Muscle Breakdown | CK Elevation | Myoglobinuria | Acute Kidney Injury
RHABDOMYOLYSIS SEVERITY
Critical Must-Knows
- CK over 10,000 U/L is diagnostic threshold for rhabdomyolysis
- Myoglobinuria (dark tea-colored urine) indicates significant muscle breakdown
- Acute kidney injury from myoglobin tubular obstruction - prevent with aggressive fluids
- Hyperkalemia from muscle necrosis - cardiac risk, monitor ECG
- Urine alkalinization (pH over 6.5) reduces myoglobin precipitation in tubules
Clinical Pearls
- "Target urine output over 200ml/hr with aggressive IV fluids (4-6L first 24h)
- "Sodium bicarbonate alkalinizes urine - prevents myoglobin precipitation
- "Compartment syndrome is most common orthopaedic cause
- "CK peaks at 24-48 hours, then declines if treated appropriately
Clinical Imaging
Imaging Gallery


Critical Rhabdomyolysis Exam Points
Myoglobinuria is Key Sign
Dark tea-colored or cola-colored urine indicates myoglobinuria - this is the clinical sign of significant rhabdomyolysis. Requires immediate aggressive fluid resuscitation to prevent acute kidney injury from myoglobin tubular obstruction.
CK Threshold
CK over 10,000 U/L is diagnostic threshold. Levels can exceed 100,000 in severe cases. CK peaks at 24-48 hours after injury, then declines if treated. Monitor serial levels.
Acute Kidney Injury Prevention
Aggressive IV fluids target urine output over 200ml/hr (4-6L first 24 hours). Alkalinize urine with sodium bicarbonate (target pH over 6.5) to prevent myoglobin precipitation in renal tubules. This is the key to preventing AKI.
Hyperkalemia Risk
Hyperkalemia from massive muscle necrosis can cause cardiac arrhythmias and arrest. Monitor potassium levels and ECG. May require calcium, insulin/glucose, or dialysis. Life-threatening complication.
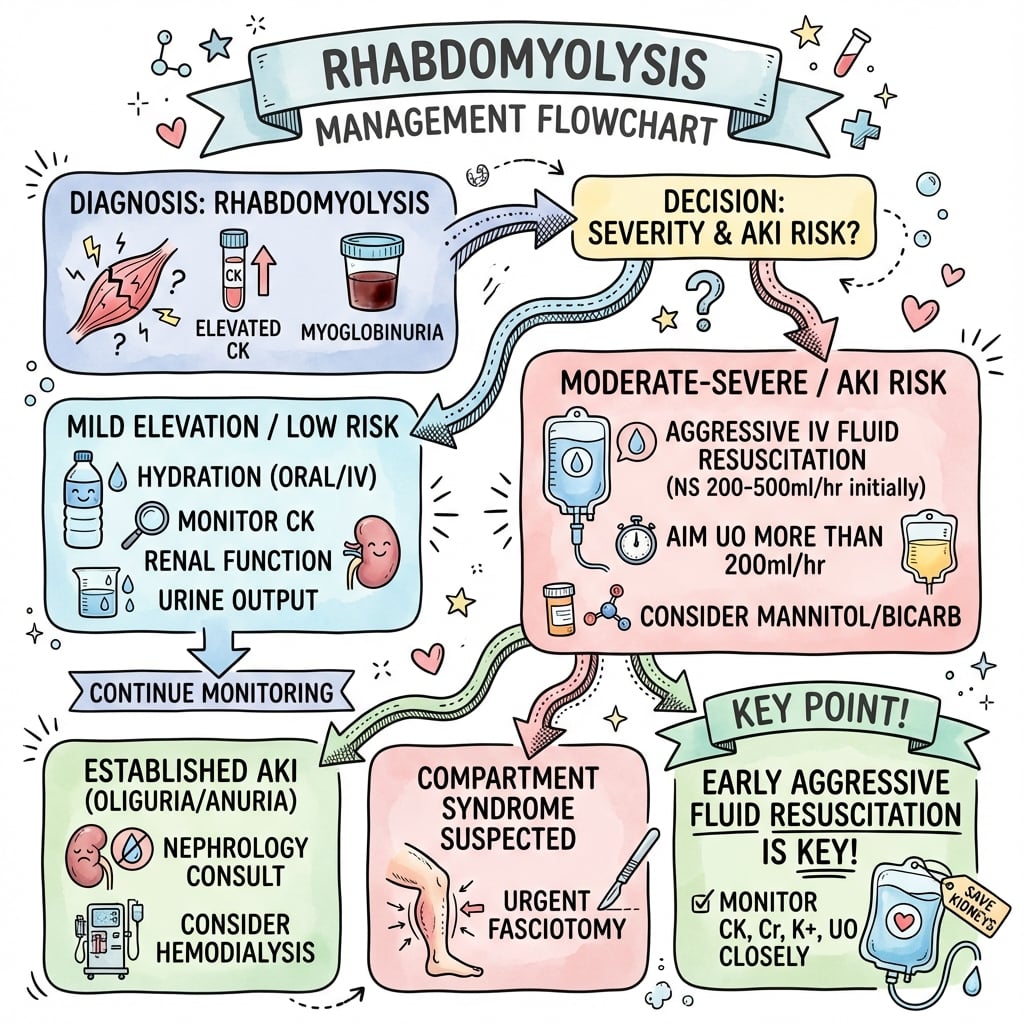
Rhabdomyolysis Management by Severity - Quick Reference
| CK Level | Myoglobinuria | Urine Output | Management |
|---|---|---|---|
| 5,000-10,000 | Absent | Normal | IV fluids, monitor CK |
| 10,000-50,000 | Present | Target 200ml/hr | Aggressive fluids, alkalinize urine |
| Over 50,000 | Severe | Over 200ml/hr | ICU, consider dialysis |
FARMRhabdomyolysis Management
| F | Fluids aggressive Target urine output over 200ml/hr (4-6L first 24h) |
| A | Alkalinize urine Sodium bicarbonate to pH over 6.5 |
