Traction Degloving of the Finger - Classify, then Decide
- A ring avulsion injury occurs when a RING catches on a fixed object and the body weight/momentum applies a sudden TRACTION force, DEGLOVING the soft-tissue envelope of the finger circumferentially off the skeleton - the skin, neurovascular bundles and tendons are torn over a LONG segment even when the skin looks deceptively intact.
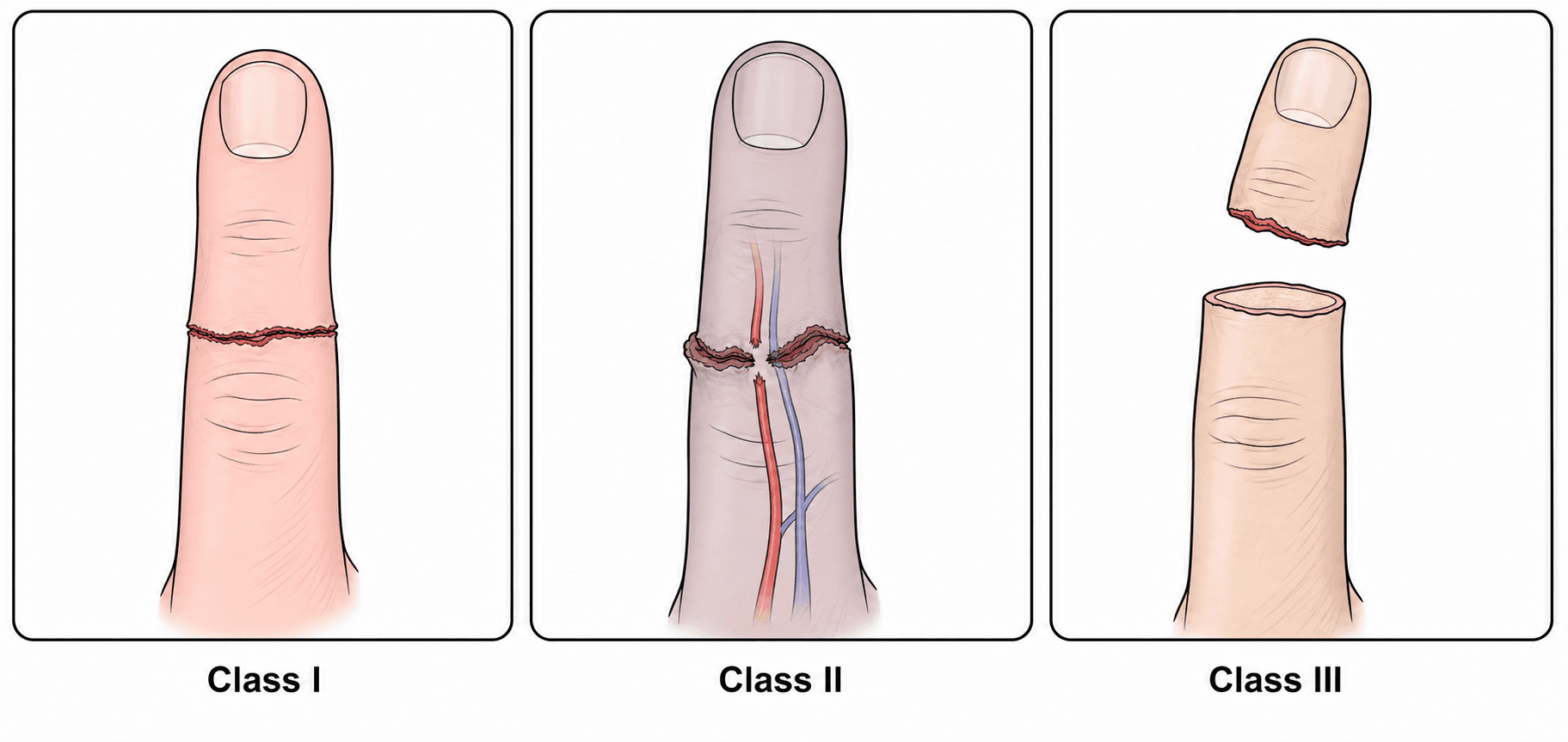
- It is classified by the URBANIAK system: Class I = adequate circulation (soft-tissue injury only); Class II = inadequate circulation needing microvascular repair; Class III = complete degloving or complete amputation. The KAY modification subdivides class II into arterial (IIa) and venous (IIv) and adds a class for bone/joint injury and a class IV for complete amputation.
