Diastematomyelia | Pang Types I-II | Tethered Cord | Pre-Scoliosis MRI Mandate
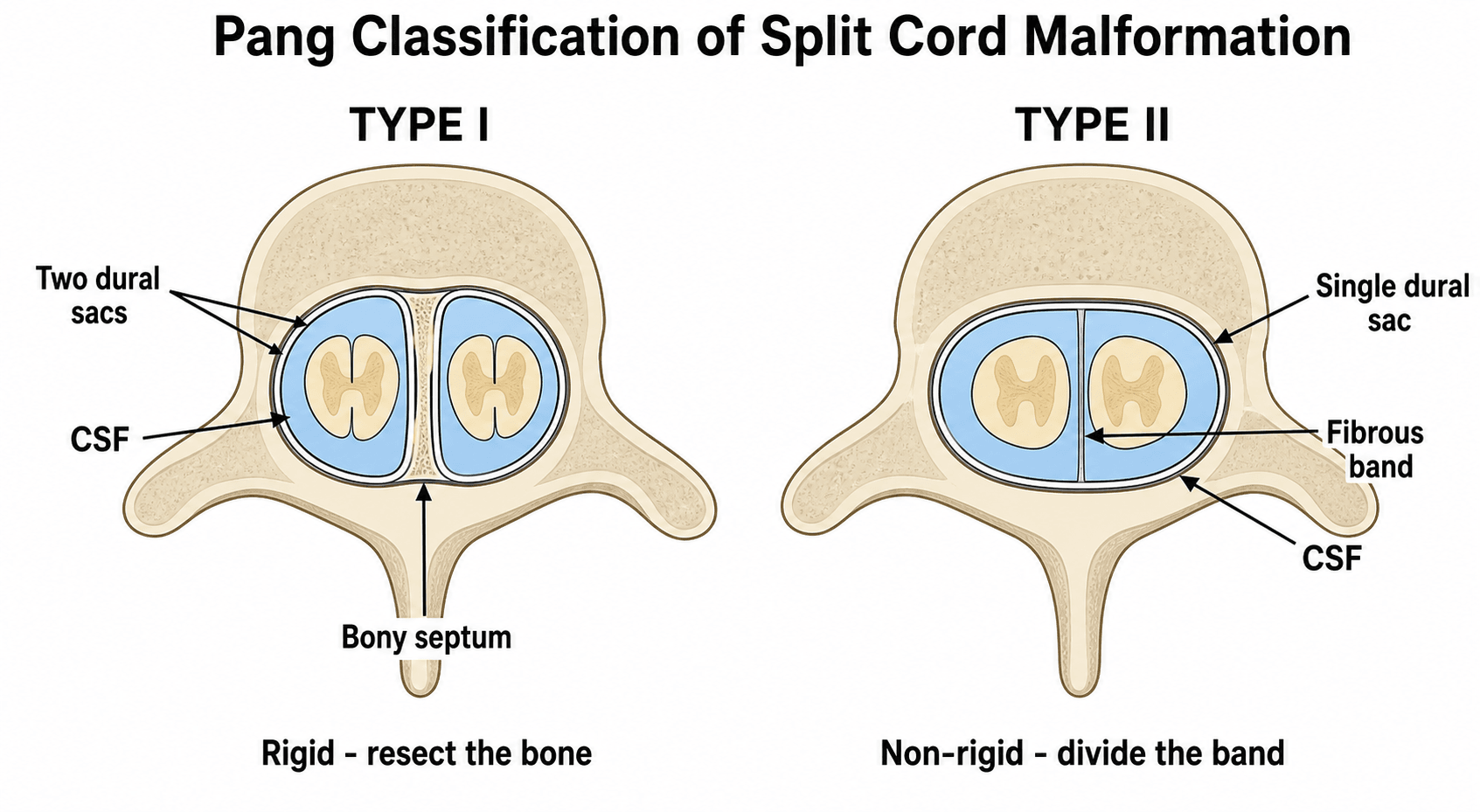
- Pang Type I has separate dural sacs and bony septum; Type II shares one dural sac with fibrous band
- Cutaneous marker (hairy patch) highly suggestive; always image the whole spine
- Up to 80 percent coexist with congenital scoliosis or kyphosis
- MRI is mandatory before any corrective surgery for congenital spinal deformity
- Progressive neurological deficit or bladder dysfunction indicates need for detethering
- “Hairy patch at lumbar level = split cord until proven otherwise
- “Type I septum is bony and can cause cord compression or tether
- “Always obtain full-spine MRI with contrast before scoliosis correction
- “Tethered cord signs may appear after growth spurts or after deformity surgery if missed
Hypertrichosis (hairy patch) is the classic sign. Also look for dermal sinus, lipomatous mass, or asymmetric gluteal cleft. Any midline cutaneous lesion below L1 demands MRI.
