Episodic Digital Vasospasm - Is It Primary or Secondary?
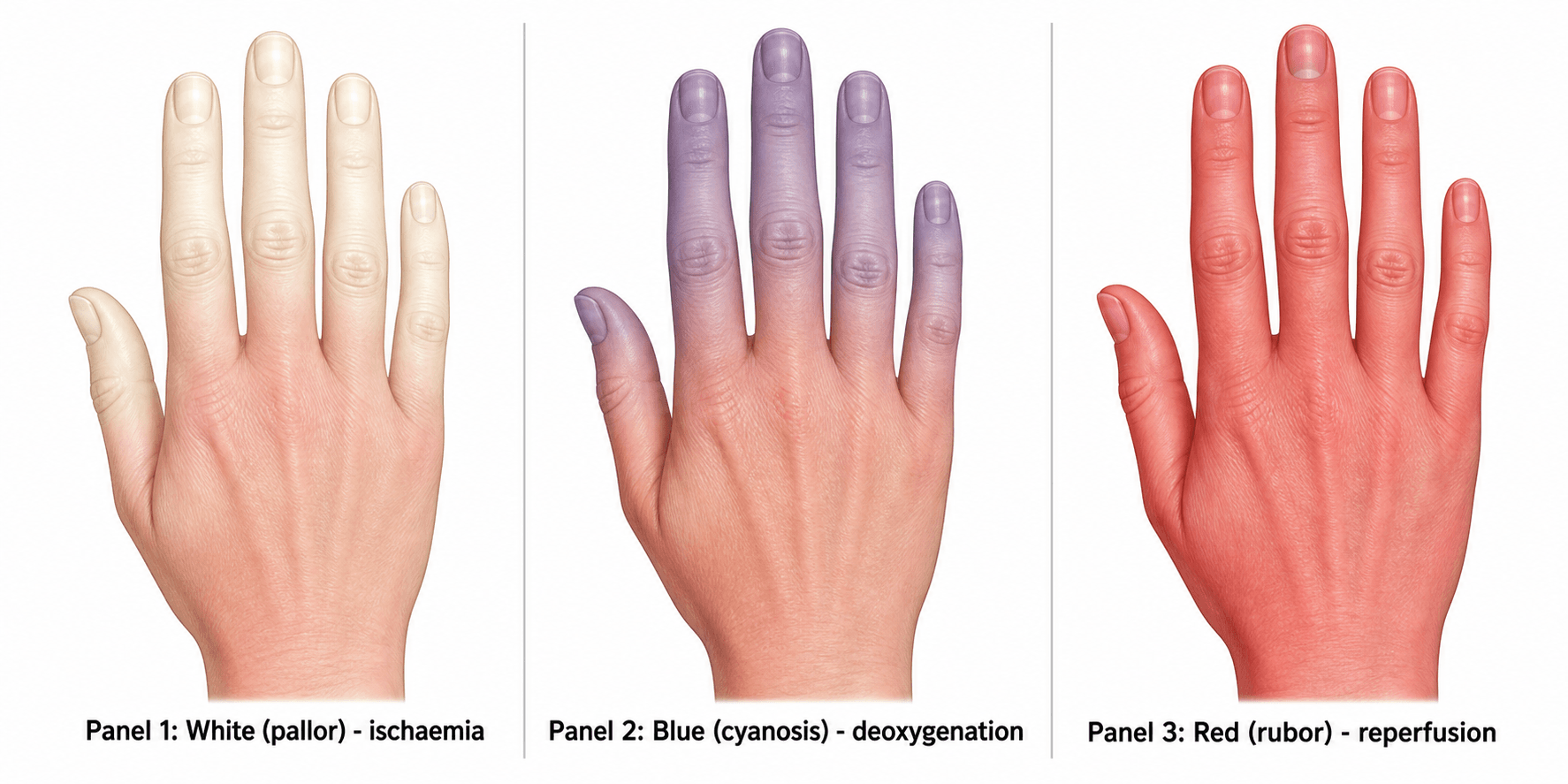
- Raynaud's phenomenon is episodic VASOSPASM of the digital arteries triggered by COLD or EMOTIONAL stress, producing the classic TRIPHASIC colour change: WHITE (pallor from ischaemia) -> BLUE (cyanosis from deoxygenation) -> RED (rubor from reperfusion hyperaemia), with accompanying numbness, pain and tingling.
