Low Energy Availability and Its Consequences
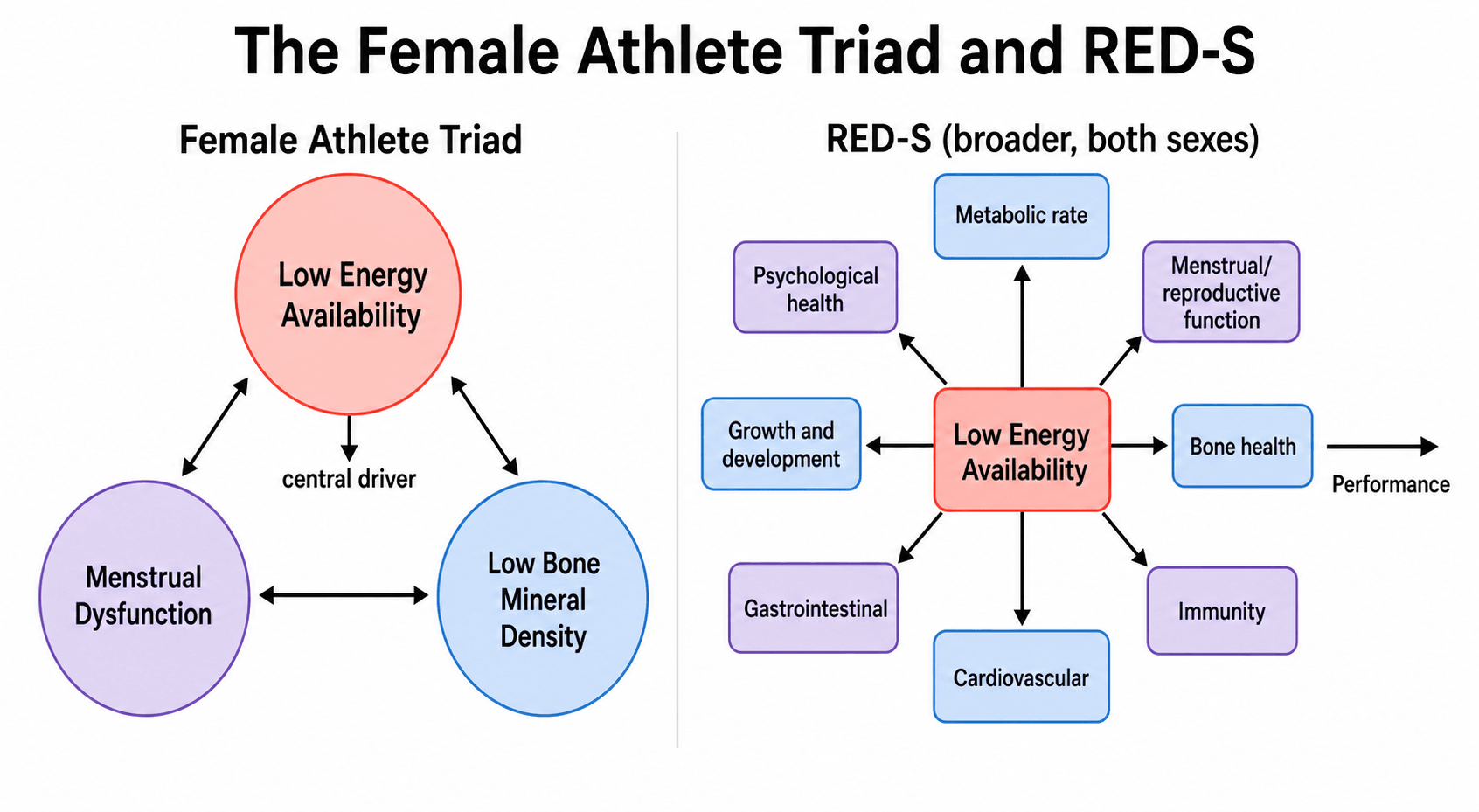
- The FEMALE ATHLETE TRIAD is the interrelated triad of LOW ENERGY AVAILABILITY (with or without disordered eating), MENSTRUAL DYSFUNCTION (most importantly functional hypothalamic amenorrhoea), and LOW BONE MINERAL DENSITY; each component exists on a spectrum from optimal health to disease, and they are causally linked.
