Suprapatellar pain | Deep flexion aggravation | Eccentric loading | Older athlete demographic
- Location: Tenderness at the superior pole of the patella (distal quadriceps insertion).
- Demographics: Often affects slightly older athletes compared to Jumper's Knee.
- Biomechanics: Deep flexion places maximum tensile load on the quadriceps tendon.
- Differential: Must rule out suprapatellar plica and bipartite patella.
- Treatment: Eccentric strengthening remains the cornerstone.
- “Tenderness is at the suprapatellar insertion (superior pole).
- “Pain is reproduced by resisted extension from deep flexion.
- “Often associated with a 'gap' palpable in ruptures (sulcus sign).
- “Calcification is more common than in patellar tendon.
Clinical Imaging
Imaging Atlas

Differentiation from Jumper's Knee is purely anatomical. Quadriceps tendinopathy is at the superior pole. Patellar tendinopathy is at the inferior pole. Do not confuse them.
Bilateral quadriceps tendon rupture is a classic association with systemic disease (Renal failure, Diabetes, RA, Hyperparathyroidism) or fluoroquinolone/steroid use. Always ask about medical history.
The quadriceps tendon is under maximal tension in deep flexion. Pain is often worse at the bottom of a squat, whereas patellar tendinopathy pain is often worse during the descent/deceleration phase.
Surgical debridement requires splitting the tendon. The quadriceps tendon is multi-layered (trilaminar). Understanding this anatomy is crucial for partial thickness tears.
| Condition | Location | Aggravating Factor | Management |
|---|---|---|---|
| Quadriceps Tendinopathy | Superior pole insertion | Deep squat / deceleration | Eccentric rehab |
| Suprapatellar Plica | Medial suprapatellar | Plausible snap/click | Injection / resection |
| Bipartite Patella | Superolateral pole | Direct trauma / overuse | Rest / excision |
| Quadriceps Rupture | Suprapatellar gap | Unable to extend knee | Surgical repair |
| Prepatellar Bursitis | Anterior to patella | Kneeling / direct pressure | Aspiration / protection |
REALRupture Risk Factors - REAL-MD
Hook:REAL-MDs check for systemic causes
RFQuadriceps Anatomy - RF-VL-VM-VI
Hook:Three layers of the tendon
IEMRehab Progression - IEM
Hook:I Eat Meat (muscle/tendon fuel)
Overview and Epidemiology
Quadriceps tendinopathy is a degenerative condition affecting the suprapatellar insertion of the quadriceps tendon. While less common than patellar tendinitis (Jumper's Knee), it is a significant cause of anterior knee pain, particularly in older athletes and weightlifters.
Epidemiology:
- Prevalence: Lower than patellar tendinitis (approx 1/10th frequency in some series).
- Age: Typically older cohort (greater than 35-40 years) compared to patellar tendinitis (under 30 years).
- Sports: Volleyball, basketball, weightlifting (deep squats).
- Gender: Male greater than Female.
The "Jumper's Knee" spectrum moves proximal with age. Young/Adolescents = Tibial Tubercle (Osgood-Schlatter). Young Adults = Patellar Tendon (Inf pole). Older Adults = Quadriceps Tendon (Sup pole).
Pathophysiology and Mechanisms
Anatomy:
- Insertion: Base of patella (superior pole).
- Layers (Trilaminar):
- Superficial: Rectus femoris
- Middle: Vastus lateralis and Vastus medialis (conjoined)
- Deep: Vastus intermedius
- Hypovascular Zone: 1-2cm proximal to the superior pole of the patella is the "watershed" area, most prone to rupture and degeneration.
Pathophysiology:
- Identical to patellar tendinopathy: Angiofibroblastic tendinosis.
- Microtearing formed by repetitive eccentric loading outpacing repair.
- Calcification: More common in quadriceps tendon than patellar tendon (Calcific tendinitis).
- Bone Spur: Traction enthesophyte at superior pole is common (tooth sign).
Classification Systems
Blazina Classification (Modified)
Originally described for Jumper's knee, applied to Quads tendon.
- Symptoms
- Pain only after activity
- Function
- No functional impairment
- Treatment
- Ice, NSAIDs, eccentric rehab
- Symptoms
- Pain during and after activity
- Function
- Can still compete/perform
- Treatment
- Activity mod + intense rehab
- Symptoms
- Pain during and after
- Function
- Unable to compete at level
- Treatment
- Prolonged rest, consider surgery
- Symptoms
- Complete tendon rupture
- Function
- Loss of extension
- Treatment
- Surgical repair
Blazina aids in decision making. Stage 1/2 is rehab. Stage 3 warrants imaging and discussion of intervention.