Asymmetric leg weakness, cavus feet, or bladder dysfunction in a child with scoliosis. The neurological level often does not match the bony deformity level.
Congenital scoliosis with a unilateral bar or hemivertebra has greater than 60 percent chance of occult SCM. MRI changes the surgical plan in up to one-third of cases.
MRI before any instrumentation or osteotomy. Missing SCM risks acute neurological injury when the cord is stretched or the septum is pulled during correction.
- Diagnosis
- MRI shows Type I or II SCM
- Action
- Close observation or prophylactic detether
- Key Pearl
- Cutaneous marker alone justifies imaging
- Diagnosis
- SCM with tethered cord on MRI
- Action
- Surgical detethering before or with correction
- Key Pearl
- Delay risks irreversible deficit
- Diagnosis
- No pre-op MRI performed
- Action
- Cancel surgery until MRI obtained
- Key Pearl
- Never instrument without MRI clearance
MRI SAFEPre-Scoliosis Surgery Checklist
Hook:MRI SAFE before every congenital scoliosis case - split cord kills if you forget!
Overview and Epidemiology
Split cord malformation is an occult spinal dysraphism that frequently coexists with congenital scoliosis. Missing the diagnosis before corrective osteotomy or instrumentation can produce catastrophic cord injury when the hemicords are stretched across a fixed septum. MRI is therefore mandatory in every child with congenital spinal deformity, even when neurological examination appears normal. Early recognition allows safe detethering and dramatically reduces operative risk.
- Primary neurulation failure: Split notochord or adhesion between ectoderm and endoderm
- Pang unified theory: Both Type I and II result from similar embryologic error at days 18-25
- Associated anomalies: Hemivertebra, block vertebra, rib fusions, diastematomyelia at same or remote level
- Incidence: Rare, estimated 1 in 5000-10000 live births
- Sex ratio: Slight female predominance
- Presentation age: Infancy to adolescence; many diagnosed during scoliosis workup
- Scoliosis link: 60-80 percent of SCM patients have congenital vertebral anomalies
Pathophysiology
The split cord creates two hemicords that are mechanically tethered. In Type I the rigid bony septum fixes the cord and prevents normal ascent during growth. In Type II the fibrous band produces similar tethering. Additional tethering may occur from a thickened filum terminale or scar. Progressive stretch produces ischemia, axonal loss, and syringomyelia. Any corrective maneuver that lengthens the spinal column (distraction, osteotomy) can acutely worsen the tether if the septum is not removed first.
- Type I (Diastematomyelia)
- Two separate dural sacs
- Type II (Diplomyelia)
- Single shared dural sac
- Type I (Diastematomyelia)
- Bony or osteocartilaginous
- Type II (Diplomyelia)
- Fibrous band only
- Type I (Diastematomyelia)
- Hemicords widely separated
- Type II (Diplomyelia)
- Hemicords close together
- Type I (Diastematomyelia)
- Rigid bony fixation
- Type II (Diplomyelia)
- Flexible fibrous tether
- Type I (Diastematomyelia)
- Higher - requires bone removal
- Type II (Diplomyelia)
- Lower - band division only
Low-lying conus (below L2) or thickened filum greater than 2 mm is present in most cases. The split itself acts as a tether point. Growth spurts or spinal lengthening during scoliosis surgery increase tension and produce acute or progressive deficit.
Correction of congenital scoliosis often requires distraction, derotation, or vertebral column resection. An unrecognized bony septum will act as a fulcrum and tear the hemicords. Even Type II fibrous bands can produce significant stretch injury once the spine is lengthened.