- RELATIVE ENERGY DEFICIENCY IN SPORT (RED-S) is the broader, more recent IOC concept that recognises LOW ENERGY AVAILABILITY as impairing MANY body systems - resting metabolic rate, menstrual/reproductive function, bone health, immunity, cardiovascular and gastrointestinal function, growth and development, and psychological health - as well as impairing PERFORMANCE, and crucially it applies to BOTH SEXES (not only female athletes).
- The CENTRAL DRIVER of both is LOW ENERGY AVAILABILITY (EA), defined as dietary energy intake minus exercise energy expenditure, expressed per kg of FAT-FREE MASS; chronically low EA suppresses the hypothalamic-pituitary-gonadal axis (low GnRH/LH -> low oestrogen, causing functional hypothalamic amenorrhoea) and lowers thyroid/metabolic activity, which together impair bone health.
- The key ORTHOPAEDIC consequence is BONE: low energy availability and low oestrogen reduce bone mineral density and cause BONE STRESS INJURIES and STRESS FRACTURES (and impair healing), so a female athlete presenting with a stress fracture, especially a recurrent one or one at a TRABECULAR-rich site (sacrum, pelvis, femoral neck), should be screened for the triad/RED-S, and amenorrhoea plus a stress fracture is a major red flag.
- SCREENING and assessment combine a history of disordered eating/menstrual status/stress fractures with validated questionnaires - the Low Energy Availability in Females Questionnaire (LEAF-Q) and the Low Energy Availability in Males Questionnaire (LEAM-Q) - plus DXA for bone mineral density and, where useful, hormonal/metabolic biomarkers; risk-stratification tools guide return-to-sport decisions.
- MANAGEMENT is MULTIDISCIPLINARY (sports physician, dietitian, psychologist/psychiatrist, and the coach/athlete) and the cornerstone is RESTORING ENERGY AVAILABILITY by increasing energy intake and/or reducing exercise energy expenditure; this restores menstrual function and improves bone health, and the condition is REVERSIBLE when energy balance is restored - alongside treating any disordered eating and optimising bone health (calcium/vitamin D, and oestrogen/therapy where indicated).
- “Female Athlete Triad = LOW ENERGY AVAILABILITY + MENSTRUAL DYSFUNCTION + LOW BMD; central driver = low energy availability (intake minus exercise expenditure per kg fat-free mass).
- “RED-S (IOC) = broader: low EA impairs many systems (metabolism, reproduction, bone, immunity, CVS, GI, psychological) + performance, in BOTH SEXES.
- “Orthopaedic link = bone stress injuries/stress fractures + low BMD (amenorrhoea + stress fracture = red flag). Screen (LEAF-Q/LEAM-Q, DXA); MULTIDISCIPLINARY management restoring energy availability (reversible).
Low energy availability drives menstrual dysfunction and low BMD (the Triad); RED-S broadens this to many systems and both sexes.
A female athlete with a stress fracture (especially recurrent) and amenorrhoea should be screened - restore energy availability (the condition is reversible).
The Triad, RED-S & the Bone Link
The Female Athlete Triad is the interrelated triad of low energy availability (with or without disordered eating), menstrual dysfunction (functional hypothalamic amenorrhoea) and low bone mineral density. RED-S (the IOC term) broadens this to recognise that low energy availability impairs many systems - metabolic rate, reproduction, bone, immunity, cardiovascular and GI function, growth and psychological health - and impairs performance, in both sexes. The central driver is low energy availability (intake minus exercise energy expenditure per kg fat-free mass), which suppresses the hypothalamic-pituitary- gonadal axis (low oestrogen) and metabolic activity, impairing bone. The key orthopaedic consequence is bone stress injuries and stress fractures with low BMD - so a female athlete with a stress fracture (especially recurrent) and amenorrhoea should be screened, and the condition is reversible when energy availability is restored.
- Female Athlete Triad
- Low energy availability + menstrual dysfunction + low BMD
- RED-S (IOC)
- Low energy availability impairing many systems
- Female Athlete Triad
- Female athletes
- RED-S (IOC)
- Both sexes
- Female Athlete Triad
- 3 interrelated components
- RED-S (IOC)
- Multisystem (metabolism, reproduction, bone, immunity, CVS, GI, psychological) + performance
- Female Athlete Triad
- Low energy availability
- RED-S (IOC)
- Low energy availability
Confirming the Diagnosis Before You Label It
Functional hypothalamic amenorrhoea is a diagnosis of exclusion, and labelling an athlete's missing periods as "just her training" without testing is a real clinical error - it delays the diagnosis of conditions that need entirely different treatment.
