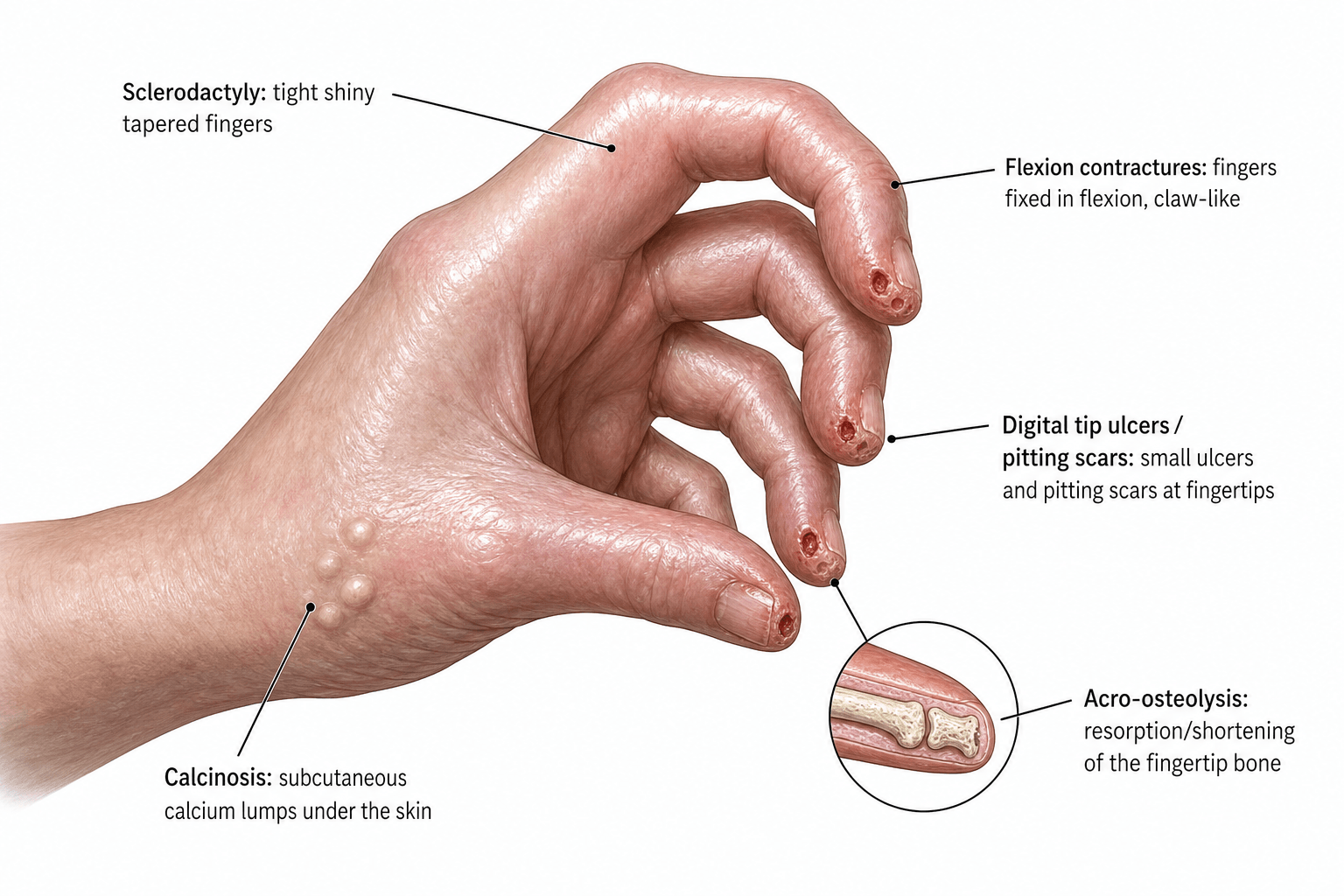
Sclerodactyly, Calcinosis, Acro-osteolysis and the Scleroderma Hand
- Systemic sclerosis (scleroderma) is an autoimmune connective-tissue disease of VASCULOPATHY and FIBROSIS; the hand is a major site, showing SCLERODACTYLY (tight, shiny, tethered, tapered skin), progressive DIGITAL FLEXION CONTRACTURES (a stiff, claw-like hand) and markedly reduced hand function.