Where SCM Sits: the Classification of Spinal Dysraphism
Examiners expect you to place split cord malformation within the wider spinal-dysraphism framework rather than treat it in isolation. The first division is open versus closed, and the closed (occult) group is then split by whether there is a subcutaneous mass:
- Skin
- Neural tissue exposed / not skin-covered
- Examples
- Myelomeningocele, myelocele - present at birth, need urgent closure
- Skin
- Skin-covered lump
- Examples
- Lipomyelomeningocele, posterior meningocele, myelocystocele
- Skin
- Skin-covered, often only a cutaneous stigma
- Examples
- Split cord malformation (diastematomyelia), tethered/thickened filum, filum lipoma, dorsal dermal sinus, caudal regression
SCM is a closed (occult) dysraphism without a subcutaneous mass - which is exactly why the subtle cutaneous stigmata (hairy patch, sinus, dimple) matter so much: there is no obvious lump to prompt imaging and the cord is fully skin-covered. The unifying functional theme across the whole closed group is tethering of the cord.
BONY FIBROUSPang Classification
Hook:BONY = Type I (separate sacs); FIBROUS = Type II (single sac) - always screen the whole spine!
Classification and Types
Pang Classification (Standard for Surgical Planning)
- Dural Sacs
- Two separate sacs
- Septum
- Bony or cartilaginous
- Typical Level
- Thoracolumbar
- Surgical Goal
- Resect septum, close dual sacs
- Dural Sacs
- Single shared sac
- Septum
- Fibrous band
- Typical Level
- Any level
- Surgical Goal
- Divide band, preserve single sac
Type I is more likely to produce early neurological signs because of the rigid septum. Type II may remain occult until a growth spurt or scoliosis surgery unmasks the tether.
Clinical Assessment
- Cutaneous lesion: Noted at birth or during growth
- Neurological progression: Leg weakness, numbness, or gait change
- Bladder/bowel: Incontinence, recurrent UTI, constipation
- Scoliosis history: Curve noticed by parents or school screen
- Prior surgery: Any previous spinal procedure without MRI
- Skin: Hairy patch, dermal sinus, lipoma, asymmetric cleft
- Legs: Asymmetric atrophy, cavus feet, trophic ulcers
- Neurology: Asymmetric reflexes, sensory level, Babinski
- Spine: Congenital curve, kyphosis, local tenderness
