Bone-Preserving Humeral Fixation
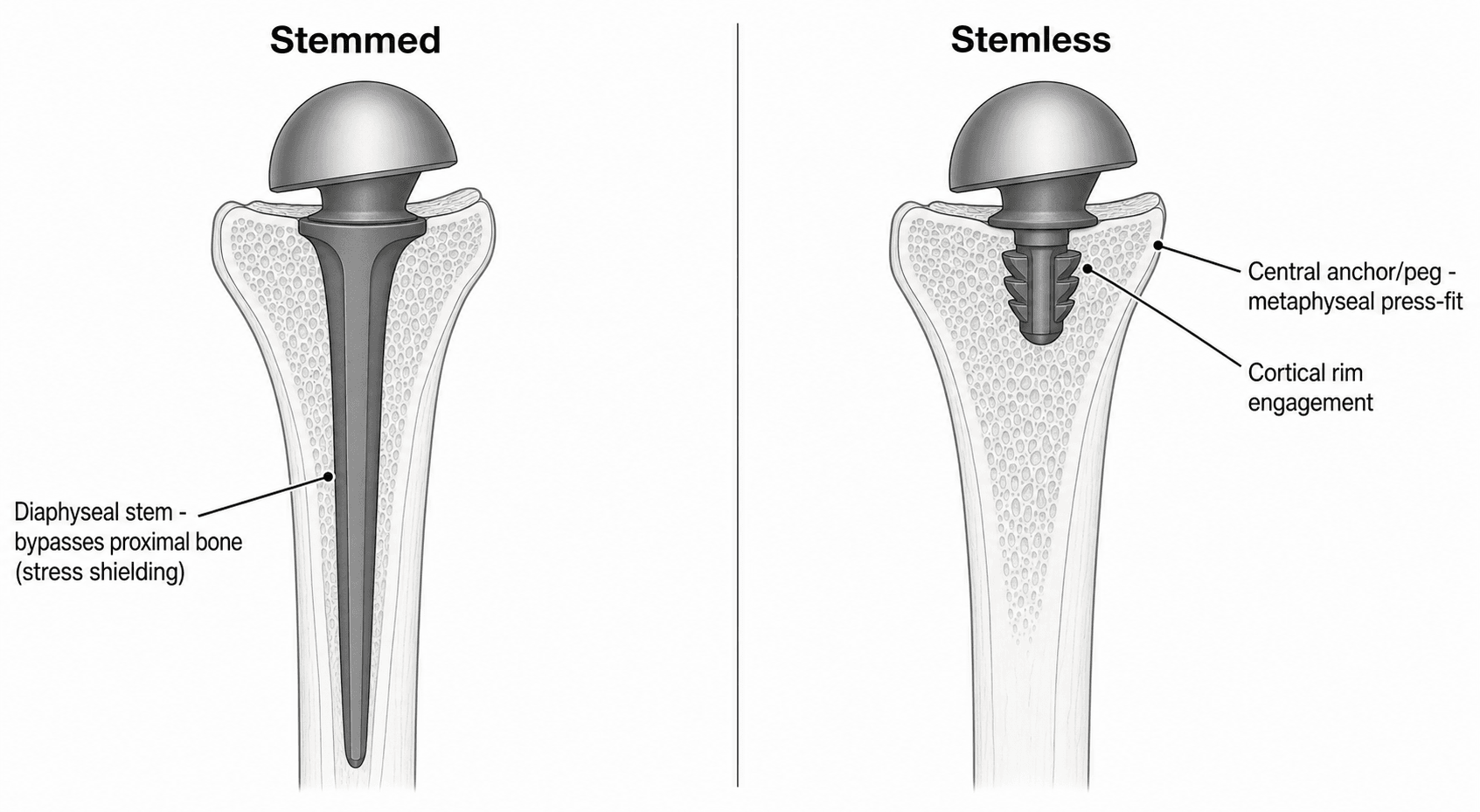
- In anatomic total shoulder arthroplasty the humeral component may be a STANDARD-length stem, a SHORT-STEM, or a STEMLESS implant, and there has been a clear TREND towards shorter and stemless components; a STEMLESS implant achieves fixation entirely in the proximal humeral METAPHYSIS (the cut humeral surface) with NO diaphyseal stem.
