Four-Part Concept | Blood Supply Critical | PROFHER Shapes Treatment
NEER CLASSIFICATION
Critical Must-Knows
- Neer classification based on 4 parts: head, greater tuberosity, lesser tuberosity, shaft
- Displacement criteria: greater than 1cm translation or over 45° angulation
- Arcuate artery (from anterior circumflex) is main blood supply to head - at risk in displaced fractures
- PROFHER trial: No difference between operative and non-operative treatment at 2 years
- 85% are minimally displaced and treated non-operatively with good outcomes
Clinical Pearls
- "Greater tuberosity displacement greater than 5mm in active patients warrants surgery
- "Elderly 4-part fracture = reverse shoulder arthroplasty (RSA) is gold standard
- "Valgus-impacted 4-part fractures have better blood supply - may be fixable
- "Axillary nerve at risk - assess deltoid and lateral shoulder sensation
Clinical Imaging
Imaging Gallery





Critical Proximal Humerus Fracture Exam Points
Blood Supply
Arcuate artery is terminal branch of anterior circumflex humeral artery. Enters at bicipital groove, runs in spiral to head. Disrupted in displaced fractures = AVN risk.
Neer Criteria
greater than 1cm displacement or over 45° angulation defines a displaced part. Count displaced parts, not fracture lines. 85% are 1-part (non-displaced).
PROFHER Evidence
Landmark UK trial: No functional difference at 2 years between surgical and non-surgical treatment for displaced fractures. Changed practice significantly.
Nerve at Risk
Axillary nerve runs 5-7cm below acromion. Test deltoid contraction and regimental badge sensation. At risk with anterior dislocation and surgery.
Quick Decision Guide
| Patient Profile | Fracture Pattern | Key Consideration | Treatment |
|---|---|---|---|
| Any age | 1-part (non-displaced) | 85% of all proximal humerus fractures | Sling, early ROM at 2 weeks |
| Young, active | 2-part surgical neck | greater than 1cm displacement or over 45° angulation | ORIF with plate or nails |
| Active patient | 2-part GT displacement greater than 5mm | Affects rotator cuff function | ORIF with screws/suture |
| Young (less than 65), good bone | 3-part or valgus-impacted 4-part | Head viability more likely | ORIF if reducible |
| Elderly (greater than 70) | Displaced 3-part or 4-part | High AVN risk, poor bone quality | Reverse shoulder arthroplasty |
| Elderly, low demand | Any displaced pattern | PROFHER supports non-op | Consider non-operative |
HGLSNeer Four-Part Classification
| H | Head (articular segment) Main blood supply concern - AVN risk |
| G | Greater tuberosity Supraspinatus and infraspinatus attach here |
| L | Lesser tuberosity Subscapularis attachment |
| S | Shaft Pectoralis major attaches, displaces shaft medially |
| H | Head (articular segment) Main blood supply concern - AVN risk | L | Lesser tuberosity Subscapularis attachment |
| G | Greater tuberosity Supraspinatus and infraspinatus attach here | S | Shaft Pectoralis major attaches, displaces shaft medially |
Hook:HGLS: Head Gets Less blood Supply when parts are displaced - count the separated parts!
AAPAProximal Humerus Blood Supply
| A | Anterior circumflex humeral artery Gives rise to arcuate artery - main supply |
| A | Arcuate artery Terminal vessel, enters at bicipital groove |
| P | Posterior circumflex humeral artery Minor contribution, runs with axillary nerve |
| A | AVN if disrupted 15-35% in 4-part fractures, 3-14% in 3-part |
| A | Anterior circumflex humeral artery Gives rise to arcuate artery - main supply | P | Posterior circumflex humeral artery Minor contribution, runs with axillary nerve |
| A | Arcuate artery Terminal vessel, enters at bicipital groove | A | AVN if disrupted 15-35% in 4-part fractures, 3-14% in 3-part |
Hook:AAPA: Anterior gives Arcuate - Posterior helper - AVN if Absent!