- Urodynamics: If any bladder symptom or before surgery
Any child with congenital scoliosis plus one of the following requires MRI: hairy patch, leg-length discrepancy, cavus foot, early-onset progressive deficit, or neurogenic bladder. The absence of cutaneous markers does not exclude SCM - up to 30 percent have completely normal skin.
- Typical Level
- Lumbosacral
- Associated Risk
- SCM Type I or II
- Next Step
- Full-spine MRI
- Typical Level
- Any level
- Associated Risk
- Infection, dermoid, tether
- Next Step
- MRI + surgical excision
- Typical Level
- Lumbosacral
- Associated Risk
- Lipomyelomeningocele
- Next Step
- MRI + neurosurgical referral
- Typical Level
- Gluteal crease
- Associated Risk
- Low risk if above coccyx
- Next Step
- Ultrasound or MRI if atypical
HAIRY PATCHCutaneous and Clinical Markers
Hook:HAIRY PATCH = the one finding that should trigger full-spine MRI in every child with spinal deformity!
Investigations

Imaging Protocol
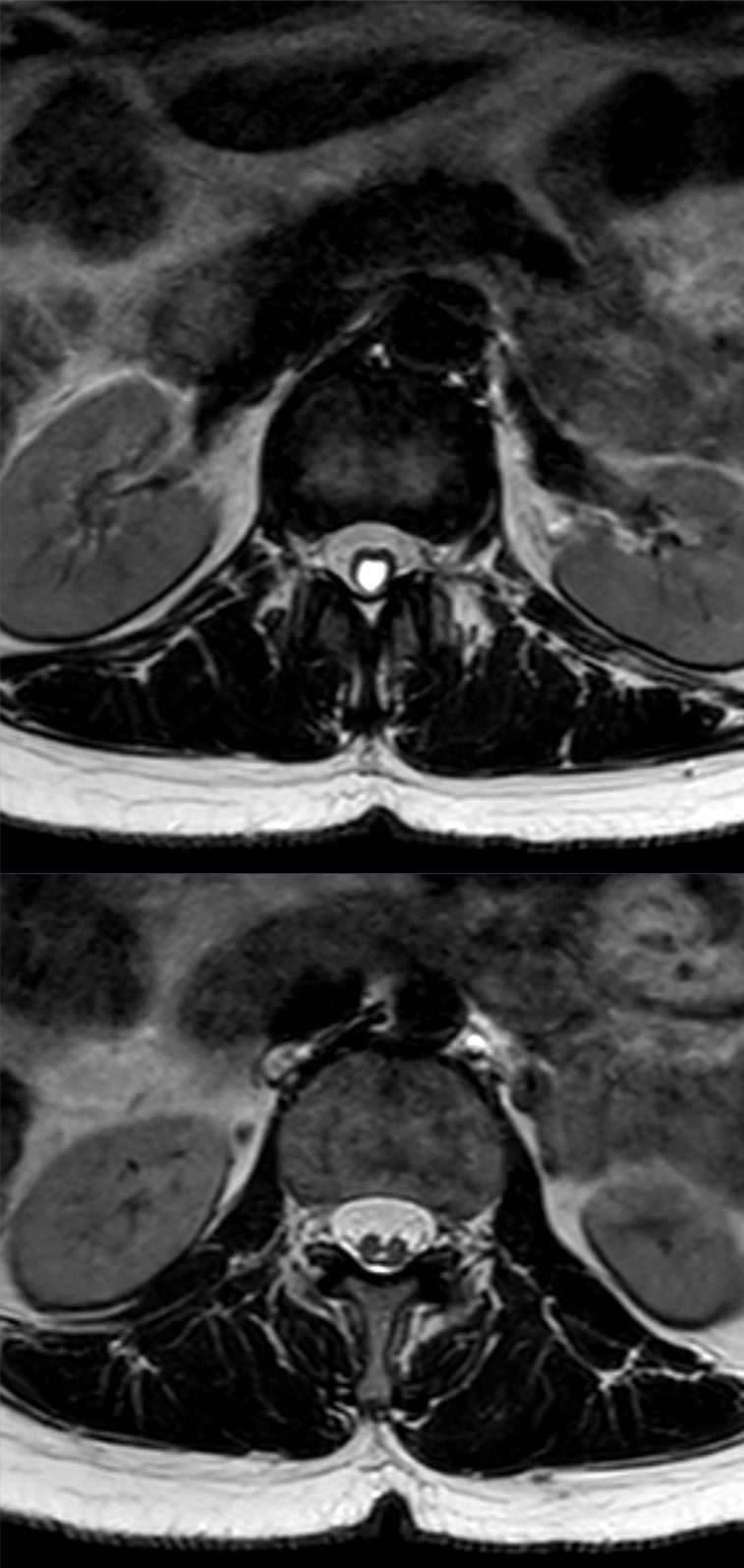
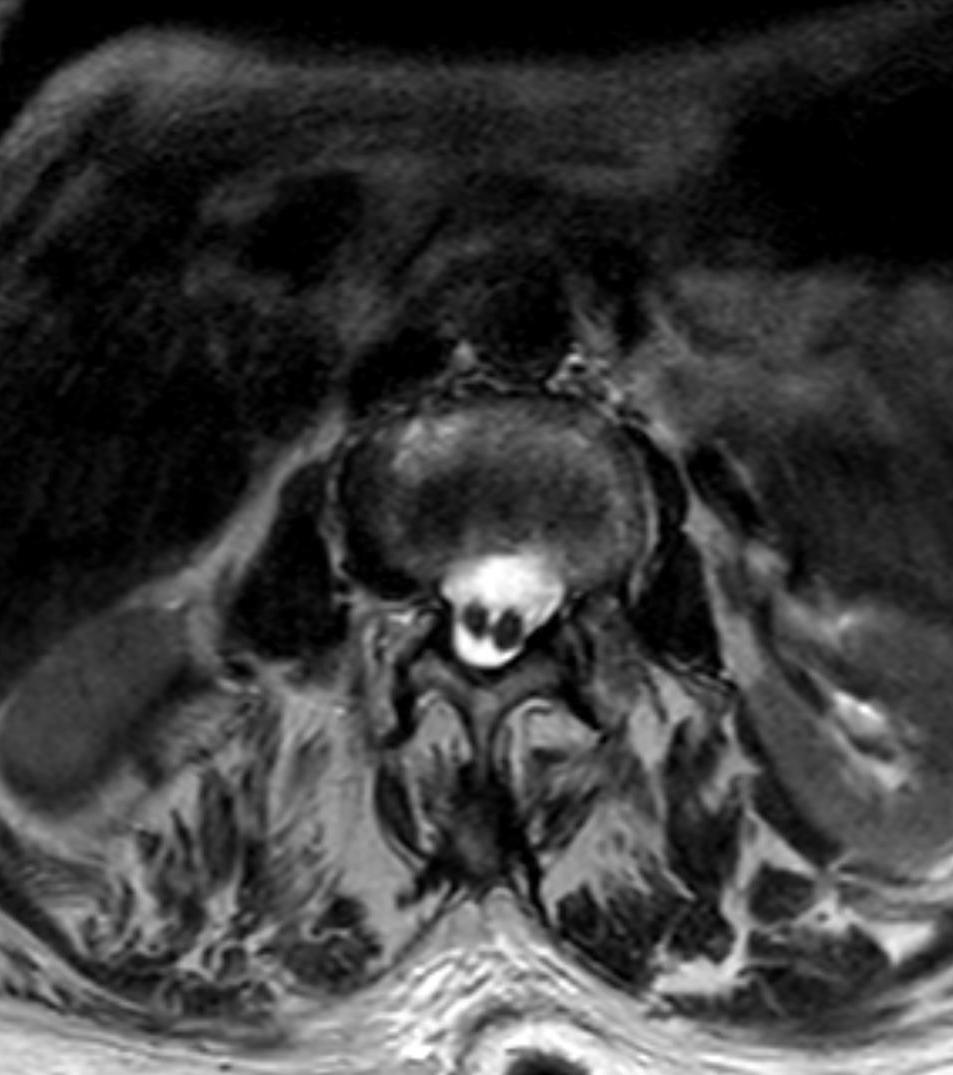
Sequences: Sagittal and axial T1, T2, STIR, post-contrast T1 Look for: Hemicords, septum (bony vs fibrous), conus level, filum thickness, syrinx, lipoma, Chiari Clinical correlation: Axial images are essential - sagittal views alone can miss the split
Indication: Delineate bony anatomy before resecting septum Findings: Location and extent of bony bar, associated vertebral anomalies Pre-op planning: Helps anticipate dural closure difficulty
Indication: Any history of incontinence or before scoliosis surgery Findings: Detrusor-sphincter dyssynergia or high-pressure voiding Post-op value: Baseline for monitoring neurological recovery
MRI is diagnostic. CT is only for surgical planning of the bony septum. Plain radiographs show the scoliosis and vertebral anomalies but never confirm or exclude SCM. If a child with congenital scoliosis arrives without MRI, obtain it before booking the operating room.
In the neonate and young infant (up to about 3 to 6 months) the posterior vertebral elements are incompletely ossified, leaving an acoustic window that makes spinal ultrasound the first-line screen for a cutaneous stigma (sacral dimple, hairy patch, lipoma, dermal sinus). Ultrasound can show the conus level, cord pulsation/movement, a thickened filum