Direct Impact Injury | Flexion Key Prognostic Factor | Myositis Ossificans Prevention Critical
RYAN CLASSIFICATION (by ROM at 24h)
Critical Must-Knows
- Knee flexion at 24 hours is the key prognostic indicator
- Immediate 120 degree flexion position reduces hematoma and speeds recovery
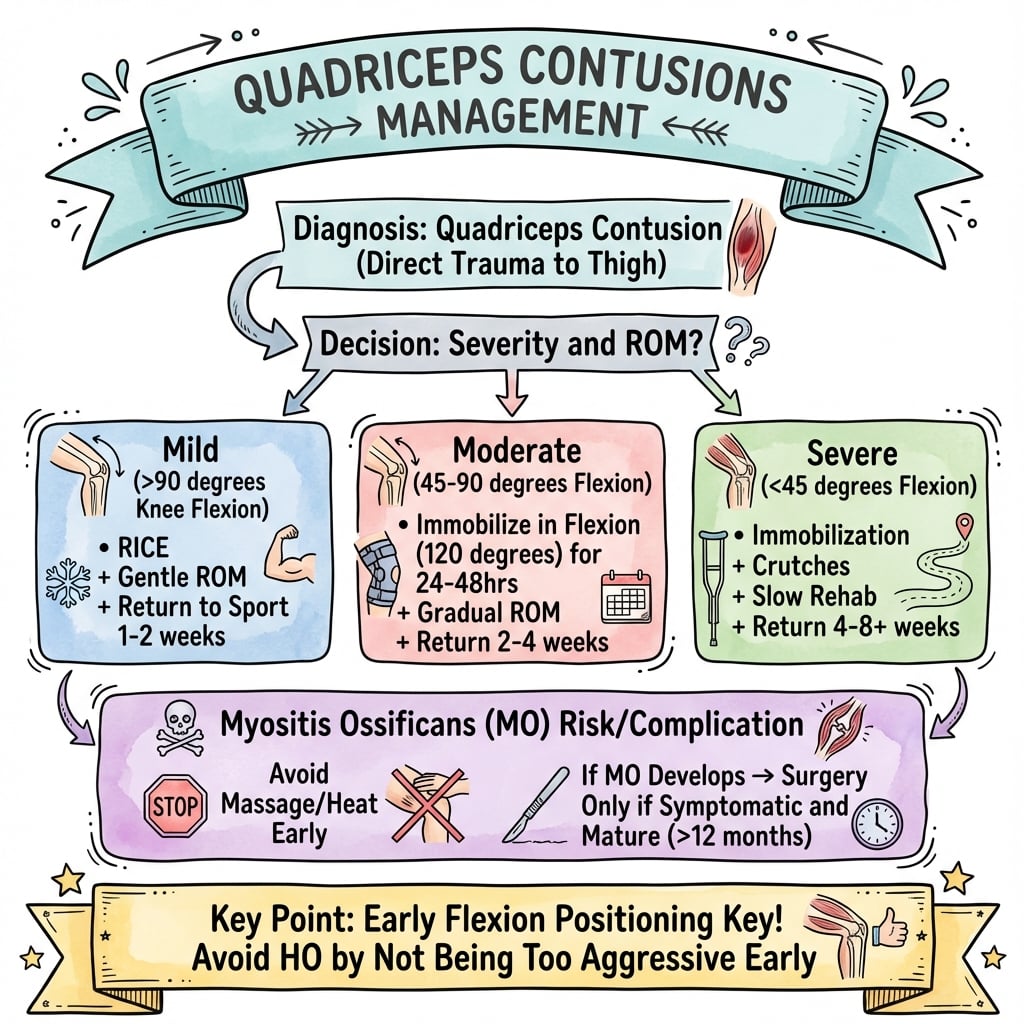
- Myositis ossificans develops in 9-17%, more common with severe grades
- Avoid early aggressive ROM and massage - increases MO risk
- NSAIDs and aspiration have role in preventing myositis ossificans
Clinical Pearls
- "Jackson and Feagin showed military cadets in flexion splints recovered 3x faster
- "Never massage a quadriceps contusion - promotes MO development
- "Heterotopic ossification appears on X-ray at 3-4 weeks post-injury
- "Compartment syndrome rare but possible - monitor tight thighs
Clinical Imaging
Imaging Gallery




Critical Quadriceps Contusion Exam Points
24-Hour ROM Classification
Flexion at 24 hours determines grade: greater than 90 degrees = mild, 45-90 degrees = moderate, less than 45 degrees = severe. This predicts recovery time and MO risk.