- A crucial principle is that the ZONE OF VASCULAR INJURY is FAR MORE EXTENSIVE than it appears - the avulsed vessels are stretched and damaged well beyond the obvious wound - so successful revascularisation/replantation requires AGGRESSIVE debridement of the damaged vessel back to healthy ends and INTERPOSITION VEIN GRAFTS rather than direct end-to-end repair under tension.
- PROGNOSIS depends heavily on the level and structures: an INTACT PROXIMAL INTERPHALANGEAL (PIP) JOINT and an intact FLEXOR DIGITORUM SUPERFICIALIS (FDS) - typical when the avulsion disrupts the bone distally (around the DIP) while the PIP/FDS are spared - predict a much better functional result; outcomes (total active motion, two-point discrimination) are best for class I and II.
- MANAGEMENT by class: Class I - treat the bone/soft tissue, no vessel repair; Class II - urgent microvascular REVASCULARISATION (artery +/- vein, with vein grafts); Class III/complete amputation - the historical default was COMPLETION AMPUTATION, but evidence shows SELECTED severe injuries (especially with an intact PIP/FDS) can be successfully REPLANTED, so the decision is individualised.
- PRESERVE THE PART CORRECTLY or the reconstruction is foreclosed before the hand surgeon sees it: wrap in SALINE-MOISTENED GAUZE, seal in a plastic bag, place the bag in ICE WATER. Never directly on ice and NEVER dry ice (freezes the tissue), never left soaking (macerates), and never transported separately - the part travels with the patient. Give tetanus prophylaxis and antibiotics, radiograph hand and part, and keep the patient nil by mouth.
- ISCHAEMIA TIMES for a digit are generous because a finger contains NO MUSCLE: about 6 hours WARM and 12 hours COLD, with success reported at 24-30 hours cold in some series - so a delayed presentation is not by itself a reason to abandon a finger. The more PROXIMAL the level the SHORTER the window (hand about 4-6 hours warm, forearm/arm under about 4), because muscle is the limiting tissue and its reperfusion risks hyperkalaemia, acidosis and myoglobinuric renal injury.
- The repair sequence is BEFANV - Bone, Extensor, Flexor, Artery, Nerve, Vein - shortening bone as needed so no repair is under tension, and anastomosing TWO VEINS for every artery with the skin closed LOOSELY so the closure does not strangle the outflow. An avulsion modifies this because the DORSAL VEINS are stripped over the same long segment as the arteries, so VEIN GRAFTS are frequently needed on the VENOUS side too - not only on the artery, which is how the requirement is usually remembered.
- MONITORING is a defined observation, not a general instruction: colour, capillary refill, pulp turgor, temperature and Doppler HOURLY for 24-48 hours, then 2-4 hourly, with a temperature difference above 2 degrees from an adjacent digit as a useful adjunct. A PALE, cool digit with no Doppler signal is ARTERIAL occlusion; a BLUE, tense digit with brisk refill bleeding dark blood is VENOUS CONGESTION - the commoner problem, and especially after avulsion. Salvage by loosening dressings/sutures, then LEECHES or nail-plate removal with heparin-soaked gauze (cover leeches against Aeromonas hydrophila), with a low threshold to re-explore.