and even the hemicords of an SCM, with no sedation and no radiation. A confidently normal study in a low-risk marker can avoid MRI; an abnormal, equivocal or high-risk finding - and any child beyond the ossification window - proceeds to MRI, which remains the definitive test. This newborn-clinic pathway for an isolated skin marker is distinct from the pre-deformity-surgery MRI mandate.
Management Algorithm
Asymptomatic Split Cord with Scoliosis
Goal: Protect the cord during planned deformity correction
- Obtain full-spine MRI with contrast before any surgical planning
- If Type I bony septum present: plan simultaneous or staged detethering and septum resection
- If Type II fibrous band: divide band during the same anesthetic as scoliosis correction
- Always section the filum terminale if it is thickened or the conus is low
- Intraoperative neuromonitoring is mandatory
Complications
Complications arise from the natural history of an untreated split cord, from missed diagnosis during deformity surgery, and from the detethering operation itself.
- Progressive tethered-cord syndrome: worsening leg weakness, sensory loss, cavus foot deformity and gait deterioration with growth
- Neurogenic bladder/bowel: detrusor-sphincter dyssynergia, recurrent UTI, incontinence - may be irreversible if late
- Syringomyelia extending into the hemicords
- CATASTROPHIC intra-operative cord injury: distraction/derotation across an unrecognised bony septum can transect the hemicords - the feared, preventable disaster of congenital-scoliosis surgery
- Curve progression while definitive correction is deferred
- New or worsened neurological deficit (motor, sensory, bladder) from manipulation of the hemicords
- CSF leak / pseudomeningocele - especially the difficult dual-tube dural closure in Type I
- Wound infection / meningitis
- Re-tethering from scar (may present with late deterioration after initial improvement)
- Incomplete release leaving a residual tether (e.g. unsectioned thick filum) with persistent symptoms
The single most important complication to PREVENT is acute cord injury from operating on congenital scoliosis without a pre-operative whole-spine MRI. Distraction across a fixed septum can cause immediate, permanent paraplegia. MRI first, detether before you lengthen.