Simple, clinically relevant.
Clinical Presentation and Assessment
History:
- Suprapatellar pain.
- Pain with deep knee flexion (e.g., squatting past 90 degrees).
- "Start-up pain" (stiffness after sitting).
- History of jumping or heavy lifting.
Physical Examination:
| Manoeuvre | Finding | Significance |
|---|---|---|
| Palpation | Tenderness at superior pole of patella | Confirm anatomic location |
| Resisted Extension | Pain, especially from deep flexion | Loads quad tendon maximally |
| Gap Test | Palpable sulcus suprapatellar | Signs of rupture |
| Active Straight Leg Raise | Lag / Inability | Complete rupture mechanism failure |
| Suprapatellar Plica | Medial snapping / tenderness | Differential diagnosis |
Check the Extensor Mechanism:
- Always confirm the integrity of the mechanism. A "painful" tendon can also be a "partially ruptured" tendon.
- Lag: Any extensor lag with active straight leg raise is a red flag.
If a patient presents with bilateral symptoms, particularly if acute-on-chronic pain, screen for systemic risk factors (Renal, Diabetes, Gout).
Investigations
1. Radiographs (X-ray):
- Views: AP, Lateral, Skyline.
- Findings:
- Tooth Sign: Traction spur at superior patellar pole (enthesophyte).
- Calcification: Loose bodies or intratendinous calcification (calcific tendinitis).
- Patella Alta/Baja: Assessing height.
- Bipartite Patella: Usually superolateral (saupe type III).
2. Ultrasound (US):
- Excellent for tendon architecture.
- Findings: Thickening, hypoechogenicity, loss of fibrillar pattern.
- Dynamic: Can assess impairment with flexion/extension.
- Calcification: High sensitivity for calcium deposits.
3. MRI:
- Gold Standard for quantifying degeneration and ruling out intra-articular pathology.
- Sequence: T2/STIR hyperintensity in the distal quadriceps tendon.
- Partial Tears: Fluid signal intensity interrupting fibers.
| Modality | Pros | Cons |
|---|---|---|
| Ultrasound | Dynamic, cheap, good for guided injection | Operator dependent |
| MRI | Shows internal derangement, partial tears, edema | Cost, static |
| X-ray | Shows calcification and spurs | Soft tissue invisible |
Management
Cornerstone of Treatment: Management mirrors patellar tendinopathy but focuses on deep flexion control.
Protocol:
- Phase 1 (Analgesia): Isometric holds (e.g., wall sit at 60 deg). Ice. NSAIDs.
- Phase 2 (Isotonic): Heavy Slow Resistance (HSR). Leg press, squats.
- Phase 3 (Eccentric):
- Note: Standard eccentric decline squats may impinge the superior pole if deep flexion is forced too early.
- Controlled eccentric lowering (e.g., single leg press lowering).
- Phase 4 (Plyometric): Return to jumping.
In quadriceps tendinopathy, deep flexion (past 90 deg) compresses the tendon against the femur/trochlea. Early rehab should often limit flexion to 0-60 degrees to avoid compressive load, progressing to deep flexion late.