- The replant-versus-amputate decision is SHARED with the patient and weighs hand dominance, occupation/manual demands, which digit (a stiff or insensate single border/index finger may impair overall hand function), ischaemia time, contamination, smoking and the patient's wishes - a well-functioning amputation/revision may outperform a stiff, insensate, painful salvaged digit.
- “Urbaniak: I = circulation adequate (soft tissue); II = inadequate (revascularise, +/- vein grafts); III = complete degloving/amputation. Kay adds IIa/IIv and class IV (complete amputation).
- “Zone of vessel injury is LONGER than it looks -> debride back to healthy vessel + interposition VEIN GRAFTS (no tension).
- “Intact PIP joint + FDS = better prognosis; class III replant possible in selected cases but completion amputation is often appropriate - shared decision.
- “Preserve the part: saline-moistened gauze -> sealed bag -> ICE WATER. Never on ice directly, never dry ice, never soaking, never travelling separately from the patient.
- “Digit ischaemia (no muscle): ~6 h warm, ~12 h cold, sometimes 24-30 h cold. Proximal levels are far tighter - muscle is the limiting tissue.
- “BEFANV sequence; TWO veins per artery; close skin loosely. Avulsion strips the VEINS as well, so vein grafts are often needed on both sides.
- “Monitor hourly x 24-48 h (colour, refill, turgor, temp, Doppler). PALE = arterial; BLUE and tense = venous congestion -> loosen, leeches or nail-plate heparin gauze, re-explore early.
The visible wound may be a simple circumferential laceration, but the traction has stretched and torn the arteries, veins and nerves over a long segment.
Debride the damaged vessel back to healthy intima and bridge the gap with interposition vein grafts - a tension-free anastomosis - rather than forcing a direct repair.
Mechanism & Classification
A ring snags on a hook, fence or machinery as the person falls or jumps; the ring transmits a sudden axial traction to the finger, degloving the soft-tissue sleeve from the bone. Depending on the force, this ranges from a circumferential soft-tissue injury with preserved perfusion, through circulatory compromise (artery and/or vein avulsed), to complete degloving ('squirrel-cage'/'glove' avulsion) or frank amputation. The bone often fails distally (around the DIP) while the PIP joint and FDS insertion remain - an important prognostic point. The injury is graded by the Urbaniak classification (with the Kay modification) to guide treatment.
- Circulation
- Adequate
- Treatment
- Bone/soft-tissue care; NO vessel repair
- Outcome
- Best (good TAM, sensation)
- Circulation
- Inadequate (artery +/- vein)
- Treatment
- Microvascular revascularisation (+/- vein grafts)
- Outcome
- Good with revascularisation
- Circulation
- Complete degloving / amputation
- Treatment
- Replantation in SELECTED cases vs completion amputation
- Outcome
- Variable; select replants do well (intact PIP/FDS)
First Contact: the Digit, the Part and the Clock
Preserving an Amputated or Devascularised Part
Getting this wrong at the referring hospital forecloses the reconstruction before the hand surgeon sees the patient, and it is asked in vivas precisely because it is so often done badly.
- Wrap the part in saline-moistened gauze.
- Seal it in a plastic bag.
- Place the sealed bag in ice water.
Three things must not happen: the part must not touch ice directly and never dry ice, which freezes and destroys the tissue; it must not be left soaking in water or saline, which macerates it; and it must not travel separately - the part and the patient are transferred together to the replantation centre. Alongside this, resuscitate and assess for other injuries, give tetanus prophylaxis and antibiotics, radiograph the hand and the amputated part, keep the patient nil by mouth, and photograph the injury before dressing it.
The Ischaemia Clock
A digit contains no muscle bulk, which is why it tolerates ischaemia far better than an amputation through the palm or forearm - and why a delayed presentation is not by itself a reason to abandon a finger.