DRAGSSurgical Indications
| D | Displacement greater than 1cm or 45 degrees Neer criteria for displaced part |
| R | Rotator cuff compromise GT displaced greater than 5mm affects function |
| A | Active young patient Higher functional demands |
| G | Good bone quality Needed for stable fixation |
| S | Shaft translation greater than 100% Unable to reduce closed |
| D | Displacement greater than 1cm or 45 degrees Neer criteria for displaced part | G | Good bone quality Needed for stable fixation |
| R | Rotator cuff compromise GT displaced greater than 5mm affects function | S | Shaft translation greater than 100% Unable to reduce closed |
| A | Active young patient Higher functional demands |
Hook:DRAGS: Displaced fractures DRAG young active patients to surgery if bone is good!
MANSComplications
| M | Malunion Most common - especially GT malunion causing impingement |
| A | AVN (Avascular necrosis) 15-35% in 4-part, depends on head vascularity |
| N | Nerve injury (axillary) 5-7cm below acromion, test before surgery |
| S | Stiffness Common post non-op and operative - early ROM key |
| M | Malunion Most common - especially GT malunion causing impingement | N | Nerve injury (axillary) 5-7cm below acromion, test before surgery |
| A | AVN (Avascular necrosis) 15-35% in 4-part, depends on head vascularity | S | Stiffness Common post non-op and operative - early ROM key |
Hook:MANS: Malunion and AVN are the main concerns, Nerve injury and Stiffness complete the picture!
Overview and Epidemiology
Clinical Significance
Proximal humerus fractures are the third most common fracture in the elderly (after hip and distal radius). The PROFHER trial has fundamentally changed treatment approach - the majority can be treated non-operatively with equivalent outcomes to surgery.
Demographics
- Bimodal distribution: young males (high-energy), elderly females (low-energy)
- Peak incidence: 60-90 years
- Female predominance increases with age
- Strongly associated with osteoporosis
Mechanism
- Low-energy fall onto outstretched hand (elderly) - 80%
- High-energy trauma (young) - MVA, sports
- Pathological fractures in metastatic disease
- Associated injuries: rotator cuff, brachial plexus
Anatomy and Blood Supply
Blood Supply is Exam Critical
The arcuate artery (ascending branch of anterior circumflex humeral artery) provides the main blood supply to the humeral head. It enters the bone at the intertubercular groove and runs superiorly. Disruption leads to AVN - risk increases with displacement and number of parts.
Key Vascular Anatomy
| Vessel | Origin | Course | Clinical Significance |
|---|---|---|---|
| Anterior circumflex humeral | Axillary artery | Wraps anterior to surgical neck | Gives arcuate artery - main supply |
| Arcuate artery | Anterolateral ascending branch | Enters bicipital groove, spirals to head | Terminal vessel - no collaterals |
| Posterior circumflex humeral | Axillary artery | Through quadrangular space with axillary nerve | Minor head supply, greater tuberosity supply |
| Axillary artery | Subclavian continuation | Behind pectoralis minor | At risk in fracture-dislocations |
Four Parts of Proximal Humerus
- Articular segment (Head): Blood supply concern
- Greater tuberosity: Supraspinatus, infraspinatus, teres minor attach
- Lesser tuberosity: Subscapularis attachment
- Shaft: Pectoralis major, deltoid, latissimus attach
Muscle Forces
- Supraspinatus: Pulls GT superiorly
- Pectoralis major: Pulls shaft medially
- Subscapularis: Internally rotates LT
- Deltoid: May displace shaft laterally
Exam Trap: Axillary Nerve
The axillary nerve exits the quadrangular space and wraps around the surgical neck 5-7cm below the acromion. Always document deltoid function and regimental badge sensation. Incidence of injury is 5-10% in fractures, higher with dislocations.