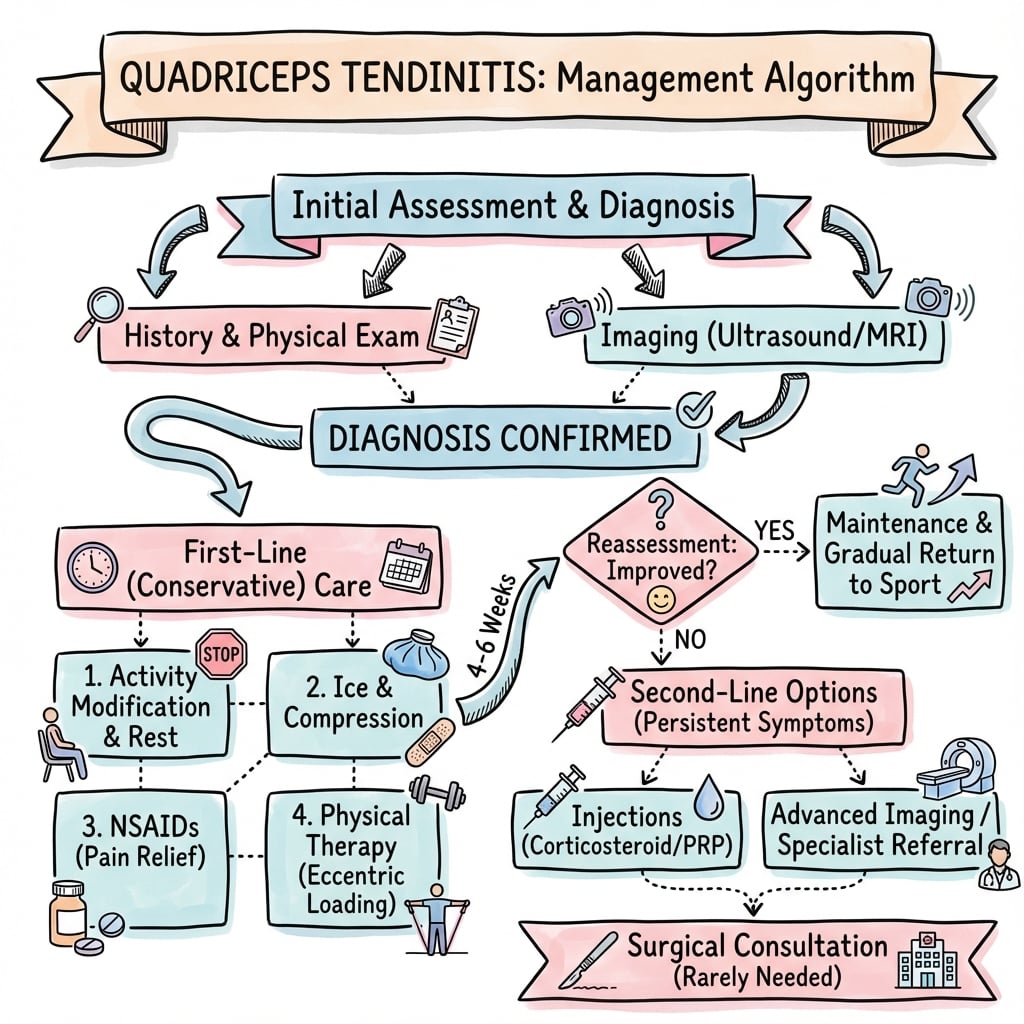
Standard therapy duration: 3-6 months.
Surgical Technique
Open Debridement and Repair:
Approach:
- Midline longitudinal incision extending proximal to patella.
- Expose paratenon.
Technique:
- Inspection: Incise paratenon. Pre-operative MRI guides location (often deep/central).
- Tenotomy: Longitudinal split in tendon to access deep layers.
- Debridement: Excise grey/friable/mucinoid tissue. "Scrape" the superior pole if cystic change present.
- Spur Removal: If a traction spur exists ("tooth"), remove with rongeur/burr to prevent impingement.
- Calcium: If calcific deposit, excise white, chalky material.
- Closure:
- Carefully repair the longitudinal split (Vicryl/PDS).
- If debridement leaves a defect, side-to-side closure.
- Close paratenon to prevent adhesions.
Post-op:
- Protected weight bearing in brace (locked extension) for 2 weeks.
- Gradual ROM increase.
- Slower than arthroscopic patellar procedures due to muscle violation.
Open debridement provides the most reliable access to the multi-layered pathology.
Complications
| Complication | Risk Factors | Management |
|---|---|---|
| Rupture | Steroid use, aggressive early load | Surgical Repair |
| Persistant Pain | Incomplete resection, wrong diagnosis | Re-imaging / Revision |
| Stiffness | Prolonged immobilization | MUA / Lysis of adhesions |
| Infection | Open surgery | Antibiotics +/- Washout |
Quadriceps Rupture:
- The ultimate failure of tendinosis.
- Requires urgent repair (suture anchors or transosseous tunnels).
- Delayed repair (greater than 3 weeks) significantly worsens prognosis due to retraction.
Postoperative Care and Rehabilitation
- Goal: Protect repair, wound healing.
- Brace in extension.
- WBAT in extension.
- Isometric quads.
- Goal: Regain ROM.
- Unlock brace 0-30, then 0-60, then 0-90.
- Active flexion, passive extension.
- Avoid active extension against resistance.