- Always exclude pregnancy first with a beta-hCG. It is the commonest cause of secondary amenorrhoea in a woman of reproductive age, athlete or not.
- Thyroid disease and hyperprolactinaemia - TSH and prolactin. A prolactinoma presents exactly this way and will not respond to eating more.
- Polycystic ovary syndrome, which is common and can coexist with athletic training; clinical hyperandrogenism and testosterone help separate it. The distinction matters because PCOS is not a state of oestrogen deficiency and does not carry the same bone risk.
- Premature ovarian insufficiency - an elevated FSH points away from a hypothalamic cause, since functional hypothalamic amenorrhoea produces low or inappropriately normal LH and FSH with low oestradiol.
- Coeliac disease and inflammatory bowel disease, which cause inadvertent energy deficiency through malabsorption rather than through under-eating.
Alongside these, check full blood count, ferritin, vitamin D, calcium and renal function, and consider T3 - a low T3 is one of the more useful markers of ongoing energy deficiency. DXA is indicated after six or more months of amenorrhoea, after a bone stress injury, with disordered eating, or at a very low BMI.
Restoring Bone: What Works, and the Contraceptive Trap
The single point most likely to be tested, and most often got wrong, concerns the combined oral contraceptive pill.
The combined oral contraceptive does not treat this condition. Prescribing it to an amenorrhoeic athlete is intuitive and wrong for two reasons. First, it has not been shown to restore bone mineral density in functional hypothalamic amenorrhoea, because the problem is not simply absent oestrogen - low energy availability independently suppresses bone formation through low IGF-1 and low T3, and no amount of exogenous oestrogen corrects an energy deficit. Second, and more insidiously, it produces a withdrawal bleed that looks like a period, which masks the single best clinical marker of recovery: the spontaneous return of menses. An athlete on the pill can appear to be improving while her energy deficit continues untreated.
What to do instead:
- Restoring energy availability is the treatment, and the return of spontaneous menstruation is the endpoint that tells you it has worked. Everything else is adjunctive.
- Calcium and vitamin D to recommended intakes, correcting a measured deficiency.
- Where pharmacological oestrogen is judged necessary - typically a persistently low BMD with continuing bone stress injuries despite genuine attempts at nutritional restoration - transdermal 17-beta-oestradiol with cyclic progestogen is preferred over the oral pill, because it avoids the hepatic first-pass effect that suppresses IGF-1 and therefore does not blunt bone formation in the way oral ethinyl oestradiol does.
- Bisphosphonates are generally avoided in young women of childbearing potential: the evidence in this population is thin, and their very long skeletal half-life raises unresolved concerns about a future pregnancy.
- If the athlete needs contraception for contraception's sake, that is a legitimate separate indication - but it should be prescribed knowing it neither treats the bone nor allows menses to be used as a recovery marker.
Putting Numbers on Energy Availability
- The definition (units matter): EA = dietary energy intake minus exercise energy expenditure, per kg of fat-free mass per day (kcal/kg FFM/day) - it is the energy left over for normal physiological function after training.
- Optimal EA is around 45 kcal/kg FFM/day - roughly energy balance, supporting normal reproductive, metabolic and bone function.
- The disruption threshold is around 30 kcal/kg FFM/day: below this, LH pulsatility and reproductive function are suppressed, metabolic hormones fall (low T3, reduced resting metabolic rate) and bone-formation markers drop - so chronically low EA below roughly 30 drives the triad/RED-S.
- Critically low EA (e.g. the cited case below 10 kcal/kg FFM/day) causes profound disruption.
- Either side of the equation: the deficit can come from reduced intake (disordered eating) and/or high exercise expenditure - and the management goal of "restoring energy availability" means bringing EA back toward around 45.
Use the threshold as a concept, not as a test
Two cautions belong with those numbers. The 30 kcal/kg figure comes from short-term laboratory studies in small groups of young women, and it describes the point at which measurable disruption appeared in that setting - it was never validated as an individual diagnostic cut-off. In practice, energy availability is also very hard to measure accurately in a free-living athlete, because it compounds the well-known unreliability of self-reported dietary intake with an estimate of exercise energy expenditure and a body-composition measurement, so a calculated EA carries a wide margin of error.