Guidelines, Registries & Global Practice
- SCM prevalence is consistent across ethnic groups; most series come from high-volume pediatric spine centers in North America, Europe, India and East Asia
- Congenital scoliosis association of 60-80 percent is reported from every major registry and is independent of geography
- Missed diagnosis remains the leading cause of catastrophic intraoperative cord injury in congenital deformity surgery worldwide
- High-resource centers: routine whole-spine MRI with contrast for every congenital curve; intraoperative ultrasound and neuromonitoring
- Limited-resource settings: MRI access may be delayed; plain film and clinical markers still drive referral, but outcomes suffer when imaging is unavailable
- Universal principle: any child with congenital scoliosis and a cutaneous marker or neurological asymmetry must reach an MRI-capable center before surgery
- MRI Indication
- Mandatory whole-spine MRI before any congenital scoliosis correction
- Surgical Sequence
- Detether and resect septum before or with deformity correction
- Registry Evidence
- No dedicated SCM registry; captured in congenital scoliosis databases
- MRI Indication
- MRI recommended for all congenital curves; urgent if cutaneous stigmata
- Surgical Sequence
- Neurosurgical input before orthopaedic correction
- Registry Evidence
- National registry data show reduced neurological complications with protocolized MRI
- MRI Indication
- MRI standard of care; CT for bony anatomy only
- Surgical Sequence
- Single-stage or staged release then correction
- Registry Evidence
- European registries emphasize avoidance of distraction across unrecognized tether
- MRI Indication
- High volume experience supports early prophylactic detether in asymptomatic SCM
- Surgical Sequence
- Combined neurosurgery-orthopaedics teams common
- Registry Evidence
- Large published series confirm safety of aggressive release protocols
There is no international SCM-specific registry. Data are derived from congenital scoliosis registries (NJR, AJRR, AOANJRR) and large single-center series. The consistent message across all sources is that preoperative MRI changes the operative plan in one-third of congenital scoliosis cases and prevents the majority of intraoperative neurological catastrophes.
Record in every congenital scoliosis patient:
- Presence or absence of cutaneous markers
- Neurological examination findings
- MRI performed (date, findings, who reviewed)
- Multidisciplinary discussion with neurosurgery
- Informed consent discussion of SCM risk
A missed SCM leading to postoperative paraplegia is a recurring source of claims worldwide. The standard of care in 2026 is full-spine MRI before booking the operating theatre.
Controversies & Areas of Uncertainty
Some centers advocate early release of every identified SCM even without deficit, arguing that growth or future surgery will eventually produce symptoms. Others observe selected asymptomatic patients with serial MRI and neurology. No randomized data exist; decision is individualized by age, curve magnitude, and family preference.
When both detethering and major osteotomy are required, some teams prefer two separate anesthetics to reduce operative time and blood loss. Others perform both in one sitting with two teams. Outcomes appear similar when neuromonitoring is used; choice depends on institutional resources and surgeon experience.
Ultrasound can confirm cord pulsation and free movement after release, but adds time and requires an open dural field. Its routine use is not universal; many experienced teams rely on direct visualization and neuromonitoring alone.
Rare adult presentations with new deficit after decades of compensation exist. Whether to operate on a stable adult with incidentally discovered SCM is controversial; most reserve surgery for progressive symptoms or when major spinal surgery is planned for other reasons.
MCQ Practice Points
Q: What is the key difference between Pang Type I and Type II split cord malformation? A: Type I has two separate dural sacs separated by a bony or cartilaginous septum; Type II has two hemicords within a single dural sac separated by a fibrous band only. The dural architecture and septum composition dictate the surgical approach and risk profile.
Q: When is MRI mandatory in a child with congenital scoliosis? A: Before any corrective surgery or even definitive bracing decision. Greater than 60 percent of congenital curves harbor occult SCM. An unrecognized bony septum can cause cord transection during distraction or osteotomy. Full-spine contrast MRI is the minimum standard.