- RAYNAUD'S phenomenon is near-universal and often the first sign; the vasculopathy causes DIGITAL ULCERS, pitting scars and, in severe disease, digital ISCHAEMIA/GANGRENE; the medical ladder for this - calcium-channel blockers, then iloprost and bosentan - is set out in full in the Raynaud's Phenomenon of the Hand topic, along with the features that predict which patients with apparently isolated Raynaud's will progress to systemic sclerosis.
- CALCINOSIS (subcutaneous calcium deposits, especially in the fingers in limited disease/CREST) can ulcerate, extrude chalky material and become infected, and ACRO-OSTEOLYSIS (resorption of the distal phalangeal tufts) reflects chronic ischaemia and severe/long-standing disease.
- TENDON FRICTION RUBS (palpable/audible creaking over moving tendons) are an important sign of DIFFUSE disease and a POOR PROGNOSTIC marker (associated with internal-organ involvement); patients may also have inflammatory ARTHRITIS, joint erosions, distal ulna resorption and a high rate of erosive osteoarthritis on hand radiographs.
- The SUBTYPE and AUTOANTIBODIES matter: LIMITED cutaneous SSc (CREST) carries ANTI-CENTROMERE antibody and pulmonary arterial hypertension risk, while DIFFUSE cutaneous SSc carries ANTI-SCL70 (topoisomerase) or ANTI-RNA-POLYMERASE III with more interstitial lung disease and scleroderma renal crisis; acro-osteolysis associates with anti-Scl70/diffuse disease and calcinosis with anti-centromere.
- MANAGEMENT is predominantly MEDICAL and rheumatology-led (immunomodulation, vasodilators, organ surveillance); ORTHOPAEDIC/HAND involvement is mostly SUPPORTIVE (hand therapy, splinting, wound care) - and SURGERY (e.g. for symptomatic calcinosis, digital ulcers/ischaemia, or contractures) must be undertaken cautiously because of the POOR WOUND HEALING, vasculopathy and infection risk of scleroderma skin.
- “Scleroderma hand: sclerodactyly + flexion contractures + Raynaud's/digital ulcers + calcinosis + acro-osteolysis.
- “Tendon friction rubs = diffuse disease + poor prognosis. Limited (CREST, anti-centromere, PAH) vs diffuse (anti-Scl70/RNA pol III, ILD/renal crisis).
- “Mostly medical/rheumatology management; operate with great caution (poor wound healing, vasculopathy) - e.g. ulcerating calcinosis, digital ischaemia.
Skin distal to elbows/knees + face; anti-centromere; calcinosis and PAH. CREST = Calcinosis, Raynaud's, Esoph. dysmotility, Sclerodactyly, Telangiectasia.
Widespread/proximal skin; anti-Scl70 / anti-RNA pol III; ILD and renal crisis; tendon friction rubs and acro-osteolysis more common.
Hand & Musculoskeletal Manifestations
The hand concentrates many features of the disease. Sclerodactyly - tight, shiny, tethered skin - gradually fixes the fingers in flexion contractures, producing a stiff, claw-like hand with poor function. The vasculopathy gives near-universal Raynaud's with digital ulcers and pitting scars at the fingertips, and in severe cases digital ischaemia/gangrene - and because Raynaud's usually precedes the diagnosis by years, the patients reaching a hand clinic with these findings are often the ones who progressed from what looked like isolated Raynaud's phenomenon (the features that predict that progression, and the ones that permit genuine reassurance, are set out in Raynaud's Phenomenon of the Hand). Calcinosis deposits chalky subcutaneous calcium (often in the fingers in limited disease), which can ulcerate and become infected, and acro-osteolysis resorbs the distal phalangeal tufts. There may be arthralgia/arthritis, joint erosions, distal ulna resorption, and a high prevalence of erosive osteoarthritis; tendon friction rubs signal diffuse disease and a worse prognosis. Hand radiographs are abnormal in roughly two-thirds of patients, increasingly so with longer disease duration.

Diagnosis & Associations
Diagnosis is clinical (ACR/EULAR criteria) supported by autoantibodies and nailfold capillaroscopy (a scleroderma pattern - giant capillaries and dropout). Key associations:
- Limited cutaneous (CREST): anti-centromere; calcinosis; pulmonary arterial hypertension risk.