- The cardinal task is to separate PRIMARY Raynaud's (Raynaud's disease - no underlying cause) from SECONDARY Raynaud's (phenomenon - with an underlying cause). Primary disease is more common, affects younger WOMEN, is symmetrical and mild with no tissue loss, normal nailfold capillaries and negative autoimmune workup, and is benign.
- SECONDARY Raynaud's most often reflects a CONNECTIVE TISSUE DISEASE - SYSTEMIC SCLEROSIS is the commonest cause - but also SLE, mixed connective tissue disease and dermatomyositis; non-rheumatic causes include occupational hand-arm VIBRATION (vibration white finger), HYPOTHENAR HAMMER SYNDROME, drugs (beta-blockers, ergot, chemotherapy, stimulants), and haematologic/vascular disease.
- RED FLAGS for a secondary cause are: onset after age ~40, MALE sex, ASYMMETRIC attacks, SEVERE episodes with digital ULCERS/pitting/tissue loss, ABNORMAL nailfold capillaroscopy and POSITIVE autoantibodies or systemic features - these warrant rheumatology referral and a search for the cause.
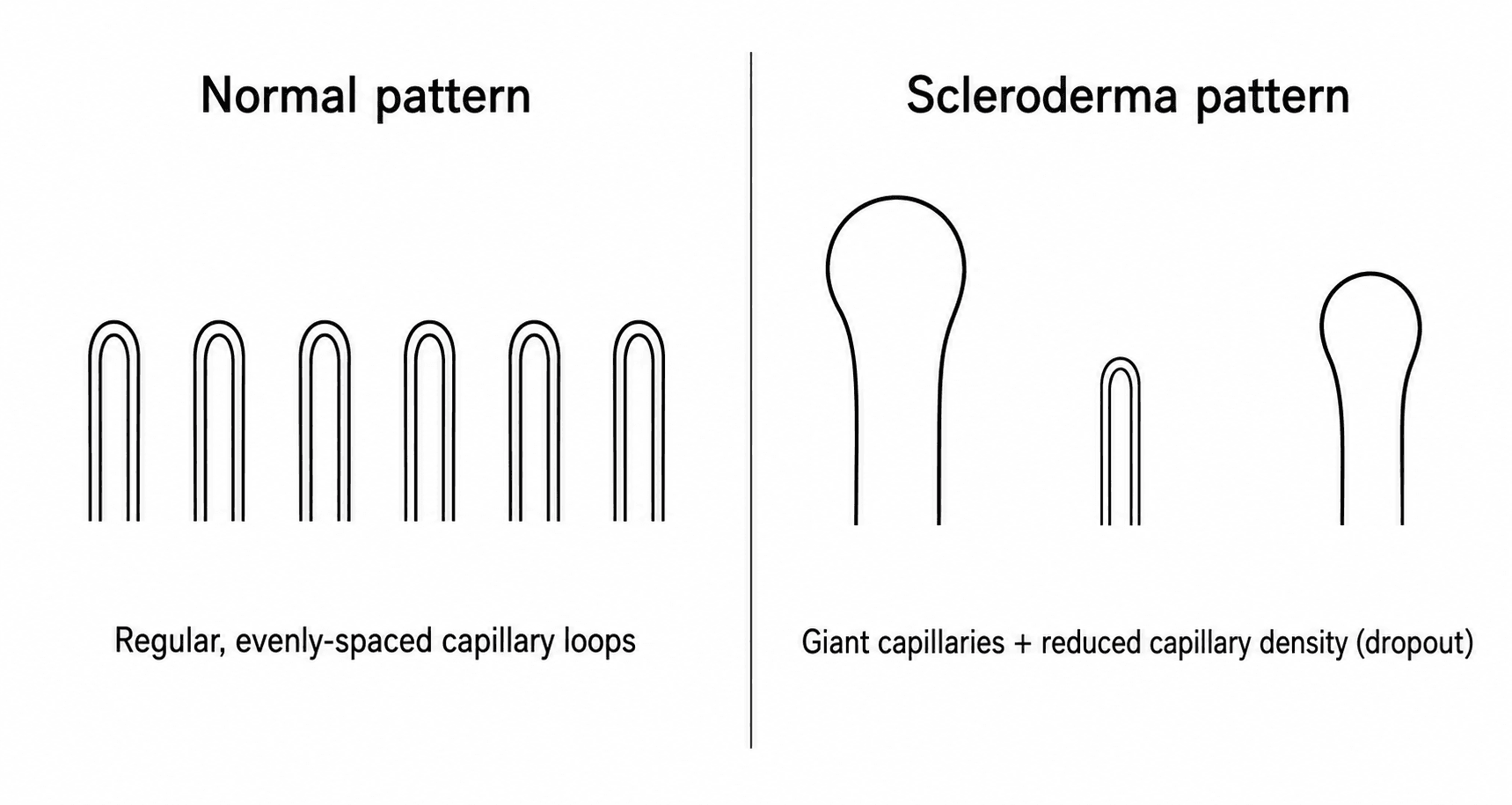
- WORKUP: history (drugs, vibration/occupation, systemic symptoms) and examination (digital ulcers, sclerodactyly, telangiectasia, calcinosis), NAILFOLD CAPILLAROSCOPY (giant capillaries and reduced capillary density define a 'scleroderma pattern'), and autoantibodies (ANA, anti-centromere, anti-Scl-70) with inflammatory markers; an Allen's test and vascular assessment if a localised arterial cause is suspected.
- MANAGEMENT is a ladder: first CONSERVATIVE - keep the hands and body WARM (gloves, hand warmers), STOP SMOKING, avoid vasoconstrictors (non-selective beta-blockers, stimulants) and treat stress; first-line DRUG therapy is a dihydropyridine CALCIUM-CHANNEL BLOCKER (nifedipine/amlodipine), with PDE5 inhibitors (sildenafil), topical