Flexion Position Treatment
Immediate 120 degree flexion (Jackson-Feagin protocol) shown to reduce recovery time from 88 to 13 days in military study. Compress hematoma between muscle bellies.
Myositis Ossificans Prevention
Avoid heat, massage, aggressive stretching in first 2-3 weeks. Consider indomethacin prophylaxis in severe grades. Aspiration of large hematomas may help.
Compartment Syndrome Risk
Anterior thigh compartment syndrome rare but described. High index of suspicion with severe contusions, anticoagulated patients, or coagulopathy.
Quick Decision Guide by Grade
| Grade | ROM at 24h | Expected Recovery | Key Management |
|---|---|---|---|
| Mild | Greater than 90 degrees flexion | 2-3 weeks | RICE, active ROM, progress when pain-free |
| Moderate | 45-90 degrees flexion | 3-6 weeks | Flexion splinting, protected rehab, monitor MO |
| Severe | Less than 45 degrees flexion | Greater than 6 weeks | Flexion splinting, consider NSAIDs prophylaxis, MRI |
| Myositis ossificans | Persistent pain, palpable mass | 3-6 months natural history | Wait for maturation, excise if symptomatic |
FLEX - AFLEX - Acute Management
| F | Flexion position 120 degrees knee flexion immediately |
| L | Limit activity Crutches, protected weight bearing |
| E | Early ice 20 min every 2 hours for 48-72h |
| X | X-ray if severe Rule out fracture, baseline for MO |
| F | Flexion position 120 degrees knee flexion immediately | E | Early ice 20 min every 2 hours for 48-72h |
| L | Limit activity Crutches, protected weight bearing | X | X-ray if severe Rule out fracture, baseline for MO |
Hook:Keep it FLEXED to compress the hematoma between muscle bellies
48 HRICE Plus - First 48 Hours
| R | Rest Non-weight bearing initially |
| I | Ice 20 min on, 20 min off |
| C | Compression Elastic wrap in flexed position |
| E | Elevation Above heart level |
| + | Plus NSAIDs Indomethacin for MO prophylaxis if severe |
| R | Rest Non-weight bearing initially | E | Elevation Above heart level |
| I | Ice 20 min on, 20 min off | + | Plus NSAIDs Indomethacin for MO prophylaxis if severe |
| C | Compression Elastic wrap in flexed position |
Hook:RICE is not enough for severe contusions - add NSAIDs for protection
MO RISK - MMO RISK - Myositis Ossificans Risk Factors
| M | Massage Never massage acute contusion |
| O | Over-aggressive rehab Passive stretching too early |
| R | Recurrent injury Return to sport too soon |
| I | Inadequate rest Insufficient immobilization |
| S | Severe grade Less than 45 degrees ROM at 24h |
| K | Keep playing Continuing activity after injury |
| M | Massage Never massage acute contusion | R | Recurrent injury Return to sport too soon | S | Severe grade Less than 45 degrees ROM at 24h |
| O | Over-aggressive rehab Passive stretching too early | I | Inadequate rest Insufficient immobilization | K | Keep playing Continuing activity after injury |
Hook:These factors put you at MO RISK for heterotopic bone formation
RTS CRTS Criteria - Return to Sport
| R | Range equal to uninjured Full symmetric ROM |
| T | Thigh girth equal Less than 1cm difference |
| S | Strength 90 percent plus Isokinetic testing symmetry |
| R | Range equal to uninjured Full symmetric ROM |
| T | Thigh girth equal Less than 1cm difference |
| S | Strength 90 percent plus Isokinetic testing symmetry |
Hook:RTS when ROM, Thigh circumference, and Strength are symmetric
Overview and Epidemiology
Quadriceps contusions are the second most common injury in contact sports after muscle strains. They result from direct blunt trauma to the anterior thigh, causing intramuscular hemorrhage and tissue damage.
Mechanism of injury:
- Direct blow - knee or helmet strike to anterior thigh (most common)
- Contact sports - rugby, Australian football, martial arts, football
- Falls - direct impact onto hard surface
- Motor vehicle accidents - dashboard injury
Sports distribution:
- Rugby and Australian Rules Football - highest incidence
- American football - common in receivers/running backs
- Hockey - puck or stick trauma
- Combat sports - knee strikes
Anatomical Vulnerability
The vastus intermedius is most commonly injured as it lies directly on the femur with no muscle posterior to provide cushioning. The rectus femoris is protected by the intermedius layer.