Classification Systems
Neer Classification (1970)
Based on 4 anatomical segments and displacement criteria.
| Parts | Description | Blood Supply | Treatment Tendency |
|---|---|---|---|
| 1-Part | No fragment meets displacement criteria | Intact | Non-operative |
| 2-Part | One fragment displaced (usually surgical neck or GT) | Usually preserved | ORIF if indicated |
| 3-Part | Two fragments displaced (head + one tuberosity attached) | At risk | ORIF or arthroplasty |
| 4-Part | All fragments separated (head isolated) | High AVN risk | Arthroplasty preferred |
Key Point
Count displaced parts, not fracture lines. A fracture can have multiple lines but if only one segment is displaced greater than 1cm or over 45°, it is a 2-part fracture. The head-split pattern and anatomic neck fractures have highest AVN risk.
Clinical Assessment
History
- Mechanism: FOOSH (low-energy), MVA (high-energy)
- Arm position: Held adducted, supported by other hand
- Pre-injury function: Activity level, dominant hand
- Comorbidities: Osteoporosis, diabetes, rotator cuff disease
Examination
- Look: Swelling, ecchymosis (tracks to chest/arm), deformity
- Feel: Crepitus, localized tenderness
- Move: Severely limited by pain
- Neurovascular: Axillary nerve, brachial plexus, pulses
Mandatory Neurovascular Exam
Axillary nerve assessment is mandatory: Test deltoid contraction (arm abduction against resistance) and sensation over regimental badge area (lateral arm). Document before and after any manipulation or surgery.
Neurovascular Testing
| Structure | How to Test | Positive Finding | Injury Rate |
|---|---|---|---|
| Axillary nerve | Deltoid contraction, regimental badge sensation | Weak abduction, numbness lateral arm | 5-10% in fractures, higher with dislocation |
| Brachial plexus | Motor and sensory exam all distributions | Variable deficits multiple nerves | Rare in isolated fractures |
| Axillary artery | Radial pulse, capillary refill, Doppler | Absent pulse, cool pale hand | Rare - fracture-dislocation risk |
| Musculocutaneous nerve | Elbow flexion (biceps), lateral forearm sensation | Weak flexion, numbness | Rare |
Associated Injuries
In high-energy trauma, assess for ipsilateral clavicle fracture (floating shoulder), scapula fracture, rib fractures, and pulmonary injury. In elderly low-energy falls, consider other fragility fractures and need for bone health assessment.
Differential Diagnosis of the Painful, Immobile Shoulder After a Fall
| Differential | Distinguishing Features | Key Investigation | Pitfall to Avoid |
|---|---|---|---|
| Proximal humeral fracture | Localised tenderness, crepitus, ecchymosis tracking to chest/arm | Trauma series radiographs (AP, scapular Y, axillary) | Missing a concomitant dislocation on inadequate views |
| Anterior glenohumeral dislocation | Squared-off shoulder, arm held abducted/externally rotated, empty glenoid | AP and axillary radiographs | Reducing before documenting axillary nerve function |
| Posterior dislocation / fracture-dislocation | Arm locked in internal rotation, light-bulb sign on AP, often after seizure or electrocution | Axillary or CT imaging (light-bulb sign easily missed) | Over-reliance on AP view alone - classically missed |
| Acromioclavicular joint injury | Tenderness and step at the ACJ, pain on cross-body adduction | AP/Zanca view of the ACJ | Attributing all shoulder pain to the humerus |
| Rotator cuff tear (acute) | Weakness in abduction/external rotation, normal bony architecture | Ultrasound or MRI | Labelling a missed greater-tuberosity fracture as a cuff tear |
| Pathological fracture | Minimal or no trauma, prior pain, lytic lesion on radiograph | Radiograph plus staging imaging if suspicious | Internal fixation without considering biopsy/staging |
Investigations
Imaging Protocol
Three views essential: True AP (Grashey), Scapular Y (Lateral), Axillary. These form the trauma series and allow assessment of all four parts and dislocation status.