The 2023 IOC consensus reflects this by moving away from a single threshold toward a physiological model that distinguishes adaptable from problematic low energy availability, modified by individual factors - the same calculated EA may be benign in one athlete over a short period and damaging in another sustained for months. The practical consequence for the exam and the clinic is the same: a calculated EA above 30 does not exclude the diagnosis in an athlete who has stopped menstruating and is breaking bones. Treat the number as a way of understanding the mechanism and framing the dietary conversation, not as a rule-in or rule-out test.
EA = intake minus exercise expenditure per kg fat-free mass per day. ~45 kcal/kg FFM/day = optimal; below ~30 = the disruption threshold (suppressed LH/reproduction, low T3/RMR, falling bone formation) → triad/RED-S; the cited case was critically low (below 10). "Restore energy availability" = push EA back toward ~45.
Reading the DXA in an Athlete: Z-Scores, Not T-Scores
- Use the Z-score, not the T-score: in premenopausal women, children/adolescents and men under 50 the age- and sex-matched Z-score is the correct measure (the T-score, comparing to young-adult peak, is for postmenopausal women and older men - covered in our Osteoporosis topic).
- The athlete caveat: weight-bearing/impact athletes normally have higher-than-average BMD, so a Z-score that looks "normal" may be abnormally low for an athlete - hence the Female-Athlete-Triad/ACSM definition of "low BMD" as a Z-score below -1.0 in an athlete with secondary risk factors (low EA, amenorrhoea, prior stress fracture), rather than the general -2.0 cutoff.
- Terminology: in this young population a Z-score of -2.0 or lower with secondary clinical risk factors supports "osteoporosis"; otherwise "low bone mass / below the expected range for age" is the preferred term.
- Sport matters: athletes in non-weight-bearing sports (cyclists, swimmers) can have low BMD even without the triad. DXA is also used to monitor the response to restoring energy availability over time.
In a young athlete use the Z-score, not the T-score. Because impact athletes normally have high BMD, the triad threshold for "low BMD" is a Z-score below -1.0 with risk factors (not the general -2.0); a Z-score of -2.0 or lower plus risk factors supports osteoporosis. Cyclists/swimmers can be low even without the triad.
Screening & Management
- Screen the at-risk athlete: history of disordered eating, menstrual status (amenorrhoea/oligomenorrhoea), and stress fractures; validated questionnaires (LEAF-Q for females, LEAM-Q for males); DXA for bone mineral density; hormonal/metabolic biomarkers where useful.
- Have a low threshold orthopaedically: any female athlete with a bone stress injury/stress fracture - especially recurrent, or amenorrhoeic - should be assessed for the triad/RED-S.
- Restore energy availability (the cornerstone): increase energy intake and/or reduce exercise energy expenditure - this restores menstrual function and improves bone health, and the condition is reversible.
- Multidisciplinary care: sports physician, dietitian, psychologist/psychiatrist (treat disordered eating), with the coach and athlete; optimise bone health (calcium/vitamin D; oestrogen/therapy where indicated).
- Risk-stratified return to sport guides clearance and ongoing participation.
The orthopaedic trap in the Female Athlete Triad / RED-S is to treat the presenting bone stress injury or stress fracture in isolation and miss the underlying low energy availability that caused it - which guarantees recurrence. A female athlete with a stress fracture, particularly a recurrent one, one at a trabecular-rich site, or with amenorrhoea, should be screened for the triad with a history of disordered eating and menstrual status, questionnaires and DXA, and managed by restoring energy availability within a multidisciplinary team, not just rested and returned. Because the condition is reversible when energy balance is restored, early recognition and correction of the energy deficit prevent long-term consequences for bone health and fertility; conversely, returning an under-fuelled, amenorrhoeic athlete to full training without addressing the energy deficit is how stress fractures and low bone density recur.
Which bone stress injuries should raise the question
Not every stress fracture points to an energy deficit, and knowing which ones do is what makes the screening decision practical. Bone stress injuries at trabecular (cancellous) sites - the sacrum, pubic rami, femoral neck and calcaneus - are the ones most associated with low bone mineral density and hormonal disruption, because trabecular bone has a high surface area and turns over fast, so it registers oestrogen deficiency early. Injuries at predominantly cortical sites - the tibial shaft and metatarsals - are more often explained by training load, surface, footwear and biomechanics. A sacral or femoral neck stress fracture in a young female endurance athlete should therefore trigger a full RED-S assessment almost reflexively, while a second metatarsal stress fracture in a runner who has just doubled her mileage may be exactly what it looks like. Multiple or recurrent stress injuries at any site, and any stress injury in an athlete with menstrual disturbance, warrant the workup regardless. Note this is a different axis from the familiar high-risk versus low-risk classification, which describes the risk of non-union and the need for aggressive treatment rather than the likelihood of an underlying energy deficit - see Stress Fractures.