- Warm ischaemia
- Up to about 6 hours
- Cold ischaemia
- Up to about 12 hours, with success reported at 24-30 hours in some series
- Why
- Skin, tendon and bone tolerate ischaemia; there is no muscle to necrose
- Warm ischaemia
- About 4-6 hours
- Cold ischaemia
- Shorter than for a digit
- Why
- Intrinsic muscle is the limiting tissue and dictates the window
- Warm ischaemia
- Under about 4 hours
- Cold ischaemia
- Shortest of all
- Why
- Large muscle mass - reperfusion risks hyperkalaemia, acidosis and myoglobinuric renal injury
For a digit, warm ischaemia up to about 6 hours and cold up to about 12 hours (occasionally much longer), because a finger has no muscle. The more proximal the level, the shorter the window - muscle is the limiting tissue. Preserve the part in saline-moistened gauze, sealed bag, ice water - never directly on ice, never dry ice, never soaking, and never travelling separately from the patient.
The Full Kay Classification (and Why the FDS Level Matters)
- Class I. Circulation adequate (with or without skeletal injury) - soft-tissue/bone care only.
- Class II. Inadequate circulation without bone/joint injury - subdivided IIa (arterial inadequate) and IIv (venous inadequate); needs microvascular repair.
- Class III. Inadequate circulation WITH an associated fracture or joint injury (likewise subdivided by arterial vs venous compromise) - a more severe, less favourable group.
- Class IV. Complete amputation, subdivided by the level relative to the flexor digitorum superficialis (FDS) insertion: amputation distal to the FDS insertion (the FDS preserved) carries a far better functional prognosis than amputation proximal to it. This FDS-level split is the prognostic heart of the classification.
Full Kay: I adequate; II inadequate circulation without bone injury (IIa artery / IIv vein); III inadequate circulation with bone/joint injury; IV complete amputation, split by the FDS insertion level (distal-to-FDS = FDS preserved = much better than proximal-to-FDS). The added value over Urbaniak is flagging bone injury (III) and the FDS-level (IV) - both prognostic.
Management & Decision-Making
- Class I: clean and repair the soft tissue, fix any fracture, repair tendons/nerves as needed - no microvascular repair required.
- Class II: urgent microvascular revascularisation of the artery (and vein where needed) - because of the extended injury, debride vessels to healthy ends and use interposition VEIN GRAFTS; repair nerves and provide soft-tissue cover (flap/graft) as required.
- Class III / complete amputation: weigh replantation against completion amputation. Replantation is more worthwhile when the PIP joint and FDS are intact, the digit is clean, ischaemia time is acceptable, and the patient accepts a long rehabilitation; otherwise a well-fashioned completion (revision) amputation restores quick, reliable function. Severe contamination, prolonged warm ischaemia, heavy smoking, and a single insensate border/index digit favour amputation.
- The decision is shared with the patient, considering hand dominance, occupation, the specific digit, cosmetic wishes and rehabilitation capacity.
Even when a class III digit is successfully replanted, the damaged vessels can fail late: series report late arterial thrombosis weeks after surgery. Replanted ring-avulsion digits therefore need careful postoperative monitoring, smoking cessation, and a low threshold for early re-exploration if perfusion deteriorates. Counsel patients that even a salvaged finger may end up stiff, cold-intolerant or partly insensate.
The Repair Sequence, and How Avulsion Changes It
The order of repair is the standard replantation sequence, BEFANV - Bone, Extensor, Flexor, Artery, Nerve, Vein - working from the stable platform outwards so that no later repair is made under tension. Bone is shortened as required to let the soft-tissue and vessel repairs sit tension-free. After about 10-15 minutes of arterial perfusion the dorsal veins engorge and become identifiable, and the aim is two veins for every artery repaired, with the skin closed loosely so the closure itself does not strangle the venous outflow.
An avulsion modifies this in three specific ways:
- Both sides of the circulation are avulsed, not just the artery. The dorsal veins are stripped over the same long segment as the digital arteries, so vein grafts are frequently needed on the venous side too - not only for the artery, which is how the requirement is usually remembered.