Modified axillary view taken with patient leaning back over cassette - avoids need to abduct arm. Useful in acute trauma with limited mobility.
Recommended for all operative cases. 3D reconstructions help understand fracture pattern, articular involvement, head viability. Essential for 3-part and 4-part fractures.
Rarely indicated acutely. May help assess rotator cuff in subacute phase or evaluate blood supply to head (contrast enhancement).
Radiographic Views
| View | Technique | What It Shows | Key Assessment |
|---|---|---|---|
| True AP (Grashey) | 40° oblique to cassette | Glenohumeral joint space | Head location, displacement, dislocation |
| Scapular Y | 90° to Grashey | Lateral view of scapula | AP displacement, dislocation direction |
| Axillary | Beam through axilla | Glenoid and head relationship | Dislocation, GT/LT displacement |
| Velpeau | Patient leaning back | Modified axillary | When axillary not possible |
CT Scan Indications
Always get CT for: 3-part and 4-part fractures, head-split patterns, fracture-dislocations, pre-operative planning. CT with 3D reconstruction is superior for understanding complex patterns and identifying head viability in valgus-impacted fractures.

Management Algorithm
Non-Operative Management
Indications:
- 1-part (minimally displaced) fractures - 85% of all cases
- Elderly low-demand patients with displaced fractures (PROFHER evidence)
- Significant medical comorbidities precluding surgery
- Head-split or severely comminuted fractures in non-surgical candidates
Non-Operative Protocol
Collar and cuff or sling. Pendulum exercises begin immediately. Elbow, wrist, hand ROM.
Begin passive and active-assisted shoulder ROM. Supine exercises initially. X-ray at 2 weeks.
Progress to active ROM and strengthening. Most fractures clinically healed by 6-8 weeks.
Full strengthening program. Return to activities as tolerated. Some stiffness may persist.
PROFHER Impact
The PROFHER trial showed no difference in functional outcomes between surgical and non-surgical treatment for displaced proximal humerus fractures at 2 years. This has shifted practice toward more conservative management, especially in elderly patients.
Surgical Technique
ORIF with Locking Plate - Comprehensive Technique:
Consent Points
- Infection: 1-2% superficial, 0.5% deep
- Axillary nerve injury: 5-10% (document preop status)
- AVN: 3-14% (3-part), 15-35% (4-part)
- Screw penetration: 14% - may need removal
- Hardware failure/reoperation: 10-15%
- Stiffness: Very common - physio critical
Equipment Checklist
- Proximal humerus locking plate (system of choice)
- Locking and cortical screws - multiple lengths
- K-wires: 1.6mm and 2.0mm for temporary fixation
- Heavy sutures: No. 2 or 5 FiberWire/Ethibond
- Bone hook and elevator for reduction
- C-arm positioned from contralateral side
Patient Positioning:
Setup Checklist
30-45° trunk elevation. Head secured in padded headrest. Body shifted toward operative edge of table. Arm freely draped on arm board or mayo stand.
Avoid excessive lateral neck flexion - stretches plexus. Head in neutral rotation, supported centrally.
C-arm enters from contralateral side. Confirm AP, axillary, and Velpeau views achievable. Test imaging BEFORE draping.
Prep from nipple to neck, axilla to midline posteriorly. Free drape arm to allow full manipulation.
Positioning Pearl
Blood pressure can drop significantly in beach chair position (cerebral hypoperfusion). Keep MAP above 70mmHg, and avoid sudden position changes.
Arthroplasty Options
RSA is Now Preferred
Reverse shoulder arthroplasty (RSA) has largely replaced hemiarthroplasty for fractures. RSA provides reliable pain relief and function regardless of tuberosity healing, while hemiarthroplasty outcomes depend heavily on tuberosity healing.