| R | Renal protection Prevent myoglobin tubular obstruction |
| M | Monitor CK/K/ECG Serial CK, potassium, ECG for hyperkalemia |
| F | Fluids aggressive Target urine output over 200ml/hr (4-6L first 24h) | R | Renal protection Prevent myoglobin tubular obstruction |
| A | Alkalinize urine Sodium bicarbonate to pH over 6.5 | M | Monitor CK/K/ECG Serial CK, potassium, ECG for hyperkalemia |
Hook:FARM the patient: Fluids Aggressive, Alkalinize urine, Renal protection, Monitor closely!
CRUSHRhabdomyolysis Causes
| C | Compartment syndrome Most common orthopaedic cause |
| R | Rhabdomyolysis Muscle breakdown from ischemia |
| U | Unconscious (prolonged) Pressure necrosis from immobility |
| S | Seizures Muscle damage from convulsions |
| H | Heat stroke/exertion Exercise-induced muscle breakdown |
| C | Compartment syndrome Most common orthopaedic cause | S | Seizures Muscle damage from convulsions |
| R | Rhabdomyolysis Muscle breakdown from ischemia | H | Heat stroke/exertion Exercise-induced muscle breakdown |
| U | Unconscious (prolonged) Pressure necrosis from immobility |
Hook:CRUSH causes: Compartment syndrome, Rhabdomyolysis, Unconscious, Seizures, Heat stroke!
BICARBMyoglobinuria Management
| B | Bicarbonate (sodium) Alkalinize urine to pH over 6.5 |
| I | IV fluids aggressive 4-6L first 24 hours |
| C | CK monitoring Serial levels every 6-12 hours |
| A | Avoid nephrotoxins No NSAIDs, contrast if possible |
| R | Renal function Monitor creatinine, eGFR |
| B | Bicarbonate target pH Urine pH over 6.5 prevents precipitation |
| B | Bicarbonate (sodium) Alkalinize urine to pH over 6.5 | C | CK monitoring Serial levels every 6-12 hours | R | Renal function Monitor creatinine, eGFR |
| I | IV fluids aggressive 4-6L first 24 hours | A | Avoid nephrotoxins No NSAIDs, contrast if possible | B | Bicarbonate target pH Urine pH over 6.5 prevents precipitation |
Hook:BICARB: Bicarbonate, IV fluids, CK monitoring, Avoid nephrotoxins, Renal function, Bicarbonate target!
Overview and Epidemiology
Rhabdomyolysis is a syndrome of skeletal muscle breakdown with release of intracellular contents into the circulation, leading to myoglobinuria and potential acute kidney injury. It is a serious complication of compartment syndrome, crush injuries, and other muscle-damaging conditions.