nitrates, ARBs or alpha-blockers as alternatives; for severe digital ischaemia/ULCERS (especially in systemic sclerosis) IV PROSTACYCLIN (iloprost) and endothelin antagonists (bosentan to prevent new ulcers) are used, and SURGERY (digital sympathectomy, botulinum toxin, or treating an underlying hypothenar hammer/embolic source) is reserved for refractory critical ischaemia.
- “Triphasic colour change: WHITE (ischaemia) -> BLUE (cyanosis) -> RED (reperfusion).
- “Primary = benign (young woman, symmetric, normal capillaroscopy, ANA-negative); Secondary = systemic sclerosis #1 (red flags: >40, male, asymmetric, ulcers, abnormal capillaroscopy, +autoantibodies).
- “Ladder: warmth/stop smoking/avoid beta-blockers -> CCB (nifedipine) first-line -> PDE5/prostacyclin/bosentan for ulcers -> surgery (digital sympathectomy) for refractory ischaemia. Exclude hypothenar hammer syndrome.
Young woman, symmetric, mild, no tissue loss, normal nailfold capillaries, negative ANA/normal markers. Reassure + conservative care.
Onset >40/male, asymmetric, severe with digital ulcers, abnormal capillaroscopy, positive autoantibodies - think systemic sclerosis; refer to rheumatology.
Presentation & the Triphasic Colour Change
An attack is provoked by cold or emotion and classically passes through three colours: WHITE (pallor) as the digital arteries vasospasm and the finger becomes ischaemic; BLUE (cyanosis) as the static blood deoxygenates; and RED (rubor) as vasospasm resolves and reactive hyperaemia floods the finger. The colour change is usually well demarcated, affects the fingers (sparing the thumb in some), and is accompanied by numbness, tingling and pain, then throbbing on rewarming. Not every patient shows all three phases, but the sharply demarcated pallor of digital ischaemia is the hallmark.