Arthroplasty Comparison
| Option | Indications | Pros | Cons |
|---|---|---|---|
| Hemiarthroplasty | Young patient, good rotator cuff, good bone | Preserves native glenoid, revision possible | Outcomes depend on tuberosity healing, unpredictable |
| Reverse SA (RSA) | Elderly, rotator cuff deficient, 4-part fractures | Reliable outcomes, less dependent on tuberosities | Glenoid revision difficult, scapular notching |
| Total shoulder | Fracture with pre-existing OA (rare) | Address arthritis simultaneously | Complex surgery, rarely indicated acutely |
Tuberosity Reconstruction
In both hemiarthroplasty and RSA, tuberosity reconstruction is critical. Tuberosities should be fixed around the prosthesis using heavy non-absorbable sutures in a tension-band configuration. Tuberosity malunion or non-union is the most common cause of poor outcomes after shoulder arthroplasty for fracture.


Complications
Complications and Management
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| AVN | 15-35% (4-part) | Displacement, head vascularity | Close monitoring, arthroplasty if symptomatic |
| Malunion | Most common | Non-op treatment, inadequate reduction | Osteotomy if symptomatic, prevention key |
| Nonunion | 5-10% | Surgical neck fx, osteoporosis, smoking | Bone graft and fixation or arthroplasty |
| Stiffness | Common | Prolonged immobilization, adhesive capsulitis | Prevention with early ROM, may need MUA or release |
| Axillary nerve injury | 5-10% | Dislocation, surgical approach | Most recover - observe 3-6 months |
| Subacromial impingement | Variable | Plate or GT malposition | Hardware removal, tuberosity osteotomy |
| Screw penetration | Variable | Technical error | Remove offending screws |
AVN Risk Factors
AVN risk correlates with head ischemia: anatomic neck fractures (highest risk), head-split fractures, 4-part fractures (15-35%), 3-part fractures (3-14%). Valgus-impacted patterns have lower risk due to preserved medial soft tissue hinge.
Postoperative Care and Rehabilitation
ORIF Rehabilitation Protocol
Sling immobilization. Elbow, wrist, hand ROM. Pendulum exercises.
Begin passive and active-assisted ROM. Forward flexion in supine, ER to neutral.
Active ROM in all planes. X-ray confirmation of healing. Discontinue sling.
Progressive rotator cuff and deltoid strengthening. Return to activities 3-6 months.
Outcomes and Prognosis
Expected Outcomes by Treatment
| Treatment | Shoulder Function | Complications | Notes |
|---|---|---|---|
| Non-operative (1-part) | Good to excellent | Minimal | 85% of fractures, reliable outcomes |
| Non-operative (displaced) | Moderate | Stiffness, malunion | PROFHER supports in elderly |
| ORIF | Variable | Hardware issues, AVN | Best in young with good bone |
| Hemiarthroplasty | Unpredictable | Tuberosity dependent | Falling out of favor |
| RSA | Reliable | Scapular notching | Current gold standard for 4-part elderly |
Prognostic Factors
Key factors affecting outcome: Age (older = more stiffness), Initial displacement (correlates with soft tissue injury), Bone quality, Patient activity level, and Tuberosity healing (for arthroplasty). Function at 1-2 years is best predictor of long-term outcome.
Evidence Base
PROFHER Trial - Surgery vs Non-Surgery
- Pragmatic multicentre RCT of 250 adults (mean age 66 years) with displaced fractures involving the surgical neck. No significant difference in the Oxford Shoulder Score averaged over 2 years (39.07 surgical vs 38.32 non-surgical; difference 0.75 points, 95% CI -1.33 to 2.84; P=0.48). No difference in complications, secondary surgery, or mortality.
Cochrane Review - Interventions for Proximal Humeral Fractures
- 47 trials, 3179 participants. High-certainty evidence of no clinically important difference between surgery and non-surgery in shoulder function at 1 year (SMD 0.10, 95% CI -0.07 to 0.27) or 2 years, with a higher risk of additional surgery after operative treatment (RR 2.06). For RTSA versus hemiarthroplasty, only very low-certainty evidence of minimal between-group functional difference, but a lower complication and reoperation rate favouring RTSA.
