Calcaneal Apophysitis | The Commonest Paediatric Heel Pain | Traction Overuse | Self-Limiting
- Traction apophysitis: Repetitive Achilles/plantar fascia pull on the calcaneal apophysis during the growth spurt - it is an overuse injury, not inflammation of a joint
- Clinical diagnosis: A positive mediolateral squeeze test of the posterior calcaneus is usually enough - imaging is NOT required for a typical presentation
- Self-limiting: Settles once the apophysis fuses (around skeletal maturity); no long-term sequelae are described
- Treatment is conservative: Load management, calf stretching, heel cushioning/orthoses - surgery has no role
- Radiographs do not confirm it: Sclerosis and fragmentation of the apophysis are common in asymptomatic children - X-rays are to exclude mimics, not to make the diagnosis
- “The single most common cause of heel pain in the 8-14 year athlete
- “Bilateral in roughly 60% - but always examine both heels and the hip
- “Squeeze test positive, single-leg heel raise reproduces pain
- “Reassure: this resolves with growth and leaves no lasting damage
The radiographic appearance of a sclerotic, fragmented calcaneal apophysis is non-specific and occurs in asymptomatic children. The danger in the exam (and in clinic) is anchoring on "Sever's" and missing a serious mimic - calcaneal osteomyelitis, a unicameral/aneurysmal bone cyst, a calcaneal stress fracture, or, in any child with hip or thigh symptoms, SCFE/Perthes referring pain to the knee/leg. Night pain, rest pain, fever, a true effusion, focal bony tenderness away from the apophysis, or systemic upset are all red flags that mandate further investigation rather than reassurance.
Overview and Epidemiology
Sever's disease (calcaneal apophysitis) is a traction apophysitis of the posterior calcaneus and is the single most common cause of heel pain in active children. It is named after James Warren Sever, who described it in 1912. It is a benign, self-limiting overuse condition of the growing skeleton, not a true "disease" in the pathological sense - the more accurate descriptive term is calcaneal apophysitis.
Epidemiology:
- Most common cause of paediatric and early-adolescent heel pain
- Peak age 8 to 14 years (girls tend to present a little earlier than boys, mirroring earlier skeletal maturation)
- Bilateral in a high proportion of cases - frequently quoted around 60%
- Strongly associated with running and jumping sports - soccer, Australian football, basketball, gymnastics, track, tennis and dance