Pathophysiology and Mechanisms
Quadriceps muscle group:
- Rectus femoris - only biarticular muscle, hip flexor
- Vastus lateralis - largest, lateral aspect
- Vastus medialis - medial aspect, VMO critical for patella tracking
- Vastus intermedius - deepest, directly on femur
Blood supply:
- Branches of profunda femoris (lateral and medial circumflex femoral)
- Rich vascular supply explains significant hematoma formation
- Intramuscular bleeding contained by fascia
Pathophysiology of contusion:
Contusion Evolution
Acute hemorrhage into muscle belly. Vasospasm initially limits bleeding. Hematoma begins forming in the intramuscular space.
Inflammatory response peaks. Edema develops. ROM rapidly decreases. Critical window for classification by flexion.
Hematoma organization begins. Fibroblast migration starts. Continued inflammation. Key period for flexion positioning.
Granulation tissue formation. Early scar tissue. Risk period for myositis ossificans if tissue is reinjured or aggressively mobilized.
Muscle regeneration phase. Satellite cell activation. Progressive strengthening safe to begin if pain-free.
Myositis Ossificans Development
Heterotopic bone forms when pluripotent mesenchymal cells differentiate into osteoblasts instead of myoblasts. Risk factors include re-injury, massage, aggressive passive stretching, and large hematoma size.
Why Flexion Works
120 degree flexion compresses the hematoma between the rectus femoris and vastus intermedius, limiting expansion. It also maintains muscle length, preventing adaptive shortening. Jackson and Feagin demonstrated recovery in 13 days vs 88 days with extension splinting.
Classification Systems
Ryan Classification (by ROM at 24 hours - most commonly used)
| Grade | Knee Flexion at 24h | Gait | Swelling | Recovery Time |
|---|---|---|---|---|
| Mild | Greater than 90 degrees | Normal | Minimal | 2-3 weeks |
| Moderate | 45-90 degrees | Antalgic | Moderate | 3-6 weeks |
| Severe | Less than 45 degrees | Unable to walk | Severe | Greater than 6 weeks |
Clinical Application
The Ryan classification is the most practical as it uses a single objective measure (ROM) taken at a standardized time point (24 hours) to predict prognosis and guide treatment intensity.
This classification informs treatment intensity and helps you counsel athletes and coaches appropriately.
Differential Diagnosis of Anterior Thigh Pain After Trauma
| Diagnosis | Distinguishing Features | Key Investigation |
|---|---|---|
| Quadriceps contusion | Direct blunt blow, diffuse intramuscular swelling, ROM loss tracks severity | Clinical grading by 24h flexion; ultrasound for haematoma |
| Quadriceps strain (muscle tear) | Indirect eccentric overload (sprinting), pain at musculotendinous junction, no impact history | Ultrasound/MRI showing fibre disruption at junction |
| Myositis ossificans traumatica | Persistent firm mass and ROM plateau weeks after contusion | Radiograph at 3-4 weeks (peripheral zoning); CT if uncertain |
| Anterior thigh compartment syndrome | Pain out of proportion, tense compartment, pain on passive stretch, saphenous paraesthesia | Compartment pressure; urgent fasciotomy |
| Femoral shaft fracture | High-energy mechanism, deformity, inability to bear weight | Plain radiograph |
| Soft-tissue sarcoma (mimic) | Painless enlarging mass, no clear trauma, deep to fascia, more than 5 cm | MRI then biopsy of periphery; do NOT assume myositis ossificans |
Clinical Assessment
History
Key history points:
- Mechanism - direct blow, contact event, speed of impact
- Immediate response - able to continue playing? (poor prognostic sign if yes - suggests ongoing bleeding)
- Time since injury - critical for classification at 24 hours
- Previous quad contusions - risk factor for recurrence
- Anticoagulation status - increased bleeding risk
Red flag symptoms:
- Severe pain out of proportion
- Numbness in leg
- Progressive swelling despite rest
- Inability to weight bear at all
Documenting the history carefully guides prognosis and identifies high-risk patients.
Examination
Physical examination:
Inspection:
- Swelling location and extent
- Ecchymosis (may appear 24-48h later)
- Muscle contour - bulge or defect
Palpation:
- Point of maximal tenderness
- Palpable hematoma or mass
- Warmth
ROM testing (critical):
- Active and passive knee flexion
- Document angle at 24 hours for classification
- Compare to uninjured side
Strength testing:
- Resisted knee extension
- Straight leg raise ability
- Document any quad lag
Compartment Syndrome Signs
Pain with passive stretch, tense anterior compartment, paresthesias in saphenous nerve distribution, weak knee extension. Rare but requires urgent fasciotomy.