- The RATIONALE for short-stem and stemless designs is to PRESERVE humeral BONE STOCK (which makes any future revision easier), to DECREASE operative time, and to avoid the complications of a diaphyseal stem - periprosthetic humeral fracture, difficult stem extraction at revision, and STRESS SHIELDING, where a stiff diaphyseal stem unloads the proximal humerus and causes bony adaptation and radiolucent lines.
- The fundamental REQUIREMENT and limitation of a stemless implant is that, because fixation is metaphyseal, it depends on ADEQUATE proximal humeral BONE QUALITY; it is therefore contraindicated or avoided where the metaphyseal bone is poor - severe osteoporosis, large subchondral cysts, avascular necrosis with collapse, or significant deformity - in which a stemmed implant is used to gain diaphyseal fixation.
- CLINICAL OUTCOMES are broadly EQUIVALENT across stem lengths: comparative data show similar range of motion, patient-reported outcomes, complication and revision rates between standard-stem, short-stem and stemless components at short-to-mid term, with the practical advantages of shorter OPERATIVE TIME for the shorter components.
- RADIOGRAPHICALLY, the shorter components show LESS stress shielding: humeral radiolucent lines are significantly LESS frequent with stemless and short-stem than with standard-length stems (1.6% and 1.7% versus 11.9% in a series of 825), reflecting more physiological proximal load transfer. BUT THAT DIFFERENCE IS RADIOGRAPHIC AND HAS NOT TRANSLATED INTO A CLINICAL ONE: in the same series motion, PROMs, complications and revision did not differ by stem length, and in a New Zealand Joint Registry study of 3,952 patients there was NO significant difference in revision rate and NO humeral loosening in ANY group up to SEVEN YEARS. A radiolucent line is currently a marker of altered load transfer, not a demonstrated cause of failure - so argue for stemless on bone preservation, operative time and revision ease, NOT on survivorship.
- A major practical advantage is EASE OF REVISION: because the diaphysis and bone stock are preserved, a failed stemless/short-stem implant can be converted relatively straightforwardly to a stemmed (or reverse) implant; the trade-off is the dependence on bone quality and the need for longer-term survivorship data, so patient and bone selection is the key to using these implants well.
- “Stemless = METAPHYSEAL fixation only (no diaphyseal stem); short-stem = shortened stem. Trend is towards shorter components.
- “Rationale: preserve humeral BONE (ease revision), shorter operative time, avoid stem complications + STRESS SHIELDING. REQUIRES adequate metaphyseal bone quality (contraindicated in severe osteoporosis/cysts/AVN/deformity).
- “Outcomes comparable to stemmed (motion/PROMs/complications/revision) with FEWER radiolucent lines and shorter operative time; eases conversion to a stemmed implant at revision.
- “Registry (NZ, 3,952 patients, 7 years): revision per 100 component-years stemless 0.99 vs conventional 1.01 - no difference; NO humeral loosening in any group; no intra-operative humeral fracture in the stemless group.
- “The 1.6% vs 11.9% radiolucent-line gap is RADIOGRAPHIC - revision rates are equal. Do not convert it into a survivorship claim.
Stemless (metaphyseal fixation, no stem) preserves humeral bone, shortens operative time, avoids stem complications and stress shielding - and eases later revision to a stemmed implant.
Fixation is metaphyseal, so it needs adequate proximal humeral bone quality - avoid in severe osteoporosis, large cysts, AVN or deformity (use a stemmed implant).
Rationale, Requirement & Outcomes
Anatomic total shoulder arthroplasty can use a standard-length stem, a short-stem, or a stemless humeral component, and the trend is towards shorter components. A stemless implant fixes entirely in the proximal humeral metaphysis with no diaphyseal stem. The rationale is to preserve humeral bone stock (easing revision), shorten operative time, and avoid diaphyseal-stem problems - periprosthetic fracture, difficult stem removal, and stress shielding (proximal bony adaptation/radiolucent lines). The key requirement is adequate proximal humeral bone quality, so stemless is avoided in severe osteoporosis, large cysts, AVN or deformity. Clinically, outcomes (motion, PROMs, complications, revision) are broadly equivalent across stem lengths, with shorter operative time and fewer humeral radiolucent lines for the shorter components - though that radiolucent-line difference is radiographic and has not been matched by any difference in revision, with registry follow-up now reaching seven years and showing no humeral loosening in any group. Durability beyond that horizon is still being established.