- Higher body mass index and high training volume are recurrent risk associations
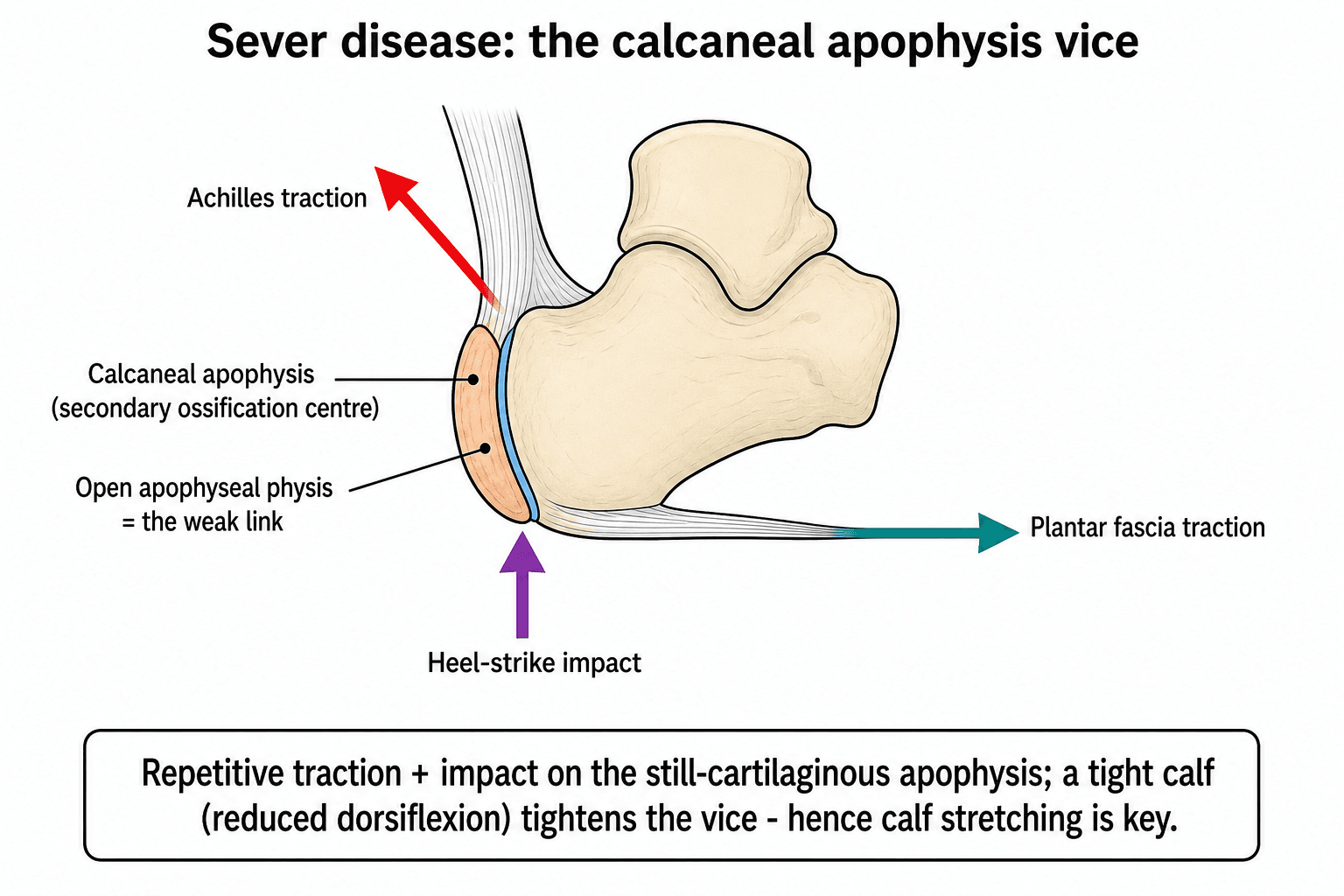
The calcaneal apophysis is a secondary ossification centre at the posterior heel. During the adolescent growth spurt, the calcaneus lengthens faster than the gastrocnemius-soleus-Achilles complex can accommodate, so the muscle-tendon unit becomes relatively tight. The Achilles inserts onto the apophysis superiorly and the plantar fascia onto it inferiorly, sandwiching the still-cartilaginous growth plate between two strong tractioning structures. Repetitive impact loading then produces microtrauma at this vulnerable junction - the essence of a traction apophysitis.
Etiology and Risk Factors:
- Open apophysis: Skeletal immaturity is the prerequisite
- Limited ankle dorsiflexion: The most consistently reported intrinsic risk factor
- Gastrocnemius-soleus tightness: Increases traction across the apophysis
- Rapid growth: Bone outpaces the soft-tissue envelope
- Foot alignment: Pronated or cavus foot postures alter heel loading
- Higher body mass index: Increases impact load
- High-impact sport: Running, jumping, kicking, sprinting
- Training load: Rapid increases in volume or intensity
- Hard surfaces and poor footwear: Increase peak heel pressures
- Cleated/flat boots: Little heel cushioning (e.g. football boots)
- Multiple concurrent sports: Inadequate recovery between sessions
Natural History:
- Symptoms wax and wane with activity over months to a couple of years
- Resolves spontaneously once the calcaneal apophysis fuses (around skeletal maturity)
- No long-term structural sequelae, deformity or arthritis are described
- The role of the clinician is accurate diagnosis, exclusion of mimics, symptom control and reassurance
Pathophysiology and Anatomy
The Calcaneal Apophysis
The posterior calcaneus develops a secondary ossification centre (the apophysis) that appears in childhood and fuses around the end of skeletal growth. It lies between two powerful tractioning structures:
- Achilles tendon - inserts onto the posterosuperior apophysis
- Plantar fascia - originates from the inferior aspect of the calcaneal tuberosity
The cartilaginous physis between the apophysis and the calcaneal body is the weak link during growth, analogous to the tibial tubercle in Osgood-Schlatter disease and the inferior patellar pole in Sinding-Larsen-Johansson syndrome.