Hertel Criteria - Predictors of Humeral Head Ischaemia
- Prospective intraoperative study of 100 intracapsular fractures. The best predictors of head ischaemia were a short calcar/metaphyseal head extension (less than 8mm), a disrupted medial hinge, and an anatomic-neck pattern. When all three were present the positive predictive value for ischaemia reached 97%.
Neer Classification Reliability
- 50 fractures reviewed by five observers on two occasions. Mean interobserver reliability coefficient (kappa) was 0.48-0.52 (moderate), and intraobserver reproducibility averaged 0.66. Simplifying the system did not improve agreement.
Locking Plate Complications
- Prospective multicentre observational study of 187 patients. Complications occurred in 52 of 155 patients (34%) at 1 year; the commonest was intraoperative screw perforation of the head (14%). 40% of complications were technique-related; 19% underwent unplanned second surgery.
Global Fracture Epidemiology in Older Adults
- Prospective database analysis 10 years apart confirming the proximal humerus as one of the classic fragility fractures whose incidence is rising in patients aged 65 years or over, with proximal humeral fractures among those increasing in older males. Driven by ageing populations and improved longevity.
Australian Registry Data (AOANJRR)
- Registry data on shoulder arthroplasty performed for acute fracture show lower cumulative revision rates for reverse total shoulder arthroplasty than for hemiarthroplasty across follow-up. Tuberosity-dependent hemiarthroplasty has progressively been replaced by RTSA for fracture indications.
Viva Scenarios
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Elderly Low-Energy Fall
"A 75-year-old woman presents after a fall at home. She has pain and inability to move her left shoulder. X-rays show a displaced 4-part proximal humerus fracture with the head in valgus position. She is otherwise healthy and independent with ADLs."
Scenario 2: Young Active Patient
"A 45-year-old competitive recreational tennis player falls during a match. He has a displaced 3-part fracture (greater tuberosity and surgical neck displaced) with moderate osteopenia. He is very keen to return to sport."
Scenario 3: Fracture-Dislocation
"A 60-year-old presents after high-speed MVA. On examination, the shoulder is squared-off with absent axillary nerve function. X-rays show a 3-part fracture-dislocation with the head posteriorly dislocated. CT confirms significant glenoid bone loss from a Hill-Sachs reverse lesion."
MCQ Practice Points
Blood Supply Question
Q: What is the main blood supply to the humeral head? A: The arcuate artery (ascending branch of the anterior circumflex humeral artery) provides 80% of blood supply. It enters at the intertubercular groove and is at risk in displaced fractures.
Classification Question
Q: In Neer classification, what defines a 'displaced part'? A: greater than 1cm translation or over 45° angulation. Count displaced parts (not fracture lines) - there are 4 anatomical parts: head, greater tuberosity, lesser tuberosity, and shaft.
AVN Risk Question
Q: What is the AVN rate in 4-part proximal humerus fractures? A: 15-35% for 4-part fractures, 3-14% for 3-part fractures. Valgus-impacted 4-part fractures have lower AVN risk due to preserved medial hinge.
PROFHER Trial Question
Q: What did the PROFHER trial demonstrate? A: No significant difference in functional outcomes (Oxford Shoulder Score) at 2 years between surgical and non-operative treatment for displaced proximal humerus fractures. Cost-effectiveness favored non-operative treatment.
Nerve at Risk Question
Q: Which nerve is most commonly injured in proximal humerus fractures? A: Axillary nerve (5-10% incidence). It wraps around the surgical neck 5-7cm below the acromion. Test deltoid contraction and regimental badge sensation.
Arthroplasty Question
Q: For a 75-year-old with a displaced 4-part fracture, what is the preferred arthroplasty option? A: Reverse shoulder arthroplasty (RSA). RSA provides more reliable outcomes than hemiarthroplasty because function is less dependent on tuberosity healing.