- Standard stem
- Diaphyseal + metaphyseal
- Short-stem
- Short metaphyseal/proximal-diaphyseal
- Stemless
- Metaphyseal only
- Standard stem
- Least
- Short-stem
- Intermediate
- Stemless
- Most
- Standard stem
- Highest (~12%)
- Short-stem
- Low (~1.7%)
- Stemless
- Lowest (~1.6%)
- Standard stem
- Tolerates poorer bone (diaphyseal hold)
- Short-stem
- Needs reasonable bone
- Stemless
- Needs good metaphyseal bone
- Standard stem
- Longer / harder removal
- Short-stem
- Shorter / easier
- Stemless
- Shortest / easiest conversion
Selection & Revision
- Select by bone quality: stemless requires adequate proximal humeral metaphyseal bone - avoid it in severe osteoporosis, large subchondral cysts, AVN with collapse, or significant deformity, where a stemmed implant gains diaphyseal fixation.
- Reap the advantages: bone preservation, shorter operative time, and less stress shielding/fewer humeral radiolucent lines.
- Plan for revision: preserved bone stock makes conversion of a failed stemless/short-stem implant to a stemmed anatomic or reverse arthroplasty relatively straightforward.
- Counsel on the evidence: outcomes are comparable to stemmed implants and registry revision rates are equivalent out to seven years with no humeral loosening in any group; durability beyond that is still being established, so use stemless and short-stem in appropriately selected patients.
The single most important judgement with a stemless shoulder implant is bone quality: because the implant relies entirely on metaphyseal fixation in the proximal humerus, it must NOT be used where that bone is inadequate - severe osteoporosis, large subchondral cysts, avascular necrosis with collapse, or marked deformity - in which a stemmed implant is needed for diaphyseal fixation. Used in the right bone, stemless and short-stem implants give outcomes equivalent to stemmed designs with the genuine advantages of bone preservation, shorter operative time, less stress shielding and easier revision; used in poor bone they risk loosening. The other caveat is maturity of evidence: registry survivorship is equivalent to stemmed implants out to seven years with no humeral loosening recorded in any group, but durability beyond that horizon is still being established, so selection - the right implant for the right bone and patient - is the key to using these designs well.
How a Stemless Component Actually Anchors
Metaphyseal, press-fit fixation raises the obvious question of how the implant actually holds. A stemless humeral component anchors entirely in the proximal humeral metaphysis through a central fixation element seated in the cancellous bone of the cut surface - designs vary but it is typically a porous-coated cage or anchor, or a finned central peg / corolla (some add peripheral fins or a small central screw). Primary stability comes from a cementless press-fit/impaction into the cancellous bone together with engagement of the strong cortical rim of the humeral neck cut; secondary stability comes from bony on-/ingrowth (osseointegration) onto the porous surface.
The anchoring mechanism explains the rest. Because load is transferred through the metaphysis to the proximal humerus rather than bypassed down a diaphyseal stem, the proximal bone is loaded more physiologically - which is the mechanism behind the less stress shielding and the fewer radiolucent lines. And because the implant is impacted into (and preserves) the cancellous metaphyseal bone rather than reaming out a diaphyseal canal, the bone stock is preserved for any future revision. (The general biology of bone ingrowth is developed in Osseointegration.)
A stemless component anchors via a central cage / finned peg / corolla press-fit into metaphyseal cancellous bone with cortical-rim engagement (primary) plus osseointegration (secondary). Loading the metaphysis physiologically is why there is less stress shielding and fewer radiolucent lines, and impacting rather than reaming is why bone is preserved for revision.
Judging Bone Quality - and the Bail-Out to a Stem
Stemless implants need adequate bone quality and should be avoided in poor bone - so judging that, and knowing what to do if the bone disappoints, is the practical skill. Pre-operatively, suspect poor metaphyseal bone in severe osteoporosis, inflammatory arthritis, avascular necrosis, large subchondral cysts and deformity, and assess the proximal humerus on imaging.
Intra-operatively, after the humeral head cut, assess the exposed metaphyseal cancellous bone directly:
- The "thumb test" - if the cancellous bone compresses/indents easily under thumb pressure, it is too soft to hold a stemless anchor.
