Schatzker Classification
What it is, and why it matters
A tibial plateau fracture breaks the weight-bearing articular surface at the top of the tibia. The Schatzker classification groups these fractures by where the fracture is (lateral plateau, medial plateau, or both) and what the fracture does (a clean split, a depressed articular fragment, or separation of the joint block from the shaft). That grouping is useful because it tracks the energy of the injury and therefore the things that actually change management: the risk of compartment syndrome, the chance of associated ligament or vascular injury, and whether the limb needs staged surgery.
The single most important idea is the energy gradient. Types I to III are lower-energy lateral injuries from a valgus force, common in younger patients. Types IV to VI cross the midline or strip the joint off the shaft, are higher-energy, and carry the dangerous associations. As you move up the numbers, you should become progressively more worried about the soft tissues and the neurovascular status of the leg — not just the bone.
The six types
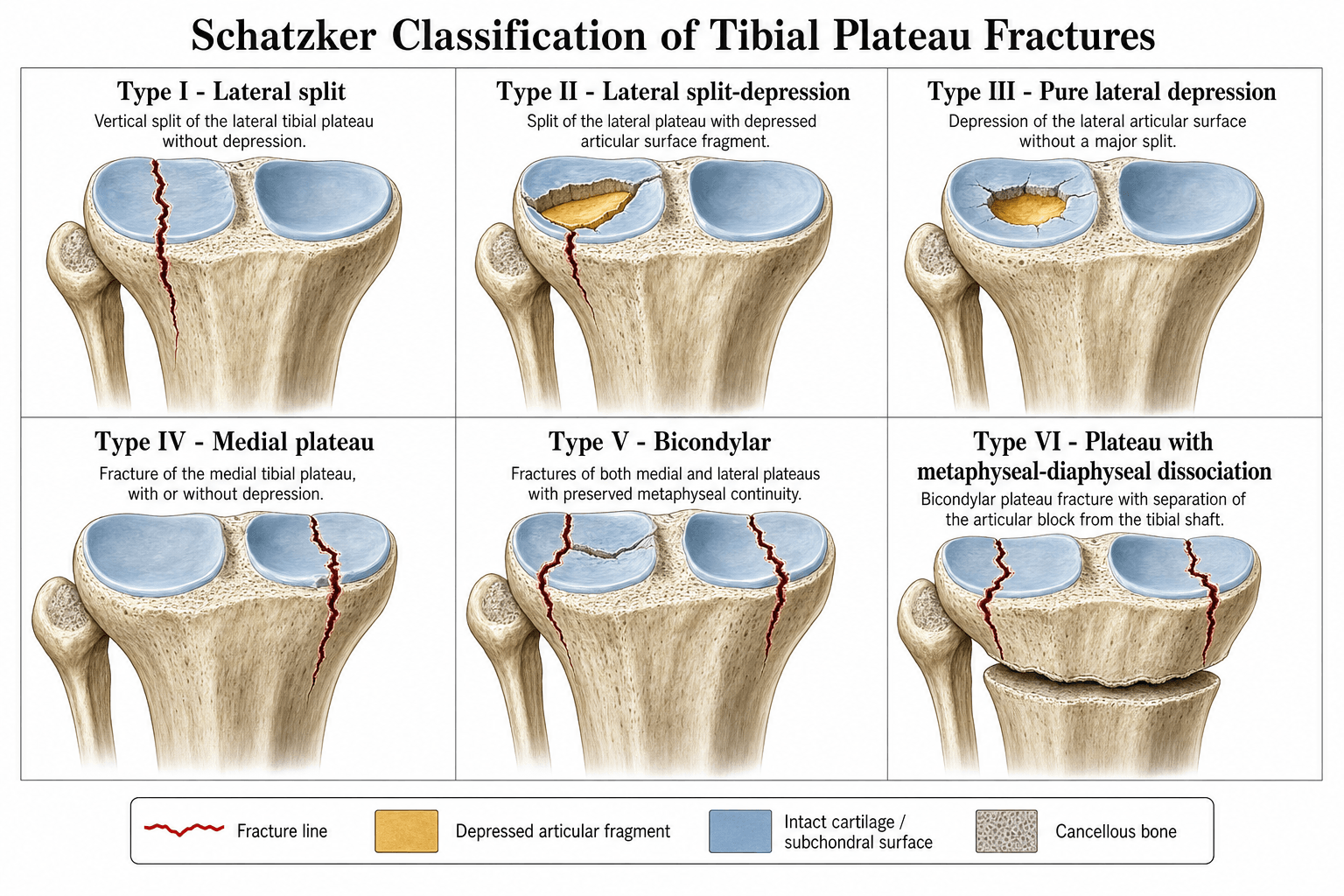
The classification is one ladder, set by the location of the main fracture lines and whether there is depression or dissociation. It is laid out once here in full; the rest of the page refers to a type by name rather than re-listing the ladder.