- Debride until the vessel is normal, then debride further. The intima is damaged well beyond the visibly injured segment, and the classic errors are resecting too little and then anastomosing damaged intima, or resecting adequately and then pulling the ends together under tension instead of grafting the gap.
- Tag every structure before repairing anything. In a degloved, retracted, blood-filled field the commonest cause of failure is a cut end that cannot be found again when it is needed.
Keeping It Alive: Monitoring and Salvage
Monitoring a replanted or revascularised digit is a defined observation, not a general instruction.
- What is observed: colour, capillary refill, pulp turgor, temperature and the Doppler signal - hourly for the first 24-48 hours, then every 2-4 hours. A temperature difference of more than 2 degrees from an adjacent normal digit is a useful adjunct, and an implantable Doppler probe gives continuous monitoring where available.
- Read the colour. A pale, cool digit with sluggish refill and no Doppler signal is arterial occlusion. A blue, swollen, tense digit with brisk refill that bleeds dark blood on pin-prick is venous congestion - the commoner early problem, and especially so after an avulsion because the venous repair is the more precarious one.
- Environment and drugs: keep the patient warm, well hydrated and pain-free (cold, hypovolaemia and pain all cause vasospasm), enforce absolute abstinence from nicotine and caffeine, elevate the hand, and give aspirin 75-150 mg daily for 2-4 weeks with thromboprophylaxis as indicated.
- Salvage the congested digit: loosen tight dressings and remove constricting sutures first, then medicinal leeches, or remove the nail plate and apply heparin-soaked gauze to encourage controlled bleeding - so-called chemical leeching. Patients on leech therapy need antibiotic cover against Aeromonas hydrophila and monitoring of haemoglobin.
- Have a low threshold to return to theatre. Deterioration that does not respond promptly to these measures is an indication to re-explore, and the salvage rate falls with every hour of delay. Ring avulsions carry the added risk of late arterial failure weeks after surgery, so the vigilance does not end with discharge.
Prognostic Factors and Functional Outcomes
- Favourable factors. An intact PIP joint and FDS (amputation distal to the FDS insertion), a lower Urbaniak/Kay class, a clean wound, short ischaemia, a non-smoker, and a patient able to commit to a long rehabilitation.
- Outcomes by class. Total active motion and two-point discrimination deteriorate progressively from class I to II to III (as in the cited systematic-review figures); even successful replants are commonly cold intolerant and may be partly insensate or stiff, and class III replants carry a risk of late arterial failure.
- When a revision amputation outperforms. A stiff, insensate, cold-intolerant salvaged digit - especially a single index or border finger - is often bypassed by the patient and can impair overall hand use, so a well-fashioned completion amputation giving quick, reliable, pain-free function may be the better functional result. The choice is shared and weighed against hand dominance, occupation and the specific digit.
Predictors of a good replant: intact PIP + FDS (distal-to-FDS amputation), low class, clean wound, short ischaemia, non-smoker, motivated patient. Counsel that even a survived digit is often cold-intolerant and may be stiff/insensate, with a class III risk of late arterial failure. A stiff, insensate single index/border digit is frequently bypassed - so a revision amputation can give the better functional result.
Mnemonics & Memory Aids
123
Hook:Urbaniak 1-2-3 = perfused, under-perfused, off (degloved/amputated).
GRAFT
Hook:In avulsion, you GRAFT - because the vessel injury is long.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A labourer catches his wedding ring on a fence jumping down and degloves his ring finger. How do you classify and manage this?”
“When would you favour completion amputation over replantation in a complete ring avulsion?”