Epidemiology:
- Common complication of compartment syndrome (especially if delayed over 6 hours)
- Crush injuries (earthquakes, building collapse)
- Prolonged immobility (unconscious patients)
- Exercise-induced (exertional rhabdomyolysis)
- Drug-induced (statins, alcohol)
- Heat-related illness
Mechanism of Muscle Breakdown:
Compartment Syndrome Connection
Compartment syndrome is the most common orthopaedic cause of rhabdomyolysis. When compartment syndrome is delayed (over 6 hours), muscle necrosis occurs, releasing myoglobin. This is why post-fasciotomy monitoring for rhabdomyolysis is essential.
Anatomy and Pathophysiology
Muscle Anatomy:
- Skeletal muscle contains high concentrations of CK and myoglobin
- Myoglobin is an oxygen-binding protein in muscle
- Muscle cell membrane disruption releases these into circulation
- Renal tubules filter myoglobin, which can precipitate
Renal Anatomy:
- Glomeruli filter myoglobin from blood
- Renal tubules are where myoglobin precipitates
- Acidic urine (pH under 5.6) promotes precipitation
- Tubular obstruction leads to decreased GFR and AKI
Final common pathway: Whatever the trigger (direct trauma, ischaemia, metabolic, toxic), the end result is an uncontrolled rise in intracellular calcium. ATP depletion impairs the Na+/K+ and Ca2+ ATPase pumps, calcium floods the myocyte, activating proteases and phospholipases that destroy the sarcolemma. Membrane rupture releases creatine kinase, myoglobin, potassium, phosphate, urate and purines into the circulation, while extracellular fluid and calcium are sequestered into damaged muscle (third-spacing causing hypovolaemia and early hypocalcaemia).
Three mechanisms of myoglobinuric AKI (all favoured by hypovolaemia and aciduria):
- Renal vasoconstriction / ischaemia - hypovolaemia plus scavenging of nitric oxide by myoglobin reduces medullary blood flow
- Intratubular cast formation - myoglobin precipitates with Tamm-Horsfall protein, especially in acidic urine (pH under 5.6), obstructing distal tubules
- Direct heme-mediated tubular toxicity - iron-catalysed lipid peroxidation and free-radical injury of proximal tubular cells
Rhabdomyolysis: From Muscle to Kidney
| Stage | Process | Consequence |
|---|---|---|
| Injury | Sarcolemma rupture, calcium influx, protease activation | Release of intracellular contents |
| Circulation | CK, myoglobin, K+, PO4, urate enter blood; fluid sequestered in muscle | Rising serum markers + hypovolaemia |
| Kidney | Myoglobin filtered, casts form, heme toxicity, vasoconstriction | Tubular obstruction + ischaemia |
| AKI | Acute tubular necrosis, falling GFR | Acute kidney injury, hyperkalaemia |
Classification Systems
Rhabdomyolysis Severity
Severity Classification by CK Level
| Severity | CK Level | Myoglobinuria | Management |
|---|---|---|---|
| Mild | 5,000-10,000 U/L | Absent | IV fluids, monitor |
| Moderate | 10,000-50,000 U/L | Present | Aggressive fluids, alkalinize urine |
| Severe | Over 50,000 U/L | Severe | ICU, dialysis if needed |
Mild: Usually resolves with simple hydration. Monitor CK levels.
Moderate: Requires aggressive management to prevent AKI. Most common presentation.
Severe: Life-threatening, requires ICU care. High risk of AKI and hyperkalemia.
Clinical Assessment
History:
- Compartment syndrome (most common orthopaedic cause)
- Crush injury (prolonged compression)
- Prolonged immobility (unconscious patient)
- Exercise-induced (exertional)
- Drug history (statins, alcohol)
- Heat exposure
Physical Examination:
Muscle Findings
- Swollen, tender muscles
- Weakness
- Myalgia
- Compartment syndrome signs (if present)
Systemic Signs
- Dark tea-colored urine (myoglobinuria)
- Decreased urine output
- Signs of hyperkalemia (ECG changes)
- Signs of AKI (oliguria, fluid overload)
Urine Assessment:
- Color: Dark tea-colored or cola-colored = myoglobinuria
- Dipstick: Positive for blood (but no RBCs on microscopy) = myoglobin
- Output: Decreased output indicates AKI developing
Myoglobinuria Recognition
Dark tea-colored or cola-colored urine is the clinical hallmark of myoglobinuria. Dipstick will be positive for blood, but microscopy shows no red blood cells (myoglobin, not hemoglobin). This requires immediate aggressive management.