Guidelines, Registries & Global Practice
Global Epidemiology
Proximal humeral fractures account for roughly 4-5% of all fractures and are the third most common fragility fracture in older adults after the proximal femur and distal radius. According to PubMed-indexed epidemiology (Court-Brown et al., Injury 2018), their incidence is rising across high-income populations as longevity increases, with a marked female predominance from low-energy falls and a smaller cohort of younger patients sustaining high-energy injuries.
Side-by-Side Guidance and Evidence
International Guidance on Displaced Proximal Humeral Fractures
| Body / Source | Region | Core Recommendation | Evidence Base |
|---|---|---|---|
| PROFHER RCT / Cochrane review | UK / international | No functional benefit of surgery over non-operative care for most displaced surgical-neck fractures | Level I (RCT and high-certainty systematic review) |
| AAOS appropriate-use criteria | USA | Non-operative care reasonable for many displaced patterns; reserve arthroplasty for selected elderly 3/4-part fractures | Consensus informed by RCT evidence |
| NICE / BOA (BOAST) standards | UK | Multidisciplinary fragility-fracture pathway, shared decision-making, default to non-operative for older low-demand patients | Guideline / quality standard |
| AO Foundation principles | International | Restore medial column and head viability for fixation; RTSA where head not reconstructable | Expert principles plus cohort data |
| EFORT / European practice | Europe | Individualised: physiological age, bone quality and pattern over chronological age; rising RTSA use for fracture | Registry and cohort evidence |
Registry Evidence and Practice Variation
Joint Registries
- AOANJRR (Australia), NJR (UK), AJRR (USA): all record rising RTSA use for fracture
- RTSA shows lower cumulative revision than hemiarthroplasty for fracture indications
- Registries capture real-world implant survival beyond trial populations
Practice Variation
- Surgery rates vary widely between health systems despite Level I evidence favouring non-operative care
- High-income settings: locking plate or RTSA; resource-limited settings rely on closed treatment or external fixation
- PROFHER-2 (ongoing, RTSA vs HA vs non-surgery) will further refine choice in 3/4-part fractures
Bone Health and Medications
Secondary Fracture Prevention
- Low-energy fracture over age 50 triggers bone-health assessment (DEXA, vitamin D)
- Anti-resorptives (bisphosphonates, denosumab) and anabolic agents per local formularies
- In Australia these agents are PBS-listed; calcium and vitamin D supplementation as indicated
Orthogeriatric Care
- Fracture liaison services reduce re-fracture risk globally
- Falls assessment and frailty optimisation alongside fracture care
- Smoking cessation support (e.g. Quitline 13 7848 in Australia) aids bone healing
Fragility Fracture Assessment
Any proximal humerus fracture from a low-energy mechanism in a patient over 50 should trigger bone health assessment - DEXA, vitamin D, and consideration of anti-resorptive therapy through a fracture liaison service. This is a consistent recommendation across international guidelines for secondary fracture prevention.