Primary vs Secondary & Workup
Primary Raynaud's is common, benign and needs no extensive workup if the picture is typical (young woman, symmetric, mild, normal examination). Secondary Raynaud's must be actively sought, because it can herald a serious systemic disease. Red flags: onset after ~40, male sex, asymmetry, severe attacks with digital ulcers/pitting/gangrene, abnormal nailfold capillaries and positive autoantibodies. Causes include:
- Connective tissue disease - systemic sclerosis (commonest), SLE, MCTD, dermatomyositis/polymyositis.
- Occupational/vascular - hand-arm vibration syndrome (vibration white finger), hypothenar hammer syndrome, thoracic outlet syndrome, atherosclerosis, emboli.
- Drugs - beta-blockers, ergot, chemotherapy, sympathomimetics/stimulants.
- Haematologic - cryoglobulinaemia, polycythaemia. Investigations: examine for sclerodactyly/telangiectasia/calcinosis/ulcers; nailfold capillaroscopy (giant capillaries + reduced capillary density = scleroderma pattern); ANA/ENA (anti-centromere, anti-Scl-70) and inflammatory markers; Allen's test/vascular imaging if a localised arterial cause is suspected.
What the Tests Actually Buy You: Predicting Who Progresses
Capillaroscopy and autoantibodies are usually described as ways to classify a patient as primary or secondary. Their real value is prognostic - Raynaud's commonly precedes a connective tissue disease by years, so the question at the first consultation is not only "is there a disease now?" but "will there be one?"
The largest prospective answer comes from a multicentre registry of 1,150 patients presenting with Raynaud's phenomenon and no definable connective tissue disease, followed for a median of 3.6 years, which assessed four features: ANA positivity, systemic-sclerosis-specific autoantibodies, abnormal nailfold capillaroscopy and PUFFY FINGERS.
- What happened
- Only 4 of 37 ANA-negative patients (10.8%) progressed - the strongest protective factor in the study
- What it means in clinic
- This is what licenses genuine reassurance rather than a label. A negative ANA is the single most useful result for the patient who wants to know whether this becomes something
- What happened
- 16 of 17 (94.1%) progressed - the highest-risk combination
- What it means in clinic
- Effectively a pre-clinical systemic sclerosis. Refer, do not observe
- What happened
- Progressively higher risk with each feature present
- What it means in clinic
- Stratify rather than dichotomise - risk is graded, not binary
- What happened
- 52.4% progressed
- What it means in clinic
- Note the denominator: these are patients referred with Raynaud's and at least one suspicious feature, not the general population of cold-sensitive hands
Puffy fingers deserve naming, because they are easy to overlook and carry the most weight. Diffuse, non-pitting swelling of the whole finger - the fingers look sausage-like and the skin creases are lost, before any true sclerodactyly has developed - is an early scleroderma feature, and in combination with a systemic-sclerosis-specific antibody it was the highest-risk pairing in the registry. Look for it deliberately in anyone presenting with Raynaud's; it is not the same as the tapered, tight, shiny skin of established sclerodactyly, which is a later finding.
Do not over-read the headline figure. The 52.4% progression rate applies to a referred cohort enriched for suspicious features, not to every patient with cold-sensitive fingers. The clinically usable results are the extremes: ANA-negative is strongly reassuring; specific antibody plus puffy fingers is near-certain progression.
Management
- Conservative (all patients): keep the whole body and hands WARM (gloves, hand/pocket warmers, layer clothing), STOP SMOKING, manage stress, and avoid vasoconstrictors - non-selective beta-blockers, ergotamine, sympathomimetics and stimulants.
- First-line drug: a dihydropyridine CALCIUM-CHANNEL BLOCKER (nifedipine or amlodipine) reduces attack frequency and severity - the most widely used agent.
- Second-line/alternatives: PDE5 inhibitors (sildenafil), topical nitrates, ARBs (losartan), alpha-blockers (prazosin), or SSRIs (fluoxetine).
- Severe disease / digital ulcers (especially systemic sclerosis): IV prostacyclin (iloprost) for critical ischaemia/active ulcers, and the endothelin-receptor antagonist bosentan to reduce new digital ulcers.
- Refractory critical ischaemia: surgery - peripheral/digital (periarterial) sympathectomy, botulinum toxin injection, and treating any underlying arterial lesion (e.g. hypothenar hammer syndrome, embolic source); debride/amputate established gangrene.