Differential Diagnosis
The "blood-positive dipstick with no red cells" picture and dark urine have a short, high-yield differential. The key discriminator is serum CK and the urine microscopy.
Differential Diagnosis of Dark Urine / Raised CK
| Condition | Distinguishing Feature | Serum CK | Urine Microscopy / Dipstick |
|---|---|---|---|
| Rhabdomyolysis (myoglobinuria) | Muscle pain/weakness, swelling, recent crush/exertion | Markedly raised (over 5x normal) | Dipstick blood positive, NO red cells; pigmented granular casts |
| Haemoglobinuria (haemolysis) | Anaemia, raised LDH/bilirubin, low haptoglobin; pink plasma | Normal | Dipstick blood positive, no red cells; plasma pink (myoglobin clears, Hb stains plasma) |
| Haematuria | Renal/urological cause, clots | Normal | Dipstick blood positive WITH red cells on microscopy |
| Myocardial / cardiac CK rise | Chest pain, no myalgia | Raised but CK-MB fraction high, troponin positive | Urine clear, dipstick negative |
| Inflammatory myopathy (polymyositis) | Subacute proximal weakness, autoantibodies | Moderately raised, fluctuating | Usually clear urine |
| Beeturia / drug discolouration (rifampicin) | Dietary/drug history | Normal | Dipstick blood NEGATIVE |
Investigations
Laboratory Tests:
Essential Laboratory Tests
| Test | Finding | Significance |
|---|---|---|
| CK (creatine kinase) | Over 10,000 U/L (diagnostic) | Peaks 24-48h, then declines |
| Myoglobin (serum) | Elevated | Confirms muscle breakdown |
| Myoglobin (urine) | Positive | Dark urine, tubular obstruction risk |
| Potassium | Hyperkalemia | Cardiac risk - monitor ECG |
| Creatinine | Rising | AKI developing |
| Phosphate | Elevated | Muscle breakdown |
| Calcium | Hypocalcemia early | Precipitates in necrotic muscle |
Monitoring Protocol:
Laboratory Monitoring
- CK, myoglobin (serum and urine)
- UEC (potassium, creatinine, urea)
- FBC, coagulation
- ECG (hyperkalemia assessment)
- CK levels (peak at 24-48h)
- Potassium (hyperkalemia risk)
- Creatinine (AKI progression)
- Urine output monitoring
- CK declining
- Renal function improving
- Potassium normalized
CK Kinetics
CK peaks at 24-48 hours after injury, then declines with half-life of 1.5 days if treated appropriately. If CK continues rising after 48 hours, ongoing muscle damage is occurring (incomplete fasciotomy, recurrent compartment syndrome, or other cause).
Urinary Sediment Findings
Management Algorithm
CK 5,000-10,000, No Myoglobinuria
Management:
- IV fluids: 1-2L over 24 hours
- Monitor CK levels
- Monitor urine output
- Usually resolves without complications
Prognosis: Excellent with simple hydration.
Surgical Technique
Note: Rhabdomyolysis itself is a medical condition, not a surgical procedure. However, if compartment syndrome is the underlying cause, fasciotomy is required. This section addresses fasciotomy technique when rhabdomyolysis is present or suspected.
Fasciotomy Technique (When Rhabdomyolysis Present)
Pre-operative Considerations:
- Rhabdomyolysis may already be present if delayed over 6 hours
- Monitor for myoglobinuria post-operatively
- Plan for aggressive fluid resuscitation
- Consider ICU admission if severe
Technique:
- Standard fasciotomy approach (leg: 2-incision, 4-compartment)
- Release all compartments completely
- Assess muscle viability (pink, contractile = viable; dark, non-contractile = necrotic)
- Debride obviously necrotic muscle
- Leave wounds open
Post-operative:
- Immediate aggressive fluid resuscitation
- Monitor for rhabdomyolysis
- Serial CK levels
- Urine output monitoring
Fasciotomy prevents further muscle necrosis and may limit rhabdomyolysis progression.