Imaging — why a CT is not optional
Plain radiographs (AP, lateral, and oblique views) start the assessment and are enough to assign a provisional Schatzker type, but they consistently underestimate the injury. They flatten the articular depression and hide the coronal-plane posteromedial and posterolateral fragments that dictate which approach and which plate you need.


This is not a soft recommendation. Adding CT to plain films changed the treatment plan in about a quarter of cases — 26%plan changed — and the classification in roughly 12% (Chan 1997), and it improved agreement between surgeons on what to do. Every operative plateau fracture gets a CT with coronal and sagittal reconstructions before theatre.
Management and surgical planning
Surgical urgency and approach are driven by the type, the depression/step-off, and the state of the soft-tissue envelope — not by the radiograph alone. Low-energy lateral fractures (I–III) are usually a single-stage job once any depression is elevated and buttressed. The decision thresholds below set out when to operate.
- Reasonable non-operative
- Stable split, under 2 mm displacement, no depression
- Operative indication
- Any depression over 2 mm or instability on stress
- Key surgical point
- Protect the lateral meniscus; submeniscal arthrotomy or arthroscopy to confirm reduction
- Reasonable non-operative
- Depression under 2 mm, stable knee
- Operative indication
- Step-off over 2 mm or varus/valgus instability
- Key surgical point
- Elevate through a metaphyseal window, raft-screw support, graft the void
- Reasonable non-operative
- Rarely non-operative
- Operative indication
- Almost all displaced medial fractures
- Key surgical point
- Treat as a knee-dislocation-spectrum injury — vascular assessment before and after reduction; address the posteromedial fragment
- Reasonable non-operative
- Never, when displaced
- Operative indication
- All displaced bicondylar patterns
- Key surgical point
- Staged: spanning external fixator, CT planning, definitive fixation only when the soft tissues settle
For the high-energy bicondylar patterns (V–VI), the timing of definitive surgery matters more than its speed — operating through swollen or compromised skin causes wound breakdown and deep infection.
- 1SpanApply a spanning external fixator across the knee in slight flexion to restore length and alignment, and let the soft tissues recover.
- 2Plan on CTOnce spanned, get the CT and map every fragment — especially the posteromedial fragment — to choose the approaches and plates.
- 3Definitive ORIFFix only when the swelling settles and skin wrinkles return (usually 7–14 days), typically dual plating through separate approaches.
Compartment syndrome occurs in up to ten percent of high-energy plateau fractures and must be excluded clinically before any surgery. A Type IV (or any high-energy) pattern is a knee-dislocation-spectrum injury until proven otherwise — examine and document the distal pulses and the peroneal nerve before and after every manipulation.
A predictable examiner pivot is "what are the complications, and what determines the long-term result?"
- Post-traumatic osteoarthritis is the dominant long-term outcome - driven by residual articular step-off, axial malalignment (especially varus) and meniscal loss, which is why anatomic joint reduction, restored alignment and meniscal preservation are the modifiable goals.
- Acute: compartment syndrome (up to around 10% of high-energy patterns), and the knee-dislocation-spectrum vascular/peroneal-nerve injury of Type IV.
- Wound breakdown and deep infection - the specific hazard of operating through a swollen high-energy (V/VI) envelope, hence the staged protocol.
- Stiffness/arthrofibrosis from prolonged immobilisation - mitigated by stable fixation and early range of motion.
- Malunion (varus collapse), loss of reduction/fixation failure, and (uncommon at the metaphysis) nonunion.
- Late subtotal joint destruction may ultimately need total knee arthroplasty, which is technically harder and has poorer survivorship after a plateau fracture than for primary osteoarthritis.
For the lower-energy lateral patterns (Schatzker I-III), arthroscopic-assisted reduction and internal fixation (ARIF) is an examinable option:
- It gives direct intra-articular visualisation of the reduction (more accurate than fluoroscopy for residual step-off) and lets you diagnose and treat the concomitant meniscal and chondral injury in the same sitting, with less soft-tissue stripping than an open arthrotomy.
- Technique: arthroscopic lavage of the haemarthrosis, then elevate the depressed fragment through a metaphyseal cortical window and support it with raft screws ± a buttress plate under arthroscopic control.
- Caution: it is generally reserved for I-III and avoided in high-energy V-VI, because arthroscopic fluid can extravasate through the fracture into the leg and precipitate compartment syndrome — use gravity/low-pressure inflow, limit pump pressure and operative time.
Elevating a depressed articular fragment leaves a metaphyseal void; supporting it is what stops the surface re-collapsing, and the filler choice is examinable:
- Raft screws placed immediately beneath the subchondral bone are the mechanical support; the void filler buttresses them.
- Options: autograft (iliac crest — osteogenic but limited volume and donor-site morbidity), allograft, and synthetic substitutes. Among synthetics, calcium phosphate cement has high compressive strength and a lower rate of articular subsidence/loss of reduction than the weaker, faster-resorbing calcium sulfate — making it the favoured void filler under a reduced articular surface.