- Approx. age (years)
- 0-7
- Description
- Posterior calcaneus largely cartilaginous
- Clinical Relevance
- Apophysitis rare at this age - investigate atypical pain
- Approx. age (years)
- 7-9
- Description
- Secondary ossification centre becomes radiographically visible
- Clinical Relevance
- Onset of the vulnerable period
- Approx. age (years)
- 9-12
- Description
- Apophysis ossifying, growth spurt, high sport load
- Clinical Relevance
- Peak incidence of Sever's disease
- Approx. age (years)
- 12-15+
- Description
- Apophysis fuses to the calcaneal body
- Clinical Relevance
- Symptoms resolve as fusion completes
Think of the apophysis as being squeezed in a vice: the Achilles pulls from above and behind, the plantar fascia pulls from below, and ground-reaction impact hammers it from beneath at heel strike. A tight calf (reduced ankle dorsiflexion) tightens that vice, which is exactly why dorsiflexion limitation is the most reproducible risk factor and why calf stretching is a cornerstone of treatment.
Pathophysiology
The condition is a repetitive microtrauma / overuse phenomenon rather than a primary inflammatory or avascular process. Cyclical tensile and compressive loading of the still-cartilaginous apophyseal plate produces microscopic injury and a reparative response. The radiographic sclerosis and fragmentation often seen are largely a feature of normal apophyseal ossification under load, which is why identical appearances occur in pain-free children.
In a child, posterior heel pain is far more likely to be apophysitis than tendinopathy. The pain localises to the posterior calcaneus at the apophysis, reproduced by the squeeze test, rather than to the substance of the Achilles tendon. Treating a growing child as if they had adult Achilles tendinopathy (e.g. aggressive eccentric loading into pain) misses the point - the goal is to offload the apophysis and manage training load.
Classification and Severity
There is no universally adopted formal classification for Sever's disease; it is graded pragmatically by symptom severity and functional impact, which directly guides intensity of treatment.
Clinical Severity Grading
- Symptoms
- Heel pain only after sport, settles with rest, no limp
- Impact on Activity
- Completes training and play
- Treatment Emphasis
- Calf stretching, heel cushioning, continue sport
- Symptoms
- Pain during and after sport, mild limp afterwards
- Impact on Activity
- Performance and participation affected
- Treatment Emphasis
- Reduce load, heel raise/orthosis, formal physiotherapy
- Symptoms
- Pain on everyday walking, persistent limp, pain at rest with activity
- Impact on Activity
- Unable to play sport
- Treatment Emphasis
- Relative rest from impact, NSAIDs for flares, consider short immobilisation
Grading is useful because it dictates how much load to remove, not whether to operate (you never operate). Milder cases need only activity modification and cushioning; more severe cases need a genuine reduction in impact loading for a period, with a graded return as the squeeze test becomes painless. All grades share the same favourable endpoint at skeletal maturity.
Clinical Assessment
History:
- Age and growth: Peak 8-14 years, often during a growth spurt
- Sport: Type, frequency, recent increase in load, surface, footwear
- Pain pattern: Posterior heel, activity-related, eases with rest
- Laterality: Often bilateral (examine both regardless)
- Limp: Present after sport in moderate-to-severe cases
- Footwear: Flat/cleated boots with poor heel cushioning
- Night pain or rest pain: Tumour, infection
- Fever, systemic upset: Osteomyelitis, malignancy
- Acute trauma: Calcaneal or stress fracture
- Swelling, warmth, true effusion: Atypical for Sever's
- Hip or thigh symptoms: Always clear the hip (SCFE, Perthes)
- Pain not related to activity: Reconsider the diagnosis
Physical Examination:
Systematic Examination
- Gait, looking for an antalgic limp or toe-walking to offload the heel
- Compare both heels; look for swelling, redness or deformity (usually absent in Sever's)
- Assess foot posture (pronation or cavus) and footwear
- Mediolateral squeeze (calcaneal compression) test: compress the posterior calcaneus from both sides at the apophysis - reproduction of pain is the hallmark finding
- Tenderness localises to the posterior calcaneus, NOT the Achilles substance or its midportion
- Palpate away from the apophysis for focal bony tenderness (would suggest a mimic)
- Ankle dorsiflexion: typically reduced (tight gastrocnemius-soleus) - measure with the knee extended and flexed
- Subtalar and midfoot motion: usually normal
- A true effusion or restricted, painful global ankle motion is atypical and should prompt review
- Single-leg heel raise / hopping: reproduces posterior heel pain
- Always examine the hip: SCFE and Perthes can refer pain distally; this is a classic exam trap and a medicolegal pitfall
- Neurovascular check to complete the limb assessment
The mediolateral calcaneal squeeze test is the signature clinical sign: squeezing the posterior calcaneus from both sides reproduces the child's pain. Combined with the right age, activity-related posterior heel pain and a tight calf, a positive squeeze test is generally sufficient to diagnose Sever's disease without imaging.