- Trial stability - a stemless trial that toggles or lacks rotational purchase signals inadequate fixation.
The safety principle is to be prepared to convert to a short-stem or stemmed implant intra-operatively if the bone is inadequate: consent for both, have the stemmed system available on the day, and never force a stemless into bone that will not hold it - forcing it risks the early loosening and subsidence that are the failure modes of metaphyseal fixation in poor bone. (General assessment of bone quality / osteoporosis is developed in Osteoporosis.)
Judge bone quality in theatre after the head cut: the thumb test (soft, easily-compressed cancellous bone fails) and a toggling trial mean inadequate fixation. Always consent and set up to convert to a stemmed implant, and never force a stemless into poor bone (early loosening/subsidence).
What the Registry Shows - and What the Radiolucent Lines Do Not
Seven-Year Registry Survivorship
Registry data now reach seven years, which is further than the short-to-mid-term comparative series. According to PubMed, a New Zealand Joint Registry study of the 12 most-used anatomic total shoulder arthroplasty implants followed 3,952 patients - 3,114 conventional stems, 360 short stems and 478 stemless - for revision up to seven years:
- n
- 3,114
- Revision per 100 component-years (95% CI)
- 1.01 (0.89 to 1.14)
- n
- 360
- Revision per 100 component-years (95% CI)
- 0.54 (0.25 to 1.03)
- n
- 478
- Revision per 100 component-years (95% CI)
- 0.99 (0.51 to 1.74)
No significant difference between the three, and that held irrespective of patient age or surgeon volume. Two further findings are worth carrying: there were no cases of humeral loosening in any group up to seven years, and no intra-operative humeral fractures in the stemless group - the latter being direct support for one of the stated reasons to avoid a diaphyseal stem.
The Radiolucent Lines Are Radiographic, Not Yet Clinical
The most quoted advantage of the shorter components is the radiographic one: humeral radiolucent lines in 1.6% of stemless and 1.7% of short-stem against 11.9% of standard stems. That difference is real, substantial and mechanistically explained by loading the metaphysis rather than bypassing it.
What it has not done is change the outcome that matters. In the same comparative series, range of motion, patient-reported outcomes, complications and revision rates did not differ by stem length; in the registry, revision rates were equivalent and there was no humeral loosening in any group at seven years. So a radiolucent line is currently a marker of altered load transfer, not a demonstrated cause of failure, and quoting the 1.6%-versus-11.9% contrast as though it were a survivorship advantage overstates it.
The honest position is that stress shielding may matter over a longer horizon than has yet been observed - which is precisely why standardised radiographic description of it has been called for - and that the case for stemless today rests on bone preservation, operative time and ease of revision rather than on a proven difference in implant survival.
Radiolucent lines are seven times commoner around a standard stem than a stemless one, and yet revision rates are the same and no humeral loosening appeared in any group by seven years. Both facts are true together. Argue for stemless on bone preservation, operative time and revision ease - not on survivorship, which the data do not currently show.
A Statistically Significant Difference That Is Not a Clinically Important One
The registry also found a better six-month Oxford Shoulder Score for stemless than conventional stems - 40.7 versus 39.4, p = 0.023. The p-value is real, but the gap is 1.3 points on a 48-point scale, which no patient would notice; with nearly 4,000 patients a trivial difference reaches significance easily. It is a useful worked example of the distinction between a significant result and an important one, and it should not be offered as a functional argument for the implant.
Mnemonics & Memory Aids
STEMLESS
Hook:STEMLESS: Shorter trend, Time reduced, Easier revision, Metaphyseal fixation, Less stress shielding, Equivalent outcomes, Selection by bone, Survivorship maturing.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What are stemless and short-stem shoulder implants, and why use them?”
“When would you NOT use a stemless implant, and what is the revision advantage?”