Investigations
X-ray:
- Not routinely required for typical contusion
- Indicated if fracture suspected (significant trauma)
- Baseline for monitoring myositis ossificans
- MO visible at 3-4 weeks post-injury
Ultrasound:
- First-line imaging for soft tissue assessment
- Quantifies hematoma size
- Differentiates intramuscular vs intermuscular
- Can guide aspiration
- Dynamic assessment of muscle integrity
MRI:
- Reserved for severe grades or diagnostic uncertainty
- Quantifies extent of muscle damage
- Identifies associated injuries
- Useful for return-to-play decisions in elite athletes
Ultrasound Findings
Acute hematoma appears hypoechoic or anechoic. Organized hematoma becomes more heterogeneous. Early myositis ossificans shows increased echogenicity before calcification is visible on X-ray.
Management Algorithm
Immediate management:
- Remove from play - do not continue with injury
- RICE protocol immediately
- 120 degree flexion position - wrap knee flexed
- Crutches - non-weight bearing to partial
- Ice - 20 min every 2 hours
Jackson-Feagin Protocol:
- Knee wrapped in maximal comfortable flexion
- Elastic bandage over ice pack
- Maintained for 24 hours initially
- Shown to reduce recovery time significantly
Medications:
- Analgesia as needed (paracetamol preferred)
- NSAIDs controversial early - may increase bleeding
- After 48-72h, indomethacin for MO prophylaxis in severe grades
This acute phase management is critical for optimal outcomes.
Surgical Technique
Surgical excision of myositis ossificans:
Surgery is rarely required for quadriceps contusions. The primary surgical indication is symptomatic mature myositis ossificans that fails conservative management.
Indications for excision:
- Persistent pain limiting function after MO maturation
- Mechanical symptoms (limited ROM, catching)
- Large MO causing cosmetic concern
- Failed conservative management for 6+ months
Contraindications:
- Immature MO (less than 6 months, hot bone scan)
- Asymptomatic MO
- Active infection
Careful patient selection is essential for successful surgical outcomes.
Complications
Myositis Ossificans Traumatica (MOT)
Incidence: 9-17% of quadriceps contusions
Risk factors:
- Severe grade (ROM less than 45 degrees)
- Delay in treatment greater than 72 hours
- Early massage or aggressive stretching
- Re-injury before full healing
- Large intramuscular hematoma
- Previous MO
Clinical features:
- Persistent pain beyond expected recovery
- Palpable firm mass in muscle
- Plateau or decrease in ROM
- Pain with activity
Radiographic features:
- Appears 3-4 weeks post-injury
- Zoning phenomenon - mature bone peripherally
- Matures over 3-6 months
Management:
- Initially conservative - wait for maturation
- NSAIDs may limit progression if caught early
- Surgical excision only if symptomatic AND mature (6-12 months)
- Pre-op bone scan to confirm maturity
Surgical Timing
Never excise immature myositis ossificans - high recurrence rate. Wait minimum 6 months, confirm maturity with bone scan (cold lesion), then excise with margin. Consider radiation prophylaxis post-excision in recurrent cases.
Rehabilitation and Return to Sport
Rehabilitation Phases
RICE protocol, 120 degree flexion positioning, crutches, ice every 2 hours. Goal is to minimize hematoma size and inflammation. No stretching or strengthening activities.
Begin active ROM exercises, continue ice, pain-free weight bearing progression. Stationary bike when 90 degrees flexion achieved. Avoid massage, heat, passive stretching.
Progressive resistance exercises when ROM greater than 90 degrees pain-free. Isometrics progressing to isotonics. Pool running and swimming permitted.
Sport-specific drills, agility training, plyometrics when strength greater than 80 percent. Non-contact training initially, then progress to contact with padding.
Full ROM, strength greater than 90 percent, functional testing passed. Protective thigh padding for first 2-4 weeks of competition. Monitor for any symptoms.
Return to Sport Criteria (all must be met):
| Criterion | Requirement | Testing Method |
|---|---|---|
| ROM | Equal to uninjured side | Goniometry |
| Strength | Greater than 90 percent | Isokinetic or 1RM |
| Thigh girth | Less than 1cm difference | Tape measure |
| Pain | None with activity | Functional testing |
| Functional | Pass hop tests | Single leg hop for distance |
Elite Athlete Considerations
In professional athletes, MRI may be used to confirm complete muscle healing before return to sport. Some teams use isokinetic testing with peak torque and total work comparisons to uninjured side, requiring greater than 90 percent symmetry.