Q: What cutaneous finding most strongly suggests split cord malformation? A: Hypertrichosis (hairy patch) over the lumbosacral spine. While not 100 percent sensitive, a hairy patch in a child with spinal deformity is an absolute indication for MRI. Other markers include dermal sinus, lipoma, and asymmetric gluteal cleft.
Q: Should detethering occur before, during, or after scoliosis correction? A: Before or at the same anesthetic as correction, never after. The cord must be free before any lengthening or derotation maneuver. Performing detethering after correction risks stretching an already injured cord across a residual septum.
Q: What additional finding is present in the majority of split cord cases and must be addressed surgically? A: Tethered cord from a thickened filum terminale or low conus. Even after septum resection, failure to section the filum leaves the cord under tension and allows late deterioration. Always inspect and release the filum at the same procedure.
Clinical Imaging
MRI Features of Split Cord Malformation
Split cord malformation is diagnosed exclusively on MRI. No plain film or CT finding replaces MRI. The study must include the entire spine from foramen magnum to sacrum because multiple levels or additional anomalies (syrinx, lipoma, dermal sinus) are common. Sagittal and axial T1- and T2-weighted sequences with contrast are standard. The key is to identify whether the hemicords lie within separate or shared dural sacs and whether a bony, cartilaginous or fibrous septum is present.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 9-year-old girl is referred with a 45-degree congenital thoracic scoliosis. On examination she has a prominent hairy patch over the lumbar spine. She has no neurological symptoms but her mother reports occasional bed-wetting. What is your next step and why?”
“A 12-year-old boy undergoes posterior instrumentation for congenital scoliosis. On the second postoperative day he develops bilateral leg weakness and urinary retention. Review of the preoperative workup shows no MRI was performed. What happened and how do you manage it now?”
Pang Classification
- Type I: two dural sacs, bony septum - resect bone and close dual tubes
- Type II: single dural sac, fibrous band - divide band only
- Both types frequently tethered by thick filum or scar
- Always release every tethering element at the index procedure
Cutaneous and Clinical Red Flags
- Hypertrichosis (hairy patch) is the strongest marker
- Asymmetric cavus feet or leg atrophy in a scoliotic child
- Early bladder dysfunction or recurrent UTI
- Any midline skin lesion below L1 demands MRI
Pre-Operative Mandate
- Full-spine contrast MRI in every congenital scoliosis case
- MRI changes surgical plan in greater than 30 percent of patients
- Never instrument or distract without MRI clearance
- Coordinate neurosurgery and spine teams before booking
Surgical Principles
- Position prone, expose one level above and below the split
- Resect bony septum under magnification protecting both hemicords
- Divide fibrous band and section thickened filum
- Confirm free cord movement before any spinal lengthening
Complications to Avoid
- Acute cord transection from distraction across unrecognized septum
- Incomplete release leaving residual tether
- CSF leak from difficult dural closure in Type I
- Late retether from scar formation
Evidence Base
Split cord malformation: Part I: A unified theory of embryogenesis for double spinal cord malformations
- Seminal paper establishing the embryologic basis for both Type I and Type II SCM from a single developmental error
- Described the spectrum of associated vertebral and cutaneous anomalies
- Provided the classification system still used worldwide for surgical decision-making
Split cord malformation: Part II: Clinical syndrome
- Detailed the clinical presentation, neurological deficits and associated anomalies in a large series of split cord cases
- Established that progressive deficit is the rule without surgical release of the septum and tether
- Provided the practical surgical decision framework still followed for Type I versus Type II lesions
Split cord malformations
- Review consolidating the unifying SCM classification: Type I = two dural sacs with a bony/fibrocartilaginous spur; Type II = a single dural sac with intradural fibrous bands
- The intervening mesenchymal elements tether the cord and drive progressive neurological, urological and orthopaedic deterioration
- The natural history supports an early, aggressive operative approach to untether the cord BEFORE clinical deterioration begins
Occult intraspinal anomalies and congenital scoliosis
- Of 251 patients with congenital scoliosis, occult intraspinal anomalies were found in 18.3% (46 patients); diastematomyelia was the commonest (41 patients)
- The risk was highly pattern-dependent: a unilateral unsegmented bar with a contralateral hemivertebra in the lower thoracic/thoracolumbar spine carried the highest rate (52%)
- Neural deterioration could be halted by excising the anomaly, supporting myelography (now MRI) in every congenital scoliosis case before correction