- Diffuse cutaneous: anti-Scl70 (topoisomerase) or anti-RNA polymerase III; interstitial lung disease and scleroderma renal crisis.
- On hand radiographs, acro-osteolysis associates with anti-Scl70/diffuse disease and ILD; calcinosis with anti-centromere and PAH/GI involvement; flexion contracture with higher skin score and GI disease. Patients need systemic surveillance (lung function/HRCT, echocardiography for PAH, renal/BP monitoring), which is a rheumatology-led responsibility but important to know.
Management (with Surgical Caution)
- Medical (rheumatology-led): disease-modifying immunosuppression for diffuse/active disease; vasodilator therapy for Raynaud's/digital ulcers (calcium-channel blockers, PDE5 inhibitors, IV iloprost, bosentan to prevent new ulcers); organ-directed treatment (e.g. ACE inhibitors for renal crisis).
- Hand therapy: stretching, splinting, paraffin baths and occupational therapy to maintain mobility and manage contractures; skin care and meticulous wound care for ulcers.
- Surgery (selective, cautious): excision of symptomatic/ulcerating calcinosis, debridement or amputation of infected/gangrenous digits, digital sympathectomy for refractory ischaemia, and occasionally contracture correction or joint fusion - all undertaken with awareness of poor wound healing, vasculopathy and infection risk; optimise perfusion, avoid tourniquets where possible, and counsel about delayed healing and recurrence (calcinosis recurs).
The fibrotic, poorly vascularised skin of systemic sclerosis is prone to breakdown, delayed healing and infection, so any incision - for calcinosis, ulcers or contractures - carries a real risk of a non-healing wound. Reserve surgery for clear indications, optimise the vasculopathy (warmth, vasodilators, smoking cessation), handle tissues gently, and warn patients that calcinosis and digital ulcers frequently recur. Recognise and refer scleroderma renal crisis and other organ emergencies, which take priority over elective hand surgery.
Scleroderma Renal Crisis: The Emergency That Trumps Hand Surgery
- Who and what triggers it: an acute, life-threatening complication, most often in early diffuse disease with rapidly progressive skin and the anti-RNA-polymerase-III antibody, and crucially precipitated by high-dose corticosteroids - the reason steroids are used cautiously in scleroderma (directly relevant if steroids are considered for MSK symptoms or peri-operatively).
- How it presents: abrupt, severe/malignant hypertension with acute kidney injury (rising
creatinine) and a microangiopathic haemolytic anaemia with thrombocytopenia (a thrombotic microangiopathy)
- often with headache, visual disturbance, encephalopathy or pulmonary oedema.
- Treatment: prompt, aggressively titrated ACE inhibitor (e.g. captopril) is the cornerstone and is continued even as the creatinine rises because it improves survival - this is a hypertensive/renal emergency needing urgent specialist referral.
- The orthopaedic message: avoid high-dose corticosteroids in scleroderma, monitor BP and renal function, and treat SRC as taking priority over any elective hand procedure.
Scleroderma renal crisis = abrupt malignant hypertension + AKI + microangiopathic haemolysis, in early diffuse / anti-RNA-pol-III disease, precipitated by high-dose steroids. Treat with a promptly titrated ACE inhibitor (captopril), continued despite a rising creatinine. So avoid high-dose steroids in scleroderma and let SRC trump elective surgery.
Getting the Scleroderma Patient Safely Through Surgery
- Access is hard: difficult IV and arterial access from the vasculopathy and tight, tethered skin - allow time and ultrasound guidance, and be wary of an arterial line in a vasculopathic limb (digital-ischaemia risk).
- The airway: microstomia (tight perioral skin limiting mouth opening) can make intubation difficult - plan for it.
- Aspiration: oesophageal dysmotility and reflux raise the aspiration risk - use reflux precautions / a rapid-sequence approach.
- Lungs and heart: interstitial lung disease and pulmonary arterial hypertension raise anaesthetic and peri-operative risk - assess with preoperative lung function and echocardiography.
- Keep warm, protect the digits: cold precipitates Raynaud's/digital ischaemia, so keep the patient and limb warm, avoid a limb tourniquet where possible, and avoid adrenaline in digital blocks (the Raynaud's ladder itself is in Raynaud's Phenomenon of the Hand, and general anaesthetic technique in General Anaesthesia in Orthopaedics).