What they are
- Anatomic TSA humeral component: standard-stem, short-stem, or stemless
- Stemless = metaphyseal fixation only (no diaphyseal stem)
- Trend towards shorter components
Rationale
- Preserve humeral bone stock (ease revision)
- Shorter operative time
- Avoid stem complications (periprosthetic fracture, hard removal) and stress shielding
Requirement & evidence
- Needs adequate proximal humeral bone quality (metaphyseal fixation)
- Avoid in severe osteoporosis, large cysts, AVN with collapse, deformity (use stemmed)
- Outcomes comparable to stemmed; fewer radiolucent lines (~1.6% vs ~12%); shorter operative time
Revision
- Preserved bone -> straightforward conversion to stemmed/reverse implant
- Avoids difficult long-stem extraction
- Durability beyond 7 years still being established
Registry evidence (NZ, 3,952 patients, 7 years)
- Revision per 100 component-years: conventional 1.01, short 0.54, stemless 0.99 - no difference
- Held irrespective of patient age and surgeon volume
- NO humeral loosening in any group; no intra-operative humeral fracture in the stemless group
- Radiolucent lines 1.6% vs 11.9% is RADIOGRAPHIC - revision rates are equal
- Oxford Shoulder Score 40.7 vs 39.4 (p=0.023) - significant but 1.3 points, not clinically important
Evidence & Key Studies
Standard-stem vs short-stem vs stemless anatomic total shoulder arthroplasty: comparative outcomes
- Across 825 patients (standard, short-stem, stemless) at minimum 2-year follow-up, range of motion and patient-reported outcomes were similar, and complication and revision rates did not differ significantly.
- Operative time was shortest for stemless and short-stem; humeral radiolucent lines were significantly fewer with shorter components (1.6% stemless, 1.7% short-stem, 11.9% standard).
- Early data support stemless and short-stem humeral components for decreasing operative time and preserving humeral bone for potential revision, with longer-term durability studies still needed.
Stress shielding of the humerus in press-fit (short/stemless) anatomic shoulder arthroplasty
- Press-fit humeral stems, including short stems and stemless implants, were developed to decrease operative time, preserve bone stock and ease revision.
- Different press-fit designs alter proximal humeral stress distribution, and stress shielding manifests as bony adaptations that may affect long-term outcome and revision.
- Standardised radiographic descriptions of stress shielding are needed because varied classification systems complicate comparison of humeral fixation.
Medium-term results of stemless, short and conventional stem humeral components in anatomic total shoulder arthroplasty: a New Zealand Joint Registry study
- Registry study of the 12 most-used anatomic total shoulder arthroplasty implants in 3,952 patients (3,114 conventional, 360 short, 478 stemless) with revision followed to seven years.
- No significant difference in revision rate per 100 component-years - conventional 1.01 (95% CI 0.89-1.14), short 0.54 (0.25-1.03), stemless 0.99 (0.51-1.74) - and this held irrespective of patient age or surgeon volume.
- There were no cases of humeral loosening in any group up to seven years and no intra-operative humeral fractures in the stemless group; the six-month Oxford Shoulder Score was statistically higher for stemless (40.7 versus 39.4, p = 0.023), a 1.3-point difference on a 48-point scale.
The comparable clinical and functional outcomes across standard, short and stemless humeral components, the shorter operative time for shorter implants, and the lower humeral radiolucent-line rate with stemless and short-stem (1.6% and 1.7% against 11.9%) come from the cited Aibinder study of 825 patients at minimum two-year follow-up. The seven-year registry survivorship, the absence of humeral loosening in any group, the absence of intra-operative humeral fracture in the stemless group and the Oxford Shoulder Score comparison come from the cited Zhou New Zealand Joint Registry study of 3,952 patients. The rationale for press-fit short and stemless designs and the concept of stress shielding, including the call for standardised radiographic description of it, come from the cited Denard review, which is a technical review rather than a comparative study.
The distinction drawn between the radiographic and clinical findings follows directly from those two sources read together - a sevenfold difference in radiolucent lines alongside equivalent revision rates and no loosening by seven years - rather than from any study designed to test whether radiolucent lines predict failure; no such study was identified, which is why stress shielding is described as something that may matter over a longer horizon rather than something shown to cause revision. The judgement that a 1.3-point Oxford Shoulder Score difference is below clinical importance is an interpretation of the size of the effect, not a published minimal clinically important difference for that instrument.
The metaphyseal-fixation requirement, the contraindications in poor bone, the intra-operative thumb test and the readiness to convert are standard, well-established teaching; no dedicated topic covers stemless humeral components elsewhere in the library, and the parent Total Shoulder Arthroplasty page does not discuss stem length. (See also Shoulder Resurfacing Arthroplasty.)