Mnemonics & Memory Aids
ENERGY
Hook:ENERGY: low Energy availability, No periods, Eroded bone, RED-S (broader/both sexes), Generalised screen, Yes reversible (restore EA).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A female distance runner presents with a stress fracture and tells you her periods stopped a year ago. What condition are you concerned about?”
“How would you manage the Female Athlete Triad / RED-S?”
Definitions
- Female Athlete Triad: low energy availability + menstrual dysfunction + low BMD
- RED-S (IOC): low EA impairing many systems + performance, both sexes
- Central driver: low energy availability (intake minus exercise expenditure per kg FFM)
Mechanism & link
- Low EA -> suppressed HPG axis (low oestrogen) -> amenorrhoea
- Low oestrogen + metabolic suppression -> low BMD
- Orthopaedic consequence: bone stress injuries / stress fractures
Screening
- History: disordered eating, menstrual status, stress fractures
- LEAF-Q (females) / LEAM-Q (males); DXA for BMD
- Amenorrhoea + stress fracture = major red flag
Management
- Multidisciplinary (sports physician, dietitian, psychologist; athlete + coach)
- Cornerstone: restore energy availability (increase intake / reduce expenditure) - reversible
- Treat disordered eating; optimise bone health; risk-stratified return to sport
Evidence & Key Studies
Energy availability and low energy availability as the mechanism of RED-S (narrative review)
- Energy availability (EA) is dietary energy remaining after exercise energy expenditure; chronic low EA (LEA) is the underlying mechanism of Relative Energy Deficiency in Sport (RED-S).
- LEA is associated with alterations in thyroid and reproductive hormones, reduced resting metabolic rate, lower bone mineral density and delayed recovery.
- Screening questionnaires (LEAF-Q for females, LEAM-Q for males) help identify at-risk athletes, with hormonal/metabolic biomarkers improving detection.
2023 International Olympic Committee consensus statement on Relative Energy Deficiency in Sport (REDs)
- Updates the 2014 and 2018 statements on the back of more than 170 new studies, and adopts the abbreviation REDs; low energy availability remains the exposure driving the syndrome in both female and male athletes.
- Introduces a Physiological Model distinguishing ADAPTABLE from PROBLEMATIC low energy availability, modified by individual factors - a deliberate move away from treating a single energy-availability threshold as diagnostic.
- Introduces the REDs Clinical Assessment Tool version 2 (CAT2), which grades severity and risk to guide training and competition decisions, and highlights emerging evidence on low carbohydrate availability, the interplay with mental health, and the impact of low energy availability in males.
Reversibility of the Female Athlete Triad when energy balance is restored (case report)
- The Female Athlete Triad and RED-S are associated with low energy availability, causing menstrual dysfunction, impaired bone health and metabolic disturbances.
- A triathlete with critically low energy availability (under 10 kcal/fat-free mass/day), hypothalamic amenorrhoea and low bone density (lumbar Z-score -2.3) recovered menstrual and reproductive function when training reduced and intake improved.
- The case highlights the reversibility of the Female Athlete Triad when energy balance is restored, underscoring the importance of early intervention.
The definition of energy availability and low energy availability as the mechanism of RED-S (with hormonal, metabolic, bone and recovery consequences) and the LEAF-Q/LEAM-Q screening tools come from the cited Espinar review; the components of the Female Athlete Triad, the link of critically low energy availability with amenorrhoea and low bone density, and the reversibility when energy balance is restored from the cited Gama case report. The triad-versus-RED-S framing, the orthopaedic link to bone stress injuries/stress fractures, the DXA assessment, and the multidisciplinary, energy-availability-restoring management are standard, well- established teaching. The REDs terminology, the adaptable-versus-problematic low-energy-availability model, the CAT2 assessment tool and the move away from a single diagnostic threshold come from the cited 2023 IOC consensus. The ineffectiveness of the combined oral contraceptive at restoring bone density and its masking of the return of menses, the preference for transdermal oestradiol, and the exclusion of other causes of amenorrhoea are standard endocrine and sports-medicine teaching. (See also Stress Fractures, Femoral Neck Stress Fractures and Osteoporosis.)