Investigations
Sever's disease is a clinical diagnosis. Investigations are used to exclude mimics, not to confirm apophysitis.
- Typical age (8-14 years)
- Activity-related posterior heel pain
- Positive squeeze test
- No red flags
- No systemic features
In this classic picture, routine radiographs add nothing and risk overdiagnosis from incidental apophyseal sclerosis.
- Atypical age or presentation
- Night pain, rest pain, systemic upset
- Focal bony tenderness away from the apophysis
- History of significant trauma
- Failure to settle with appropriate conservative care
- What It Shows
- Apophyseal sclerosis/fragmentation (non-specific); excludes fracture, cyst, tumour
- Role in Sever's
- Only if red flags or atypical - to exclude mimics
- What It Shows
- Raised in infection or inflammatory arthritis
- Role in Sever's
- If infection or systemic illness suspected
- What It Shows
- Soft-tissue and tendon assessment; user-dependent
- Role in Sever's
- Selective - atypical or refractory cases
- What It Shows
- Marrow oedema, occult fracture, osteomyelitis, tumour
- Role in Sever's
- Reserved for diagnostic uncertainty or to exclude serious mimics
Because apophyseal sclerosis and fragmentation occur in pain-free children, a "positive-looking" X-ray does not prove Sever's and a "normal-looking" apophysis does not exclude it. Use imaging to answer a specific question (is this infection, fracture, cyst or tumour?) rather than to label the apophysitis.



Differential Diagnosis
- Distinguishing Features
- 8-14y, activity-related posterior heel pain, positive squeeze test, tight calf
- Key Action
- Clinical diagnosis, conservative management
- Distinguishing Features
- Pain at rest/night, fever, focal tenderness, raised CRP/ESR
- Key Action
- URGENT - bloods, imaging (MRI), treat infection
- Distinguishing Features
- Acute or rapid onset, focal tenderness, positive squeeze but trauma/overload history
- Key Action
- Imaging (MRI/bone scan), offload
- Distinguishing Features
- Localised pain, possible pathological fracture, focal lytic lesion on X-ray
- Key Action
- Imaging and onward referral
- Distinguishing Features
- Pain in tendon substance or insertion, older/adolescent, less typical in young children
- Key Action
- Examine the tendon; manage as soft-tissue pathology
- Distinguishing Features
- Plantar medial heel pain, worse on first steps, uncommon in young children
- Key Action
- Clinical; consider if plantar rather than posterior pain
- Distinguishing Features
- Stiff, painful hindfoot, recurrent sprains, peroneal spasm
- Key Action
- Imaging (CT/MRI) of the hindfoot
- Distinguishing Features
- Hip/thigh/knee symptoms, altered hip rotation
- Key Action
- ALWAYS examine the hip in paediatric leg pain
- Infection - a child with rest/night pain, fever or raised inflammatory markers has osteomyelitis until proven otherwise, not Sever's.
- Referred hip pathology - SCFE and Perthes can present with distal leg pain. Examining the hip in every child with leg or heel pain is both good practice and a recurrent viva and medicolegal point.
Management
Management is entirely conservative and built on load management, calf flexibility, heel offloading and reassurance. There is no role for surgery, and corticosteroid injection is not used.