- Goal: Strength.
- Wean brace.
- Start concentric strengthening.
- Progress to eccentric loading.
- Goal: Power and Sport.
- Plyometrics.
- Return to sport criteria (limb symmetry index greater than 90%).
Post-op rehab for quadriceps tendon debridement is typically slower than patellar tendon debridement because the muscle belly itself is often more affected by the surgical approach and inhibition.
Outcomes and Prognosis
- Conservative: High success rate (70-90%) with compliance to activity modification and rehab.
- Surgical: Good results (80-90% satisfaction) in appropriately selected patients.
- Recurrence: Can occur if biomechanics (training errors, flexibility) are not addressed.
- Calcific Tendinitis: excellent prognosis with lavage or excision.
Controversies and Areas of Uncertainty
- Extrapolated evidence: Almost every high-quality loading and injection trial studied the patellar tendon, not the quadriceps tendon. The shared eccentric-loading biology makes extrapolation reasonable, but it should be acknowledged honestly in a viva rather than quoting "Level I evidence for quadriceps tendinopathy".
- PRP: Popular but the evidence is heterogeneous and preparation-dependent. Patellar tendon data are cautiously favourable; routine first-line use is not supported.
- Eccentric decline squats vs HSR: Classic eccentric decline-squat protocols can provoke compressive/insertional pain at the superior pole in quadriceps disease. Heavy slow resistance and isometric-led progression are increasingly preferred, especially early.
- Compressive vs tensile model: Insertional quadriceps tendinopathy is partly a compressive problem (deep flexion compresses the deep fibres against the trochlea). This challenges the older purely tensile-overload model and changes early rehab (limit deep flexion initially).
- Surgery for tendinosis: Debridement evidence is largely low-level case series; selection (failed prolonged rehab, structural partial tear, symptomatic enthesophyte) matters more than the specific technique.
- Calcific vs degenerative: Calcific tendinitis is a distinct entity (self-limiting resorptive cycle, often responsive to barbotage/shockwave) and should not be lumped with degenerative tendinosis.
Evidence Base
All evidence below has been verified against PubMed. Several landmark trials are drawn from the patellar tendon (jumper's knee) literature because high-quality, tendon-specific quadriceps trials are scarce; the loading biology is shared, but the limitation should be stated explicitly in a viva.
- Review of symptomatic Achilles, patellar, ECRB and rotator cuff tendons.
- Symptomatic tendons show disorganised collagen, increased mucoid ground substance and fibroblastic/myofibroblastic proliferation with neovascularisation.
- The most significant feature is the ABSENCE of inflammatory cells - this is tendinosis, not tendinitis.
- RCT of 39 men with patellar tendinopathy: corticosteroid injection (CORT) vs eccentric decline squats (ECC) vs heavy slow resistance (HSR), 12 weeks.
- All three improved VISA-P and pain at 12 weeks, but CORT deteriorated by 6-month follow-up while ECC and HSR were maintained.
- HSR produced the highest treatment satisfaction and increased collagen turnover.
- Single-blind randomised cross-over in volleyball players with patellar tendinopathy.
- A single bout of isometric contractions reduced single-leg decline squat pain (mean reduction 6.8/10) with analgesia sustained at 45 minutes, versus 2.6/10 for isotonic.
- Isometrics also released cortical inhibition and increased maximal voluntary contraction.
- In-season RCT of 20 jumping athletes: isometric leg-extension holds vs isotonic leg extension over 4 weeks.
- Both reduced pain, but isometric contractions produced significantly greater immediate analgesia throughout the trial.
- Week-one analgesic response correlated with VISA-P improvement at 4 weeks.
- Systematic review (Level I-IV) of PRP across Achilles, patellar, lateral elbow and rotator cuff tendons.
- Patellar tendon appeared to benefit from PRP, whereas Achilles did not; rotator cuff surgical augmentation showed no benefit.
- Overall evidence remains heterogeneous with variable PRP preparations.
- Case series of 14 distal quadriceps tendon tears in NFL players (1994-2004).
- Eccentric contraction was the commonest mechanism; prodromal symptoms and predisposing factors were usually absent.
- Despite timely surgical repair only 50% returned to regular-season play - a guarded prognosis even in elite athletes.
- Critical analysis review of chronic quadriceps tendon rupture.
- Delayed diagnosis leads to poorer results regardless of treatment - timely diagnosis and repair of acute injury are imperative.