Outcomes and Prognosis
Prognosis by grade:
| Grade | Expected Recovery | Return to Sport | MO Risk |
|---|---|---|---|
| Mild | 2-3 weeks | Full recovery expected | Low (under 5%) |
| Moderate | 3-6 weeks | Full recovery expected | Moderate (10-15%) |
| Severe | 6+ weeks | May have prolonged course | High (15-20%) |
Factors affecting outcome:
- Time to treatment initiation (earlier is better)
- Compliance with flexion positioning protocol
- Avoidance of re-injury during recovery
- Strict adherence to RTS criteria
Long-term outcomes:
- Most athletes return to pre-injury level
- Recurrent contusion possible if RTS too early
- Myositis ossificans may require delayed surgical excision
- Chronic pain rare if properly managed
Prognosis Summary
Key prognostic indicator is ROM at 24 hours. Athletes who follow the Jackson-Feagin flexion protocol and meet all RTS criteria have excellent outcomes with low recurrence rates. Premature return is the main risk factor for complications.
Evidence Base
Jackson-Feagin Study (1973) - Landmark
- Severity of injury correlates directly with disability and complication rate
- Heat, massage and premature activity were associated with worse outcomes and myositis ossificans
- Established graded rehabilitation and the principle of early protected motion
Ryan et al - West Point Update (1991) - Landmark Classification
- 24-hour knee ROM is the key prognostic indicator and basis of the grading system
- Mean disability 13 days (mild), 19 days (moderate), 21 days (severe)
- Myositis ossificans in 9%; five risk factors - ROM less than 120 degrees, football mechanism, previous quadriceps injury, treatment delay greater than 3 days, ipsilateral knee effusion
Aronen et al - Immediate 120 degree Flexion Immobilisation (2006)
- Immediate 120 degree flexion held for 24 hours dramatically shortened disability (mean 3.5 days)
- Only 1 case of myositis ossificans on 3- and 6-month radiographs of the first 23 patients
- Earlier intervention from the moment of injury improved results compared with prior series
Diaz et al - Severe Quadriceps Contusions (2003)
- Severe contusions produce large intramuscular haematoma and markedly prolonged recovery
- Imaging (ultrasound/MRI) defines haematoma size and guides rehabilitation
- Highlights need for protected, graded return to avoid re-injury and myositis ossificans
Beiner & Jokl - Contusion Injury and Myositis Ossificans (2002)
- Healing is a balance between muscle regeneration and scar/heterotopic bone formation
- Myositis ossificans is a major debilitating complication of contusion injury
- Reviews risk factors and prevention strategies including avoidance of re-injury and aggressive early mobilisation
Larruskain et al - Contusion Epidemiology in Elite Football (2018)
- Contusions are among the most common injuries in elite football
- Contusion incidence 4.82 times higher in male than female players (95% CI 2.30-10.08)
- Reflects greater contact exposure as the driver of contusion injury
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Severe Contusion
"A 22-year-old rugby player presents 6 hours after a direct knee strike to his anterior thigh. He has marked swelling and can only flex his knee to 30 degrees. How would you manage this player?"
Scenario 2: Myositis Ossificans Development
"A footballer returns 4 weeks after a moderate quadriceps contusion with persistent pain and a firm palpable mass in the anterior thigh. X-ray shows early calcification. How would you manage this?"
Scenario 3: Return to Sport Decision
"A professional AFL player sustained a moderate quadriceps contusion 5 weeks ago. He has regained 100 degrees of knee flexion and wants to return for finals. The coach is putting pressure on medical staff. How do you approach this?"
MCQ Practice Points
Ryan Classification
Q: What is the key prognostic indicator for recovery time in quadriceps contusions? A: Knee flexion at 24 hours. Recoveries vary from 2-3 weeks (greater than 90 deg) to greater than 6 weeks (less than 45 deg).
Jackson-Feagin Protocol
Q: What is the most important acute intervention? A: Immediate 120 degree knee flexion positioning. This compresses the hematoma and prevents stiffness.
Myositis Ossificans Signs
Q: What radiographic sign distinguishes Myositis Ossificans from malignancy? A: Zoning Phenomenon. MO has mature cortical bone peripherally with a central lucency. Osteosarcoma is the reverse (central ossification, indistinct margin).