Stepwise Conservative Management
- Explain the benign, self-limiting natural history to child and parents
- Reduce, do not abolish, impact sport - cut volume and intensity to a pain-tolerable level
- Substitute lower-impact cross-training (cycling, swimming) during flares
- Address footwear: a cushioned heel; avoid hard, flat or worn-out footwear
- Ice to the heel after activity
- Simple analgesia / short-course NSAIDs for painful flares only
- Relative rest during severe flares
- Heel cups, heel raises or foot orthoses reduce load on the apophysis
- Custom foot orthoses may outperform off-the-shelf heel lifts in some trials, though both reduce pain
- For barefoot-sport athletes (gymnasts, dancers), specific heel braces are an alternative
- Gastrocnemius-soleus stretching to address the tight calf / limited dorsiflexion
- Eccentric/concentric calf and foot strengthening as tolerated
- Graded return-to-sport programme guided by symptoms and the squeeze test
- For genuinely refractory or severe symptoms: a period of relative rest, occasionally a short spell of immobilisation (e.g. walking boot/cast) for a few weeks to break the cycle
- Reassess the diagnosis if symptoms do not respond - re-examine and image to exclude mimics
- Extracorporeal shockwave therapy has been described but the evidence base is weak
Complications and Prognosis
- Excellent - self-limiting, resolves as the apophysis fuses around skeletal maturity
- No described long-term deformity, growth disturbance or arthritis
- Symptoms may persist or recur for months to a couple of years while the child is still growing and active
- The main "complication" is missed time from sport and parental anxiety - both mitigated by reassurance
- Missed mimic (infection, fracture, tumour, referred hip) - the only serious risk
- Deconditioning from unnecessary prolonged rest
- Overtreatment / overinvestigation of a benign condition
- Failure to reassess when symptoms do not follow the expected course
The most therapeutic intervention is often accurate reassurance: this is a common, benign overuse condition of the growing heel that does not cause lasting damage and reliably resolves with growth, provided serious mimics have been excluded.
Guidelines, Registries & Global Practice
Global epidemiology. Calcaneal apophysitis is a worldwide condition of the skeletally immature, running and jumping athlete and is consistently reported as the most common cause of paediatric heel pain. A systematic review of risk factors (1265 children, mean age 10.7 years) identified limited ankle dorsiflexion, increased plantar pressures, foot malalignment and higher body mass index as recurrent associations, according to PubMed (DOI). There is no dedicated registry; surveillance comes from sports-medicine cohorts and treatment trials rather than arthroplasty-style national registries.
Guideline landscape. No major society publishes a Sever's-specific guideline; recommendations are drawn from paediatric overuse-injury and apophysitis guidance, which is strikingly consistent across systems - the diagnosis is clinical and management is conservative.
- Position
- Activity modification, calf stretching, heel cushioning/orthoses; reassurance about the self-limiting course
- Imaging Stance
- Clinical diagnosis; radiograph only for atypical features or to exclude other pathology
- Evidence Basis
- Expert consensus, supported by small RCTs
- Position
- Primary-care conservative management, load modification, physiotherapy; referral reserved for red flags
- Imaging Stance
- Imaging not routine; reserved for diagnostic uncertainty or trauma
- Evidence Basis
- CKS-type narrative guidance, consensus-based
- Position
- Conservative care, family education; avoid overinvestigation of incidental apophyseal change
- Imaging Stance
- Selective imaging only
- Evidence Basis
- Consensus / practice standards
- Position
- Load management, calf flexibility and graded return; flag prolonged or atypical courses
- Imaging Stance
- Ultrasound or MRI selectively for atypical or refractory cases
- Evidence Basis
- Cohort and RCT evidence (Level 2-3)
- Position
- Training-load monitoring during growth spurts; gradual return-to-sport progression
- Imaging Stance
- Clinical diagnosis emphasised
- Evidence Basis
- Consensus / sports guidance
The main international variation is in imaging threshold and use of orthoses, not in the core approach: management is uniformly conservative worldwide. Higher-resource and elite-sport settings use ultrasound/MRI more liberally and prescribe custom orthoses, while primary-care systems keep the diagnosis clinical and favour simple heel cushioning. Randomised evidence suggests no in-shoe device is clearly superior in the medium term (DOI), so cost and preference reasonably guide device choice.
Medicolegal Considerations:
Key documentation points:
- History of gradual, activity-related posterior heel pain in a child of typical age
- Documentation of a positive squeeze test and reduced ankle dorsiflexion
- Explicit screening for red flags (night pain, fever, systemic upset, trauma)
- Hip examination performed to exclude referred SCFE/Perthes
- Discussion of the benign, self-limiting natural history and a plan for review if symptoms do not follow the expected course
Don't Miss the Mimics: Failing to recognise calcaneal osteomyelitis or referred hip pathology in a child labelled with "Sever's" is a recognised source of harm and litigation. Document the red-flag screen and hip examination in every case.