- Chronic cases require V-Y lengthening, vastus advancement or autograft/allograft augmentation owing to retraction and patellar migration.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old weightlifter presents with chronic pain just above the patella. It hurts deep in the squat. X-rays show a small spur at the superior pole. How do you manage him?”
“A 55-year-old diabetic male presents with bilateral suprapatellar pain and difficulty climbing stairs. He has a history of renal disease. What is your concern?”
“Ultrasound reports a 1cm calcific deposit in the quadriceps tendon of a 35-year-old female. She has failed physiotherapy. Options?”
MCQ Practice Points
Q: Which layer of the quadriceps tendon is deepest? A: Vastus Intermedius. (Superficial: RF, Middle: VL/VM, Deep: VI).
Q: Which antibiotic class is associated with tendon rupture? A: Fluoroquinolones (e.g., Ciprofloxacin).
Q: Where is the 'watershed' zone of hypovascularity in the quad tendon? A: 1-2 cm proximal to the superior pole of the patella.
Q: A patient on dialysis with knee pain likely has pathology in which tendon? A: Quadriceps tendon (strongly associated with renal failure/secondary hyperparathyroidism).
Q: What is the 'Tooth Sign' on lateral knee X-ray? A: A traction enthesophyte (spur) at the superior pole of the patella, indicative of chronic quadriceps tendinopathy.
Q: Where is a bipartite patella typically located? A: Superolateral pole (Saupe Type III).
Guidelines, Registries & Global Practice
Global epidemiology:
- Quadriceps tendinopathy is substantially less common than patellar tendinopathy ("jumper's knee"), affecting an older cohort (typically over 35-40 years), with male predominance and a strong association with jumping/weightlifting sports.
- Complete quadriceps tendon rupture has an estimated incidence of roughly 1 per 100,000 per year, peaks in men over 40, and is over-represented in patients with chronic kidney disease, diabetes, hyperparathyroidism, gout and systemic inflammatory disease.
- There is no implant or arthroplasty registry that tracks tendinopathy; epidemiology is drawn from cohort series rather than national registries.
Side-by-side society positions (loading-led, injection-cautious):
| Body | Loading | Injections | Surgery |
|---|---|---|---|
| AAOS / AMSSM (US) | Progressive resistance (HSR / eccentric) first-line | PRP optional in recalcitrant cases; steroid discouraged | Reserved for failed prolonged rehab |
| BOA / NICE-aligned (UK) | Structured physiotherapy and load management first-line | Limited routine injection role; avoid intratendinous steroid | Specialist referral after failed conservative care |
| ESSKA / EFOST (Europe) | Exercise therapy cornerstone; ESWT as adjunct | PRP considered; heterogeneous evidence acknowledged | Debridement for chronic recalcitrant tendinosis |
| IOC consensus (sport) | Graded loading and relative rest; manage training load | Caution with injectables in-season; no steroid | Last resort; protect return-to-sport timeline |
Registry & high- vs limited-resource practice:
- High-resource settings: ready access to ultrasound and MRI allows confident differentiation of tendinosis from partial/complete tear; ultrasound-guided barbotage and shockwave are widely available; supervised graded loading programmes are standard.
- Limited-resource settings: diagnosis is clinical and radiographic (the "tooth sign" enthesophyte and the palpable suprapatellar gap of rupture become critical); home-based isometric and heavy-slow-resistance programmes are emphasised because they need minimal equipment; acute rupture repair is prioritised over advanced adjuncts.
- Across all settings the consensus is identical on two points: progressive mechanical loading is the cornerstone, and intratendinous corticosteroid is contraindicated because of rupture risk.
Key Facts
- Insertion: Superior pole of patella
- Age group: Older (over 40) than Jumper's Knee
- Deep flexion (greater than 90°) aggravates pain
- Systemic link: Renal, Diabetes, Steroids
Imaging
- X-ray: Tooth sign (spur) at superior pole
- US/MRI: Hypoechoic/High signal in critical zone
- Hypovascular zone: 1-2cm proximal to insertion
- Always rule out partial tear
Management
- Isometrics to HSR to Eccentrics
- Limit deep flexion in early phase
- Barbotage for calcific deposits
- Surgery for failed conservative / rupture
Red Flags
- Bilateral symptoms (Systemic cause)
- Extensor lag (Rupture)
- Inability to SLR (Rupture)
- Fluoroquinolone use