PROXIMAL HUMERUS FRACTURES
Clinical summary
Key Anatomy
- •4 parts: Head, Greater tuberosity, Lesser tuberosity, Shaft
- •Arcuate artery (from anterior circumflex) = main blood supply
- •Axillary nerve 5-7cm below acromion - test deltoid and sensation
- •Pectoralis major displaces shaft medially
Neer Classification
- •Count DISPLACED parts (greater than 1cm or over 45°)
- •1-part = non-displaced = 85% of fractures = non-op
- •2-part = one displaced segment = consider ORIF if young/active
- •3-part = two displaced = ORIF vs arthroplasty
- •4-part = all separated = RSA in elderly
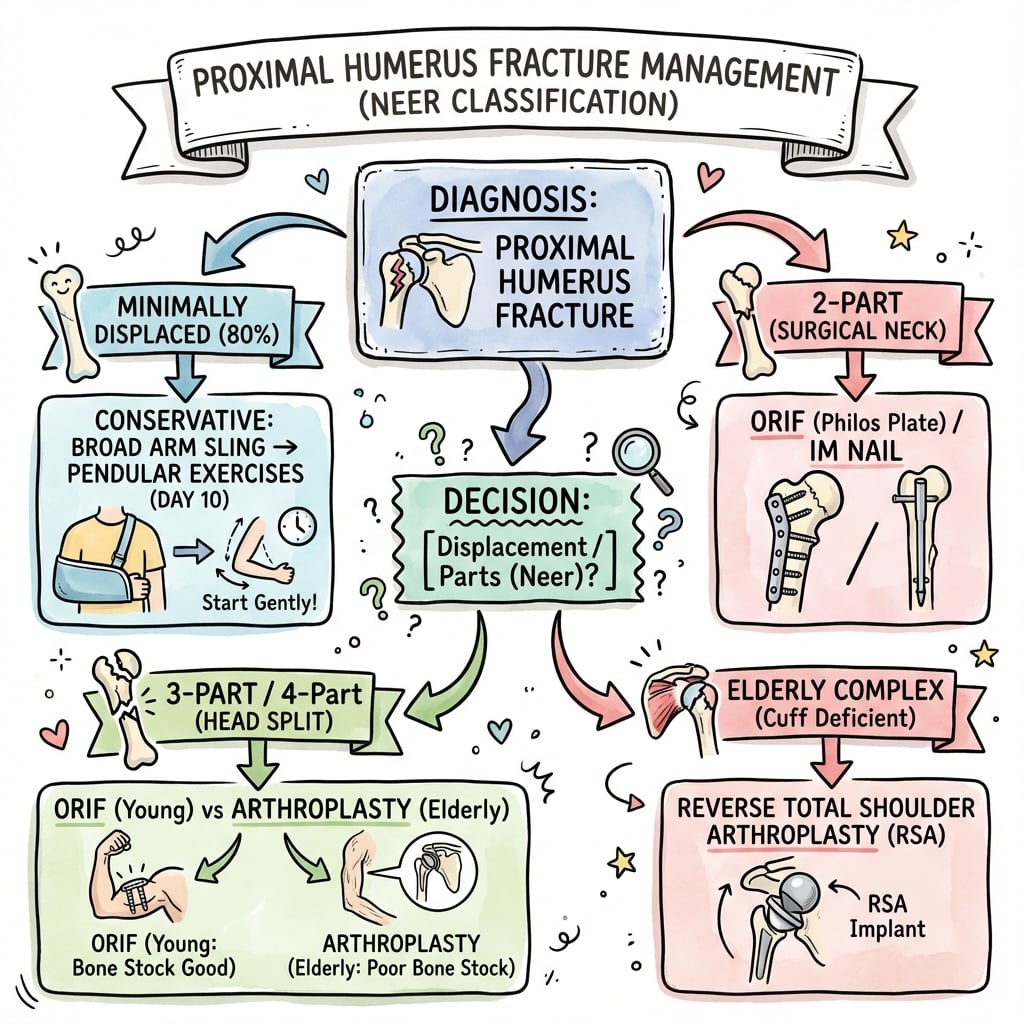
Treatment Algorithm
- •1-part: Sling and early ROM - excellent outcomes
- •2-part GT greater than 5mm: ORIF in active patients
- •2-part surgical neck: ORIF if young, consider non-op if elderly
- •3-part: ORIF if good bone and young, RSA if elderly
- •4-part: RSA preferred over hemiarthroplasty in elderly
Surgical Pearls
- •Deltopectoral approach - cephalic vein laterally
- •Plate 5-8mm below GT tip to avoid impingement
- •Calcar screw improves stability
- •Check screw penetration with fluoroscopy AP, axillary, Velpeau views
- •Tuberosity repair with heavy sutures critical for function
Complications
- •AVN: 15-35% in 4-part, 3-14% in 3-part
- •Malunion: Most common complication overall
- •Stiffness: Early ROM prevents adhesive capsulitis
- •Axillary nerve injury: Document before surgery, most recover