Treatment Details
Aggressive IV Fluid Therapy
Goal: Maintain urine output over 200ml/hr (or over 1ml/kg/hr)
Protocol:
- Initial: 1-2L bolus if dehydrated
- Maintenance: 4-6L over first 24 hours
- Type: Normal saline or lactated Ringer's
- Monitoring: Hourly urine output, daily weights, clinical assessment
Rationale:
- High urine flow prevents myoglobin precipitation
- Maintains renal perfusion
- Prevents tubular obstruction
Fluid Target
Target urine output over 200ml/hr (or over 1ml/kg/hr) is essential to prevent myoglobin tubular obstruction. This requires aggressive IV fluid administration - 4-6L in first 24 hours is common.
Complications
Rhabdomyolysis Complications
| Complication | Incidence | Management |
|---|---|---|
| Acute kidney injury | 30-50% if untreated | Prevent with aggressive fluids, alkalinization |
| Hyperkalemia | Common in severe cases | Monitor ECG, treat with calcium/insulin/bicarb |
| Hypocalcemia (early) | Common | Usually resolves, avoid overcorrection |
| Hypercalcemia (late) | During recovery | Calcium released from necrotic muscle |
| Compartment syndrome | If underlying cause | Fasciotomy if present |
| DIC | Rare | Supportive care |
Acute Kidney Injury:
- Most serious complication
- Develops in 30-50% if untreated
- Prevention is key: aggressive fluids, urine alkalinization
- Most recover renal function with treatment
- May require temporary dialysis
Hyperkalemia:
- Life-threatening complication
- Can cause cardiac arrest
- Requires immediate treatment
- Monitor ECG continuously
AKI Recovery
Most patients with rhabdomyolysis-induced AKI recover renal function with appropriate treatment. Dialysis is often temporary. Long-term renal impairment is uncommon if treated early and aggressively.
Postoperative Care
After Fasciotomy (if compartment syndrome cause):
Post-Fasciotomy Rhabdomyolysis Management
- Aggressive IV fluids (target 200ml/hr urine output)
- Alkalinize urine (sodium bicarbonate)
- Monitor CK, potassium, creatinine
- ECG monitoring
- Continue aggressive fluids
- Serial CK every 6-12 hours
- Monitor urine output hourly
- Assess for hyperkalemia
- Consider ICU if severe
- CK should peak then decline
- Continue monitoring
- Assess renal function
- Wean fluids as CK normalizes
- CK declining
- Renal function improving
- Can reduce monitoring frequency
- Continue until CK under 5,000
Key Monitoring:
- Urine output (target over 200ml/hr)
- Urine color (should lighten as myoglobinuria resolves)
- CK levels (should decline after 24-48h peak)
- Potassium (hyperkalemia risk)
- Creatinine (AKI progression)
Outcomes and Prognosis
Recovery:
- CK normalization: 3-5 days with treatment
- Renal function: Most recover completely
- Mortality: Low if treated appropriately (under 5%)
- Long-term: Usually no sequelae if treated early
Prognostic Factors:
- Early treatment: Better outcomes
- CK level: Higher CK = worse prognosis
- Time to treatment: Delayed treatment = higher AKI risk
- Underlying cause: Treatable causes (compartment syndrome) have better outcomes
Evidence Base
Rhabdomyolysis and Acute Kidney Injury
- Definitive modern review of pathophysiology and management
- Myoglobin causes AKI via tubular cast obstruction, direct heme toxicity and renal vasoconstriction
- Early, aggressive volume expansion is the cornerstone of AKI prevention
- Evidence for routine bicarbonate and mannitol beyond saline is weak
Compartment Monitoring in Tibial Fractures: The Pressure Threshold for Decompression
- Prospective study of 116 tibial diaphyseal fractures with continuous compartment monitoring
- Acute compartment syndrome occurred in 3 patients (2.6%)
- A differential pressure (diastolic minus compartment pressure) under 30 mmHg missed no cases
- Absolute thresholds of 30 or 40 mmHg would have led to many unnecessary fasciotomies
Early Management of Shock and Prophylaxis of Acute Renal Failure in Traumatic Rhabdomyolysis
- Foundational protocol for crush/traumatic rhabdomyolysis
- Early, vigorous volume loading begun before or during extrication prevents oliguric ARF
- Mannitol-alkaline diuresis proposed to reduce cast formation and tubular toxicity
- Hypovolaemia and aciduria are the key drivers of renal injury
Early Fluid Resuscitation in Patients with Rhabdomyolysis
- Early vigorous fluid resuscitation (up to 12 L/day alkaline fluid) can prevent myoglobinuric AKI
- Resuscitation started at the scene mobilises sequestered fluid and corrects hyperkalaemia and acidosis
- In crush syndrome, mortality has fallen from nearly 100% to under 20% over 70 years
- A large positive fluid balance is tolerated in young, monitored patients
Rhabdomyolysis and Myohemoglobinuric Acute Renal Failure
- Classic mechanistic review of myoglobinuric AKI
- Heme proteins precipitate with Tamm-Horsfall protein, favoured by acidic urine
- Iron-catalysed lipid peroxidation drives direct tubular toxicity
- Volume expansion and urinary alkalinisation are rational, mechanism-based interventions
Preventing Renal Failure in Rhabdomyolysis: Do Bicarbonate and Mannitol Make a Difference?