Mechanism
- Ring catches -> axial traction -> circumferential degloving of soft-tissue sleeve
- Vessels/nerves/tendons torn over a LONG segment (skin appearance underestimates it)
- Bone often fails distally (DIP); PIP/FDS may be spared
Classification
- Urbaniak I: adequate circulation (soft tissue)
- Urbaniak II: inadequate circulation (Kay IIa artery / IIv vein) -> revascularise
- Urbaniak III: complete degloving/amputation (Kay class IV = complete amputation)
First contact
- Part: saline-moistened gauze -> sealed bag -> ice water (NOT on ice, NOT dry ice, NOT soaking)
- Part travels WITH the patient; tetanus + antibiotics; X-ray hand and part; nil by mouth
- Digit ischaemia: ~6 h warm, ~12 h cold (24-30 h cold reported) - no muscle in a finger
- Hand ~4-6 h warm, forearm/arm under ~4 h - muscle is the limiting tissue
Treatment
- I: bone/soft tissue, no vessel repair | II: microvascular repair + VEIN GRAFTS
- III: replant in selected cases (PIP/FDS intact, clean) vs completion amputation
- Debride vessels to healthy ends; tension-free; repair nerves; soft-tissue cover
- BEFANV sequence; TWO veins per artery; close skin loosely
- Avulsion strips the VEINS too - expect vein grafts on the venous side as well
Monitoring & salvage
- Colour, refill, turgor, temperature, Doppler - hourly x 24-48 h, then 2-4 hourly
- Temperature difference above 2 deg from an adjacent digit = warning sign
- PALE, cool, no Doppler = ARTERIAL occlusion
- BLUE, tense, brisk refill, dark bleeding = VENOUS congestion (commoner)
- Loosen dressings/sutures -> leeches or nail-plate + heparin gauze (cover for Aeromonas)
- Warm, hydrated, pain-free, no nicotine/caffeine; aspirin 75-150 mg for 2-4 weeks
Decision & prognosis
- Intact PIP + FDS = best prognosis; class I/II do best
- Favour amputation: high manual demand, contamination, long ischaemia, smoker, single border/index digit
- Watch for LATE arterial failure; counsel re stiffness/cold intolerance; shared decision
Evidence & Key Studies
Ring avulsion injuries: a systematic review
- Across 20 studies (572 patients), injuries were Urbaniak class I (54), II (204) and III (314).
- Functional outcomes (total active motion, two-point discrimination) were superior for class I and II injuries.
- Selected class III injuries can be successfully treated with replantation rather than completion amputation, with shared decision-making essential.
Ring avulsion replantation by extended debridement of the avulsed digital artery and long vein grafts
- In 7 complete (Urbaniak class III) ring avulsions, replantation succeeded in all initially; long-term success was 85% (two late arterial failures, one salvaged by reoperation).
- The zone of arterial injury is more extensive than it appears, so the avulsed artery was debrided far back and bridged with long interposition vein grafts.
- With an intact PIP joint and FDS, microsurgical replantation of complete ring avulsions gave good function and aesthetics - but beware late arterial failure.
The class distribution and the superior outcomes of class I/II (with selected class III replants) come from the cited Bamba systematic review, and the extended-vessel-debridement-plus-vein-graft technique, the role of an intact PIP/FDS, and the risk of late arterial failure from the cited Akyurek series. The Urbaniak/Kay classification and the degloving mechanism are standard hand-surgery teaching.
The general replantation material - digit ischaemia tolerance (about 6 hours warm and 12 hours cold, with success reported at 24-30 hours cold in some series, because a finger contains no muscle), the preservation protocol for the amputated part, the BEFANV sequence, the two-veins-per-artery target, aspirin 75-150 mg for 2-4 weeks, the hourly monitoring parameters and the 2-degree temperature threshold, and leech or nail-plate chemical-leech salvage of venous congestion - is taken in substance from Hand and Digit Replantation, where it is set out in full with its own sources; it applies unchanged to a ring avulsion. What is specific here is that an avulsion strips the dorsal veins over the same long segment as the arteries, so vein grafts are often required on the venous side as well. (See also Fingertip Injuries.)