Prevention Strategies:
- Training-load management during growth spurts (progress volume before intensity)
- Calf flexibility work and attention to footwear with adequate heel cushioning
- Awareness among coaches and parents that activity-related heel pain in this age group is usually benign but should be assessed
Memory Aids
SEVERSEVER - Core Features
Hook:If you can SEVER the link between sport overload and a growing heel, the pain settles - it is a traction overuse problem that growth eventually cures.
HEELHEEL - Conservative Management
Hook:Look after the HEEL with cushioning, stretching, education and load control - no injections, no surgery.
LIMPLIMP - Red Flags That Are NOT Sever's
Hook:A child with a LIMP and any of these features has earned investigation, not reassurance.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 11-year-old boy who plays a lot of football presents with a 6-week history of pain at the back of both heels. The pain is worse after matches and he sometimes limps off the pitch. He is otherwise well.”
“A 9-year-old presents with heel pain. This child also wakes at night with pain, feels generally unwell, and on examination has a low-grade fever, warmth over the heel and focal bony tenderness. An X-ray shows a sclerotic, fragmented calcaneal apophysis.”
“A 13-year-old competitive gymnast has had calcaneal apophysitis confirmed clinically. Despite calf stretching and activity advice over 8 weeks she still has limiting bilateral heel pain and is missing competitions. The family is anxious and asking whether she needs surgery.”
Key Anatomy
- Calcaneal apophysis = secondary ossification centre at posterior heel
- Achilles inserts above, plantar fascia originates below - the 'sandwich'
- Cartilaginous physis is the weak link during growth
- Apophysis fuses around skeletal maturity
Diagnosis
- Clinical diagnosis - imaging NOT required if typical
- Mediolateral calcaneal squeeze test positive
- Age 8-14 years, activity-related posterior heel pain
- Reduced ankle dorsiflexion (tight calf); often bilateral
Treatment
- Load MODIFICATION, not complete rest
- Calf (gastrocnemius-soleus) stretching
- Heel cushioning / heel raise / foot orthoses
- Ice and short-course NSAIDs for flares
- No surgery, no injection - ever
Imaging Indications
- Night or rest pain (tumour, infection)
- Fever or systemic upset (osteomyelitis)
- Significant trauma (fracture)
- Atypical age or failure of conservative care
Red Flags (NOT Sever's)
- Night/rest pain, fever = infection or tumour
- Focal bony tenderness away from apophysis
- Acute trauma = fracture / stress fracture
- Hip or thigh symptoms = SCFE, Perthes
Prognosis
- Excellent - self-limiting with skeletal maturity
- No long-term deformity or arthritis
- Symptoms may fluctuate for months while still growing
- Reassurance is a key part of treatment
Evidence Base
Sever's disease has a modest but growing evidence base, dominated by conservative-treatment trials and risk-factor studies. Each card below is verified against PubMed. Because the underlying mechanism is shared with other paediatric apophysitides, some principles are extrapolated from that broader literature and labelled where relevant.
Footwear and Foot Orthoses: 12-Month Factorial RCT
- Factorial 2x2 randomised trial in 124 children aged 8-14 with calcaneal apophysitis
- Compared heel raises versus prefabricated orthoses, with or without footwear replacement
- A relative advantage of heel raises over prefabricated orthoses was seen only at the 2-month point in the physical domain
- By 6 and 12 months there was no advantage of any one treatment over another - all groups improved
Custom Foot Orthoses vs Heel-Lifts: CONSORT-Compliant RCT (n=208)
- Randomised trial of 208 children aged 9-12 with calcaneal apophysitis over 12 weeks
- Custom-made polypropylene foot orthoses versus off-the-shelf heel-lifts
- Both groups improved in pain (VAS) and pressure-pain threshold (algometry)
- Custom orthoses produced significantly greater improvement (VAS reduction approximately 69% vs heel-lifts)
Conservative Treatment: Systematic Review of RCTs
- Systematic review of 8 randomised controlled trials of conservative treatment
- Interventions included insoles, therapeutic exercises, kinesio taping and foot orthoses
- Good overall methodological quality (mean PEDro score 6.75)
- Conservative treatment was an effective option for relieving Sever's disease symptoms
Risk and Associated Factors: Systematic Review
- Systematic review of 11 observational studies (1265 participants, mean age 10.7 years)
- Limited ankle dorsiflexion was the most frequently identified intrinsic risk factor
- Increased plantar pressures and foot malalignment were also associated
- Higher body mass index, age, sex, sport participation and other osteochondroses were implicated