- The goal is a stable subchondral construct (raft screws + structural void fill) that maintains the elevated joint line until union.
Limitations and modern context
- Inter-observer reliability of the Schatzker classification on plain radiographs is only fair to moderate (Walton 2003); adding CT improves agreement on the treatment plan more than on the classification label itself (Chan 1997), and borderline cases between Types II and V still cause disagreement.
- The original system does not capture the coronal-plane posteromedial and posterolateral fragments now recognised as critical to stability — these need dedicated fixation and are a common reason a "simple" type is harder than it looks.
- Associated soft-tissue injury is the rule, not the exception: across operative plateau fractures, MRI shows a complete cruciate/collateral tear in around three-quarters and lateral meniscus pathology in over ninety percent (Gardner 2005). The bony label alone underestimates the true injury.
- The classification remains valuable for communication and planning but should be paired with soft-tissue grading (Tscherne or Gustilo-Anderson) and detailed CT mapping.
A favourite examiner follow-up is "what are the limitations of Schatzker, and what addresses them?" The three-column classification (Luo, 2010) is the CT-based answer. It divides the proximal tibia on the axial CT slice into a lateral, a medial and a posterior column, and defines a "three-column fracture" as one with a separate fragment in each. Its value is precisely the blind spot of Schatzker: it forces recognition of the posterior (coronal-plane) column that plain films and the six-type ladder miss, and it directly drives the surgical plan - a posterior column fragment needs a posterior (inverted-L) approach and buttress, usually combined with an anterolateral approach, rather than a single anterolateral plate. Use Schatzker as the shared shorthand, but map the columns on CT to choose your approaches.
Exam & revision
Everything below condenses the topic for revision and viva practice — the high-yield points, the memory hooks, two worked vivas, and a one-screen cheat sheet.
- Energy rises with the type number — and with it the risk of compartment syndrome, ligament disruption and vascular injury.
- I–III are lateral (I split, II split-depression, III pure depression); IV is medial; V is bicondylar; VI adds metaphyseal-diaphyseal dissociation.
- Type IV signals the knee-dislocation spectrum — assess the popliteal artery and peroneal nerve before and after reduction.
- CT before fixation, always — it changed the plan in about 26% of cases and reveals posteromedial fragments invisible on plain films.
- V–VI are staged — spanning external fixator first, definitive plating once the soft tissues settle.
- The bony type underestimates the injury — soft-tissue damage (meniscus, ligaments) is present in the great majority.
Split · Split-Depress · DepressLateral three
Hook:Types I to III stay on the lateral plateau: split, then split-depress, then pure depress.
Medial · Both · DissociationMedial and beyond
Hook:Types IV to VI escalate: medial, then both, then both with the joint stripped off the shaft.
Viva practice
Practise clinical reasoning and management decisions out loud
“A thirty-five-year-old motorcyclist is brought in after a high-speed collision. The knee is swollen and deformed. Plain radiographs show a bicondylar tibial plateau fracture with apparent metaphyseal extension. What is your classification, and how do you proceed?”
“A sixty-year-old woman falls from standing onto her outstretched leg. Radiographs show an isolated lateral tibial plateau fracture with apparent central depression. How do you classify it and decide on treatment?”
The six types
- Type I: lateral split — valgus, low energy, raft screws or buttress plate
- Type II: lateral split-depression — most common, elevate and buttress
- Type III: pure central depression — axial, elderly, non-operative if stable and minimal step-off
- Type IV: medial condyle — varus, high energy, knee dislocation until proven otherwise
- Type V: bicondylar without metaphyseal extension — dual plating when soft tissues allow
- Type VI: bicondylar plus metaphyseal-diaphyseal dissociation — spanning external fixator first
Energy & soft tissue
- Higher number = higher energy, more ligament disruption, higher compartment risk
- Type IV–VI almost always need a staged protocol with temporary external fixation
- CT changes the treatment plan in about a quarter of operative cases (26%, Chan 1997)
Examination & planning
- Document compartments, pulses and neurology before and after reduction
- CT with 3D reconstructions for every operative case
- Plan approaches from the fragment positions on CT, not the plain-film label
Evidence
The tibial plateau fracture. The Toronto experience 1968-1975
- Original description of the six-type classification, linking fracture pattern (mechanism and morphology) to surgical approach and prognosis
Indications for surgical treatment of tibial condyle fractures
- In 131 tibial condyle fractures, articular step-off up to 3 mm and condylar widening up to 5 mm were well tolerated, whereas increasing medial plateau tilt and moderate-to-severe instability predicted poor function
- Recommended surgery for any displaced medial unicondylar fracture, all medially tilted bicondylar fractures, and lateral fractures with tilt/valgus over 5 degrees, step-off over 3 mm, or widening over 5 mm