- Immunosuppression adds an infection risk on top of the poor skin healing.
Scleroderma surgery is risky beyond the skin: hard IV/arterial access, a difficult airway from microstomia, aspiration from oesophageal dysmotility, raised risk from ILD/PAH, and Raynaud's/digital ischaemia - so keep warm, avoid tourniquets and digital adrenaline, assess lungs/heart preoperatively, and account for immunosuppression-related infection and poor wound healing.
Mnemonics & Memory Aids
CREST
Hook:CREST = limited cutaneous systemic sclerosis (anti-centromere).
SCAR HAND
Hook:The scleroderma hand has a SCAR and HANDles surgery badly.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What are the hand and musculoskeletal manifestations of systemic sclerosis, and how do the subtypes and antibodies relate to them?”
“A scleroderma patient has painful ulcerating calcinosis and a digital ulcer. How would you manage the hand, and what surgical cautions apply?”
Hand manifestations
- Sclerodactyly + flexion contractures (claw-like, stiff)
- Raynaud's, digital ulcers/pitting scars, ischaemia/gangrene
- Calcinosis (CREST), acro-osteolysis, erosions, distal ulna resorption, erosive OA
Subtypes & antibodies
- Limited (CREST): anti-centromere; calcinosis; PAH
- Diffuse: anti-Scl70 (topoisomerase) / anti-RNA pol III; ILD; renal crisis
- Tendon friction rubs = diffuse disease + poor prognosis
Diagnosis/surveillance
- ACR/EULAR criteria + autoantibodies + nailfold capillaroscopy (scleroderma pattern)
- Hand X-ray abnormal in ~68% (acro-osteolysis, calcinosis, contracture, erosions)
- Organ surveillance: lung (PFT/HRCT), echo (PAH), renal/BP
Management
- Mostly medical (immunomodulation, vasodilators: CCB/PDE5i/iloprost/bosentan), organ-directed
- Hand therapy/splinting; wound care
- Surgery selective (ulcerating calcinosis, infection/gangrene, ischaemia) - beware poor wound healing/recurrence
Evidence & Key Studies
Musculoskeletal and radiological features in systemic sclerosis: a registry study
- In 180 SSc patients, tendon friction rubs were associated with calcinosis, muscle tenderness and flexion contracture.
- Disease duration was the main factor for developing joint erosion, acro-osteolysis, distal ulna resorption, calcinosis and flexion contracture on hand radiographs.
- Acro-osteolysis was more frequent in the diffuse subtype and with anti-topoisomerase (Scl70) antibody.
Hand X-ray findings, clinical features and autoantibodies in systemic sclerosis
- Hand X-ray abnormalities (acro-osteolysis, calcinosis, flexion contracture, erosion, joint-space narrowing, subluxation) were present in about 68% of SSc patients.
- Acro-osteolysis associated with anti-Scl70 and interstitial lung disease; calcinosis with anti-centromere and pulmonary arterial hypertension/GI involvement.
- Erosive osteoarthritis was more prevalent than in the general population; findings increased with disease duration and organ involvement.
The association of tendon friction rubs with calcinosis and contracture, and of disease duration with acro-osteolysis, calcinosis and erosion, comes from the cited Azarbani registry of 180 patients; the prevalence of hand-radiograph abnormalities (about 68%) and the antibody and organ associations - acro-osteolysis with anti-Scl70 and interstitial lung disease, calcinosis with anti-centromere and pulmonary arterial hypertension - from the cited Sakata study.
The repeated caution that scleroderma skin heals badly is stated qualitatively and deliberately without a figure: searches for a complication or non-healing rate after hand surgery in systemic sclerosis, and for recurrence rates after excision of digital calcinosis, did not identify a verified series, so the mechanism - fibrotic, poorly vascularised skin in a vasculopathic, often immunosuppressed patient - is given instead of a number that would have to be invented. The same applies to how often calcinosis and digital ulcers recur.
The CREST and limited-versus-diffuse framework, the renal-crisis presentation and its ACE-inhibitor treatment, and the peri-operative considerations are standard, well-established teaching. No dedicated connective-tissue- disease or digital-ischaemia topic exists in the library, so those threads are carried here. (See also Raynaud's Phenomenon of the Hand, General Anaesthesia in Orthopaedics and Hypothenar Hammer Syndrome.)