- Review of 2,083 trauma ICU admissions; 85% had abnormal CK
- CK over 5,000 U/L was associated with renal failure (19% vs 8%, p under 0.0001)
- Bicarbonate/mannitol did NOT reduce renal failure, dialysis or mortality
- Authors called for re-evaluation of routine bicarbonate/mannitol use
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Post-Fasciotomy Rhabdomyolysis
"A 35-year-old man underwent fasciotomy for compartment syndrome 12 hours after injury. Post-operatively, his urine is dark tea-colored, CK is 25,000 U/L, and creatinine is rising. How do you manage this?"
Scenario 2: Crush Injury Rhabdomyolysis
"A 45-year-old construction worker is extracted from a building collapse after 8 hours. He has a crushed leg, is hypotensive, and his urine is dark. CK is 75,000 U/L, potassium is 6.8mmol/L, and ECG shows peaked T-waves. Describe your immediate management."
Scenario 3: Delayed Recognition
"A 28-year-old athlete presents 48 hours after a marathon with severe muscle pain, weakness, and dark urine. CK is 45,000 U/L, creatinine is 250 micromol/L, and urine output is 30ml/hr. How do you manage this?"
MCQ Practice Points
CK Threshold Question
Q: What is the diagnostic threshold for rhabdomyolysis? A: CK over 10,000 U/L - this is the widely accepted diagnostic threshold. Levels can exceed 100,000 in severe cases. CK peaks at 24-48 hours after injury, then declines if treated appropriately.
Myoglobinuria Question
Q: What is the clinical sign of myoglobinuria? A: Dark tea-colored or cola-colored urine - this indicates significant myoglobin release from muscle breakdown. Dipstick will be positive for blood, but microscopy shows no red blood cells (myoglobin, not hemoglobin).
Urine Output Target Question
Q: What is the target urine output for rhabdomyolysis management? A: Over 200ml/hr (or over 1ml/kg/hr) - this high urine flow prevents myoglobin precipitation in renal tubules and maintains renal perfusion. Requires aggressive IV fluid administration (4-6L first 24 hours).
Urine Alkalinization Question
Q: Why is urine alkalinization important in rhabdomyolysis? A: Myoglobin precipitates in acidic urine (pH under 5.6), causing tubular obstruction and AKI. Alkaline urine (pH over 6.5) prevents precipitation. Sodium bicarbonate is added to IV fluids to maintain urine pH over 6.5.
Hyperkalemia Question
Q: Why does rhabdomyolysis cause hyperkalemia? A: Massive muscle necrosis releases intracellular potassium into circulation. This can cause life-threatening hyperkalemia with cardiac arrhythmias. Requires immediate treatment (calcium, insulin/glucose, bicarbonate) and may need dialysis.