When Raynaud's is unilateral, affects only certain digits, or presents with digital ischaemia/ulcers, exclude a local arterial cause - especially HYPOTHENAR HAMMER SYNDROME (ulnar artery aneurysm/ thrombosis at Guyon's canal from repetitive palmar trauma) and embolic sources - with an Allen's test and vascular imaging (duplex/angiography). These are surgically treatable and are missed if every case is labelled 'Raynaud's'. (See Hypothenar Hammer Syndrome and Ulnar Tunnel Syndrome / Guyon's Canal.)
Why It Spasms - and Why the Drug Ladder Works
One mechanism ties the colour change to the vasoactive drugs used to treat it. Raynaud's is an exaggerated vasoconstrictive response from an imbalance between vasoconstriction and vasodilation:
- Neural: cold and emotion drive sympathetic activity, and the digital vessels have increased alpha-2 adrenoceptor activity/sensitivity - particularly the cold-sensitive alpha-2C subtype - causing excessive smooth-muscle constriction.
- Endothelial: endothelial dysfunction with reduced nitric oxide and prostacyclin and increased endothelin-1 (a potent vasoconstrictor).
- Structural: in primary disease the spasm is functional and reversible with structurally normal vessels, whereas in secondary disease (e.g. systemic sclerosis) there is added structural narrowing (intimal proliferation/fibrosis) and intravascular factors (platelet activation, raised viscosity) - which is why secondary disease is more severe and ulcerates.
This explains the ladder: calcium-channel blockers, topical nitrates and PDE5 inhibitors (via the nitric-oxide/cGMP pathway) are vasodilators; prostacyclin (iloprost) replaces deficient prostacyclin; bosentan blocks endothelin-1; alpha-blockers oppose the adrenoceptor drive; and non-selective beta-blockers are avoided because unopposed alpha vasoconstriction worsens the spasm.
Raynaud's = vasoconstriction-vasodilation imbalance: increased alpha-2C adrenoceptor cold-sensitivity + endothelial dysfunction (low NO/prostacyclin, high endothelin-1); secondary disease adds structural narrowing. This is why CCB/nitrate/PDE5 (vasodilate), iloprost (prostacyclin) and bosentan (anti-endothelin) help and non-selective beta-blockers are avoided.
Surgery for Digital Ischaemia
Surgery is reserved for refractory critical digital ischaemia or non-healing ulcers despite maximal medical therapy, and the options are these:
- Periarterial (Leriche / digital) sympathectomy: microsurgical stripping of the adventitia - and the sympathetic fibres travelling within it - from the radial/ulnar, common and proper digital arteries, removing the sympathetic vasoconstrictor drive and improving digital perfusion.
- Botulinum toxin: injected around the neurovascular bundles in the distal palm/digits as a less-invasive chemical sympatholysis (and it reduces pain); the effect is temporary and repeatable.
- Ulcer / gangrene care: good wound care and treating infection; a dry distal gangrene may be allowed to auto-amputate (demarcate), while wet/infected or proximal gangrene needs debridement/amputation at a demarcated level.
- Always exclude a localised, reconstructable arterial lesion first - hypothenar hammer syndrome (ulnar artery resection and reversed vein graft) or an embolic source - which is surgically curable and missed if every case is labelled Raynaud's. (Those reconstructions are covered in Hypothenar Hammer Syndrome.)
For refractory digital ischaemia: periarterial (Leriche) sympathectomy (adventitial stripping of the digital arteries) or botulinum toxin (temporary chemical sympatholysis); manage the ulcer/gangrene (auto-amputation vs debridement). First exclude a reconstructable arterial lesion (hypothenar hammer syndrome / emboli) - surgically curable.
Mnemonics & Memory Aids
WBR
Hook:Raynaud's runs White -> Blue -> Red (WBR).
SECONDARY
Hook:SECONDARY lists the causes and red flags for secondary Raynaud's.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient describes their fingers going white then blue then red in the cold. How do you decide if this is primary or secondary Raynaud's, and why does it matter?”
“How would you manage a patient with troublesome Raynaud's, including one with digital ulcers from systemic sclerosis?”
