeks is associated with more failures); oral in the well patient, IV if febrile/acutely ill or extensive cellulitis; surgical drainage/bursectomy for bursitis not responding to antibiotics or for recurrent disease.
If you do operate, respect the skin over the patella. The anterior knee is the worst place on the body to make a healing problem: the skin is thin, its blood supply is modest, and it is the surface the patient kneels on. Three consequences:
- Do not place a longitudinal incision down the midline over the patella. Use a transverse or parapatellar approach so the scar is off the kneeling surface and away from the point of maximum tension.
- Expect slower healing than the operation seems to justify, and protect it - the commonest complications of bursectomy are wound breakdown and a persistent sinus, not recurrence of the bursitis.
- Excise the bursa completely rather than partially, since a retained bursal remnant is a route to recurrence, and counsel the patient to keep off the knee until the wound is sound.
Antibiotics alone resolve most septic bursitis with success equivalent to surgery, so the threshold for operating should be genuine failure, an abscess or a foreign body - not impatience.
The two errors to avoid in prepatellar bursitis are opposite. The first is missing SEPTIC bursitis: because the prepatellar bursa is superficial and easily seeded through a skin breach, a hot, very tender, erythematous bursa
- especially with fever or cellulitis - should be treated as septic until proven otherwise, with aspiration for Gram stain and culture and anti-staphylococcal antibiotics, since untreated septic bursitis can progress. The second is needlessly aspirating a QUIET, non-infected microtraumatic bursa, which risks introducing infection and converting a benign problem into an iatrogenic septic bursitis - so a chronic kneeling-related bursa is managed conservatively with knee protection rather than routine aspiration. Distinguishing the superficial bursitis from a true intra-articular effusion, and septic from non-septic, is what guides safe management.
Mnemonics & Memory Aids
KNEEL
Hook:KNEEL: Kneeling cause, Not intra-articular, Evaluate for sepsis, Examine skin/ultrasound, Leave quiet bursa alone (aspirate/treat if septic).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient who kneels at work has a swelling in front of the kneecap. How do you assess it?”
“How does your management differ for septic versus non-septic prepatellar bursitis?”
Recognition
- Superficial, fluctuant swelling in front of the patella ('housemaid's knee')
- Knee joint normal - distinguish from intra-articular effusion
- Commonest superficial bursitis site along with the olecranon
Causes
- Chronic kneeling microtrauma (commonest)
- Acute trauma/haemorrhage; gout/rheumatoid arthritis
- Infection (septic bursitis - usually S. aureus)
Septic vs non-septic
- Septic signs: warmth, marked tenderness, erythema, fever, cellulitis
- Ultrasound separates bursitis from cellulitis; aspirate if infection suspected (Gram/culture/crystals)
- Do NOT routinely aspirate a non-infected microtraumatic bursa (iatrogenic infection)
Management
- Traumatic/microtraumatic: conservative (rest/ice/compression; knee protection)
- Inflammatory/crystal: treat underlying condition (steroid injection often used)
- Septic: anti-staph antibiotics (adequate duration); surgery for non-response/recurrence
Evidence & Key Studies
Common superficial bursitis (olecranon and prepatellar): diagnosis and management
- Chronic microtrauma (e.g. kneeling on the prepatellar bursa) is the most common cause of superficial bursitis; other causes include acute trauma/haemorrhage, inflammatory disorders (gout, rheumatoid arthritis) and infection.
- Diagnosis is clinical with a focus on septic signs; ultrasound distinguishes bursitis from cellulitis, and if infection is suspected the bursa should be aspirated (Gram stain, crystals, glucose, cell count, culture).
- Bursal aspiration of a non-infected microtraumatic bursa is generally not recommended (iatrogenic septic-bursitis risk); septic bursitis is treated with antibiotics effective against Staphylococcus aureus, with surgery reserved for non-responsive or recurrent cases.
Clinical characteristics and management of olecranon and prepatellar septic bursitis
- In 272 patients with septic bursitis, a microorganism was identified in about two-thirds, with staphylococci in 73% and streptococci in 19%.
- Septic bursitis resolved in the majority even with exclusively medical (antibiotic) treatment, with an equivalent success rate to surgical management.
- A treatment duration shorter than 14 days was associated with more failures in both medically and surgically treated patients.
The predominance of chronic kneeling microtrauma as the cause, the diagnostic focus on septic signs (with ultrasound distinguishing bursitis from cellulitis), the aspiration approach, the caution against aspirating a non-infected microtraumatic bursa, and the anti-staphylococcal treatment of septic cases come from the cited Khodaee review; the microbiology (staphylococci predominant), the equivalent success of medical and surgical management, and the higher failure rate with antibiotic courses shorter than 14 days from the cited Charret study. The distinction of a superficial bursitis from a true intra-articular effusion is standard, well-established teaching. Aspirating through healthy skin away from the inflamed area to avoid a chronic sinus, and the preserved passive joint movement that separates a bursitis from septic arthritis, follow Septic Bursitis, which covers the olecranon bursa alongside this one, so the two pages give the same technique. (See also Septic Arthritis Pathophysiology, Pes Anserine Bursitis and Gout and Crystal Arthropathy.)