Controversies and Areas of Uncertainty
Much of "classic" rhabdomyolysis management is based on physiology and observational data rather than randomised trials. The exam-relevant debates are:
Areas of Genuine Uncertainty
| Question | Where the evidence sits |
|---|---|
| Bicarbonate vs saline alone | No RCT shows bicarbonate-alkaline diuresis is superior to adequate isotonic saline. Brown et al (J Trauma 2004) found no benefit of bicarbonate/mannitol on renal failure, dialysis or mortality. Most guidelines now favour volume first, bicarbonate optional. |
| Routine mannitol | Theoretical osmotic diuretic and free-radical scavenger benefit is unproven; risks volume depletion and hyperosmolality. Avoid in oliguria/established AKI. Not supported by trial data. |
| CK threshold for 'rhabdomyolysis' | No universal cutoff. Commonly CK over 5x upper limit of normal (~1,000 U/L) defines the syndrome, while AKI risk rises sharply above ~5,000 U/L and especially over 15,000-40,000 U/L. The '10,000' figure is a pragmatic teaching threshold, not an absolute rule. |
| Target urine output | 100-300 ml/hr is variously quoted; ~200-300 ml/hr (or 3 ml/kg/hr) is typical, but the real goal is brisk flow without precipitating fluid overload. |
| Early vs late renal replacement therapy | RRT is for standard indications (refractory hyperkalaemia, acidosis, fluid overload, uraemia). 'Prophylactic' high-flux dialysis to clear myoglobin is not evidence-based for routine use. |
The single highest-yield message
If you remember one thing for the viva: volume, volume, volume. Early, adequate isotonic fluid resuscitation prevents AKI; bicarbonate and mannitol are adjuncts of unproven incremental benefit and must never delay or substitute for fluids.
Guidelines, Registries & Global Practice
Global epidemiology:
- Crush-related rhabdomyolysis follows mass-casualty events: earthquakes are the archetype (Marmara/Turkey 1999, Wenchuan/China 2008, Haiti 2010, Kahramanmaras/Turkey 2023), where it is a leading cause of preventable post-event death after head injury.
- Non-traumatic causes (statins/drugs, exertion, alcohol, immobility, infection, inherited metabolic myopathies) dominate in routine hospital practice worldwide.
- Acute kidney injury complicates roughly 10-50% of significant rhabdomyolysis depending on cause and resuscitation timing; with early aggressive fluids, AKI and dialysis dependence fall substantially.
Guidelines side by side (where emphasis genuinely differs):
Major Guidance on Rhabdomyolysis / Crush Injury
| Source | Emphasis |
|---|---|
| ISN / Renal Disaster Relief Task Force | Crush-syndrome focus: start IV isotonic saline before/at extrication; large volumes (up to ~6-12 L/day) with close monitoring; alkalinisation optional |
| AO Foundation / orthopaedic trauma | Recognise and decompress acute compartment syndrome early (delta-P under 30 mmHg); fasciotomy limits ongoing muscle necrosis and myoglobin load |
| KDIGO (AKI) | General AKI principles: volume optimisation, avoid nephrotoxins, treat hyperkalaemia, RRT for standard indications |
| IOC / sports medicine (exertional) | Exertional rhabdomyolysis: rest, hydration, screen for recurrent/atypical cases and inherited metabolic myopathy before return to sport |
High- vs limited-resource practice variation:
- High-resource: point-of-care CK and electrolytes, continuous ECG, ICU-level monitoring, and ready access to haemodialysis/CRRT for refractory AKI.
- Limited-resource / disaster settings: the decisive intervention is early oral and IV fluid; dialysis capacity is the rate-limiting step. International nephrology task forces pre-position dialysis support after earthquakes precisely because crush AKI overwhelms local capacity.
Avoid the classic pitfalls
The preventable harms are the same everywhere: missed/late acute compartment syndrome, under-resuscitation, failure to detect rising potassium, and continued nephrotoxin exposure (NSAIDs, contrast). Early fluids and serial CK/potassium/creatinine address all four.
RHABDOMYOLYSIS
Clinical summary
Key Facts
- •CK over 10,000 U/L is diagnostic threshold
- •Dark tea-colored urine = myoglobinuria
- •Compartment syndrome is most common orthopaedic cause
- •CK peaks at 24-48 hours, then declines
Management (FARM)
- •Fluids Aggressive: Target 200ml/hr urine output (4-6L first 24h)
- •Alkalinize urine: Sodium bicarbonate to pH over 6.5
- •Renal protection: Prevent myoglobin tubular obstruction
- •Monitor: CK, potassium, creatinine, ECG
Hyperkalemia Treatment
- •IV Calcium (cardioprotective, stabilizes membrane)
- •Insulin/Glucose (drives K+ into cells)
- •Sodium Bicarbonate (alkalinizes, shifts K+)
- •Dialysis if refractory or severe
Complications
- •Acute kidney injury: 30-50% if untreated
- •Hyperkalemia: Life-threatening, cardiac risk
- •Hypocalcemia early, hypercalcemia late
- •Most recover with appropriate treatment