Contraindications
Q: What modalities should be absolutely avoided in the acute phase? A: Heat and Massage. Both increase blood flow and risk of Myositis Ossificans.
Return to Sport
Q: What is a mandatory criterion for return to contact sports? A: Full ROM and greater than 90% Strength. Plus protective padding is essential.
Guidelines, Registries & Global Practice
Global epidemiology:
| Measure | Figure | Source |
|---|---|---|
| Rank among sports injuries | Contusion second only to strain as cause of sports-injury morbidity | Beiner & Jokl (PMID 11476532) |
| Frequency in elite football | Among most common injury categories over five seasons | Larruskain et al (PMID 28207979) |
| Sex difference (contusion) | 4.82x higher incidence in men vs women (contact exposure) | Larruskain et al (PMID 28207979) |
| Myositis ossificans risk | 9% of quadriceps contusions (up to 9-17% in series) | Ryan et al (PMID 1867338) |
The injury is fundamentally a contact-sport problem and is over-represented wherever collision codes dominate (the football codes, rugby, American football, ice hockey, martial arts and combat sports). The driver is exposure to direct blunt impact rather than any geographic or health-system factor.
Guidance and consensus, side by side:
There is no high-level RCT-based guideline body that issues a quadriceps-contusion-specific protocol; practice is built on the West Point/Naval Academy military series and sports-medicine consensus, which are remarkably consistent worldwide.
| Body / source | Position | Evidence level |
|---|---|---|
| West Point / Naval Academy series (Ryan; Aronen) | Immediate sustained knee flexion (aim 120 degrees), grade by 24-hour ROM, avoid heat/massage | Level IV consensus from prospective military series |
| AMSSM / sports-medicine consensus (US) | RICE plus early protected flexion; criteria-based graded return | Expert consensus |
| BJSM / European sports-medicine practice | Same acute principles; emphasis on ultrasound/MRI grading and objective return-to-sport testing | Expert consensus |
| AO / general trauma principles | Exclude fracture and compartment syndrome; conservative care for isolated contusion | Expert consensus |
There is no joint or implant registry relevant to this soft-tissue injury, so registry-based survival or revision data do not apply.
Global practice variation:
| Setting | Typical approach | Reason |
|---|---|---|
| Elite / professional team setting | Immediate pitch-side flexion bracing, early ultrasound/MRI, isokinetic-guided return | Resourced medical teams, financial stakes of recurrence |
| Community / general practice | Clinical grading by ROM, RICE, physiotherapy-led rehabilitation, imaging only if severe or atypical | Cost-effective and adequate for most cases |
| Limited-resource settings | Clinical diagnosis and graded rehabilitation without routine imaging | Imaging access constrained; clinical course usually sufficient |
The Universal Principle
Across every region and resource setting the core message is identical: immediate sustained flexion, grade by 24-hour ROM, avoid heat and massage, and use objective criteria for return to sport. Premature return is the dominant modifiable risk factor for recurrence and myositis ossificans.
Quadriceps Contusions
Clinical summary
Classification (Ryan)
- •Mild: Flexion greater than 90 degrees at 24h - RTS 2-3 weeks
- •Moderate: Flexion 45-90 degrees - RTS 3-6 weeks
- •Severe: Flexion less than 45 degrees - RTS greater than 6 weeks
- •Prognosis: 24h ROM is key predictor
Acute Management
- •IMMEDIATE 120 degree flexion positioning
- •RICE protocol - ice 20 min every 2 hours
- •Non-weight bearing with crutches
- •NSAIDs AFTER 48-72h only (bleeding risk earlier)
Jackson-Feagin Protocol
- •Wrap knee in maximal comfortable flexion
- •Elastic bandage over ice pack
- •Reduced recovery 88 days to 13 days
- •Compresses hematoma between muscle bellies
Myositis Ossificans
- •Develops in 9-17% of quad contusions
- •Visible on X-ray at 3-4 weeks
- •ZONING phenomenon = mature bone peripherally
- •Surgery only after maturation (6-12 months)
Return to Sport Criteria
- •Full ROM equal to uninjured side
- •Strength greater than 90 percent (isokinetic)
- •Thigh girth within 1cm
- •Pain-free with sport-specific activity
Key Exam Points
- •Never massage acute quad contusion
- •Avoid heat and aggressive stretching early
- •MO vs Osteosarcoma: zoning phenomenon key differentiator
- •Compartment syndrome rare but possible - high suspicion