Presentation
- Episodic digital vasospasm triggered by cold/emotion
- Triphasic colour: WHITE (ischaemia) -> BLUE (cyanosis) -> RED (reperfusion)
- Numbness/pain; well-demarcated pallor
Primary vs secondary
- Primary: young woman, symmetric, mild, normal capillaroscopy, ANA-negative (benign)
- Secondary causes: systemic sclerosis (#1), SLE/MCTD, vibration, HHS, drugs, haematologic
- Red flags: >40/male, asymmetric, digital ulcers, abnormal capillaroscopy, +autoantibodies
Workup
- History (drugs/occupation), exam (sclerodactyly/telangiectasia/ulcers)
- Nailfold capillaroscopy (giant capillaries + reduced density = scleroderma pattern)
- ANA/ENA (anti-centromere, Scl-70) + markers; Allen's test/imaging if local cause
Management ladder
- Warmth, stop smoking, avoid beta-blockers/stimulants, stress management
- 1st-line: dihydropyridine CCB (nifedipine); then PDE5i/nitrates/ARB/alpha-blocker
- Digital ulcers (SSc): IV iloprost + bosentan; refractory: digital sympathectomy/botox; exclude HHS
Evidence & Key Studies
Progression of Raynaud's phenomenon to systemic sclerosis: the VEDOSS multicentre longitudinal registry
- 1,150 patients with Raynaud's phenomenon and no definable connective tissue disease enrolled across 42 centres; 553 followed for a median of 3.6 years, assessed on four criteria - ANA positivity, systemic-sclerosis-specific autoantibodies, abnormal nailfold capillaroscopy and puffy fingers.
- Absence of ANA at baseline was the strongest protective factor: only 4 of 37 ANA-negative patients (10.8%) progressed to fulfil classification criteria for systemic sclerosis.
- Systemic-sclerosis-specific autoantibodies together with puffy fingers carried the highest risk - 16 of 17 (94.1%) progressed.
- Overall progression among those reaching an endpoint or five years was 52.4%, but this is a referred cohort enriched for suspicious features rather than all patients with cold-sensitive fingers.
Sociodemographic and pharmacological characteristics of patients with primary and secondary Raynaud's phenomenon
- Of 567 patients (mean age 51.9 years, 82.5% women), 58.7% had primary and 41.3% secondary Raynaud's phenomenon.
- The most frequent secondary cause was systemic sclerosis (36.8%); calcium-channel blockers were the most used drugs (45.7%).
- 9.2% of patients were taking drugs that can worsen Raynaud's (mostly non-selective beta-blockers) - a reminder to review the drug history.
Evaluation of algorithms to identify the scleroderma pattern in nailfold videocapillaroscopy
- Nailfold videocapillaroscopy is well established in evaluating Raynaud's phenomenon and systemic sclerosis.
- Reduced capillary density (<=8 capillaries/mm) best identified the scleroderma pattern (accuracy ~88%), and giant capillaries were highly specific (~98%).
- Combining giant capillaries with low density gave high accuracy (~91%) - supporting capillaroscopy to distinguish secondary (scleroderma-pattern) from primary Raynaud's.
The primary/secondary proportions, systemic sclerosis as the main secondary cause, the predominance of calcium-channel blockers and the risk of beta-blockers worsening Raynaud's come from the cited Valladales-Restrepo study, and the role of nailfold capillaroscopy (giant capillaries, reduced density) in identifying the scleroderma pattern from the cited Shinzato study. The triphasic colour change, red flags and treatment ladder are standard, well-established teaching. The progression figures - the 10.8% in ANA-negative patients, the 94.1% with a specific autoantibody plus puffy fingers, and the 52.4% overall - come from the cited VEDOSS registry, and are quoted with their referred-cohort denominator because that is what makes them interpretable. The musculoskeletal manifestations of the disease those patients are progressing towards are developed in Systemic Sclerosis: Musculoskeletal Manifestations. (See also Hypothenar Hammer Syndrome, Ulnar Tunnel Syndrome / Guyon's Canal, Frostbite and Dermatomyositis and Polymyositis.)