& Subungual Tumours
- A subungual exostosis (Dupuytren's exostosis) is a BENIGN osteocartilaginous outgrowth - trabecular bone capped by FIBROCARTILAGE - that arises from the DORSAL or dorsomedial aspect of the DISTAL PHALANX, most commonly of the GREAT TOE, typically in adolescents and young adults, and a history of preceding TRAUMA is often present.
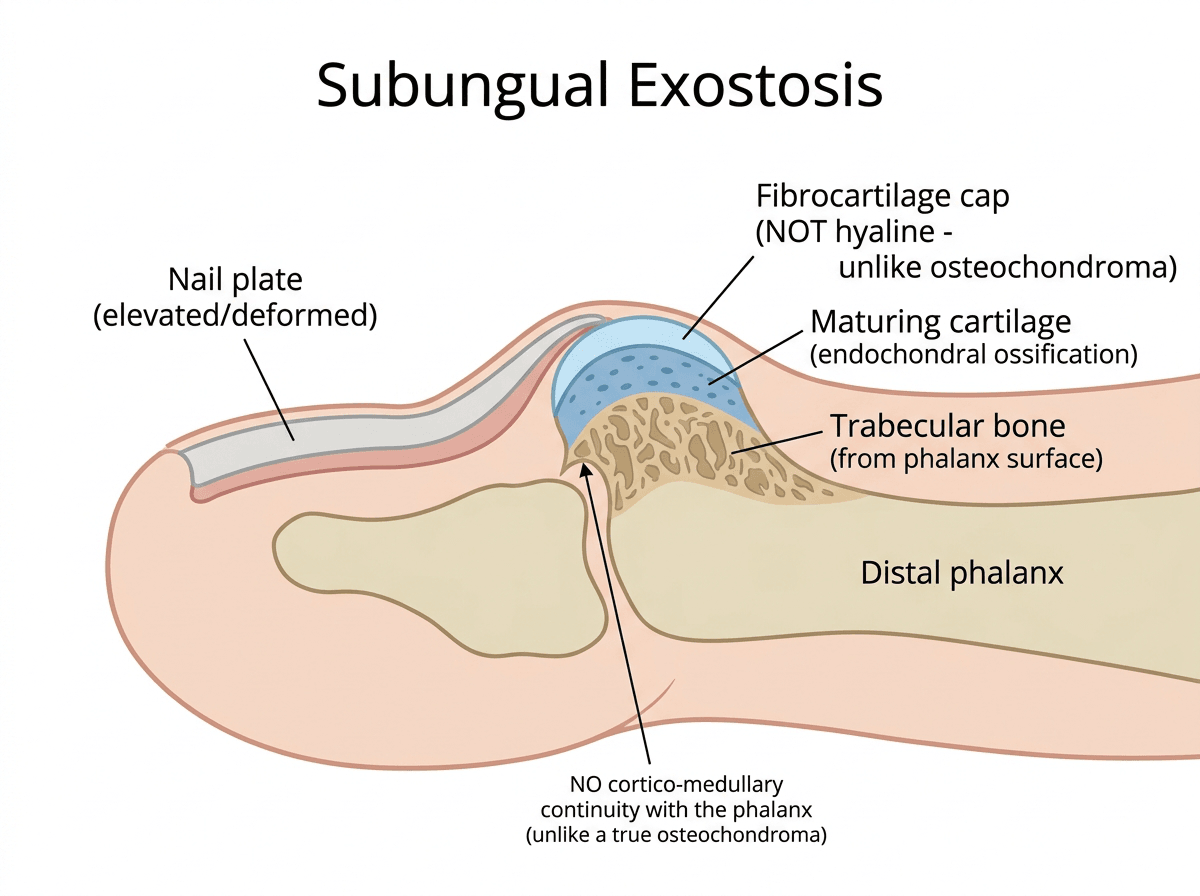
- It is histologically and radiologically DISTINCT from a true (hyaline-cartilage-capped) OSTEOCHONDROMA: a subungual exostosis has a FIBROCARTILAGE cap and does NOT show continuity of its cortex and medulla with the underlying bone (unlike an osteochondroma), and it arises from the surface of the distal phalanx rather than the metaphysis of a long bone.
- It PRESENTS as a firm subungual or periungual nodule that ELEVATES and DEFORMS the nail (onycholysis/nail-plate elevation), is often painful (especially with footwear pressure), and may ulcerate or bleed; the diagnosis is suggested clinically and confirmed on a plain RADIOGRAPH showing the bony outgrowth projecting from the distal phalanx.
- It must be considered within the broader differential of SUBUNGUAL TUMOURS, which includes benign solid lesions (glomus tumour - classically severe pain/cold sensitivity, subungual exostosis, soft-tissue chondroma, keratoacanthoma, haemangioma/pyogenic granuloma), benign cysts (epidermal/mucoid), and MALIGNANT tumours - squamous cell carcinoma and, crucially, subungual MELANOMA - so imaging (radiograph, and ultrasound/MRI for soft-tissue lesions) and a low threshold for biopsy are used to differentiate them.
- The MUST-NOT-MISS diagnosis is subungual MELANOMA: any persistent pigmented subungual lesion, a longitudinal melanonychia with Hutchinson's sign (pigment spread to the nail fold), or an atypical/non-healing subungual lesion must prompt suspicion and biopsy, because mis-diagnosing a melanoma as a benign subungual lesion is a catastrophic error - so a subungual mass is not assumed benign without appropriate assessment.
- RECURRENCE IS NOT PREDICTED BY THE FEATURES THAT LOOK MOST ALARMING. In 74 excised subungual exostoses and osteochondromas, AGE UNDER 18 was associated with recurrence, while SEX, DURATION OF SYMPTOMS, PRE-OPERATIVE PAIN, TUMOUR SIZE and DESTRUCTION OF THE NAIL PLATE had NO significant effect - so a large lesion, a long history or a badly damaged nail should not be used to stratify follow-up, whereas a skeletally immature patient should be followed and counselled as higher risk. In the same series a BURR appeared more effective than other techniques, which fits the principle that the retained cartilage cap is what recurs.
- COUNSEL WITH THE NUMBERS: about 85% of patients were satisfied with the procedure and close to 80% rated the cosmetic result good or very good. Worse satisfaction was strongly associated with recurrence, and separately with younger age and with the intensity of post-operative pain - so analgesia and expectation-setting are part of the outcome, not an afterthought.
- TREATMENT of a symptomatic subungual exostosis is MARGINAL EXCISION - removing the exostosis with its fibrocartilage cap down to its base on the distal phalanx (often with partial nail-plate removal for access) - and the key principle is COMPLETE excision, because an incompletely excised lesion (cartilage cap left behind) RECURS; histology should confirm the benign diagnosis.
- “Subungual exostosis (Dupuytren) = BENIGN FIBROCARTILAGE-capped bony outgrowth from the DORSAL DISTAL PHALANX, usually the great toe, in adolescents/young adults (often post-trauma) - elevates/deforms the nail.
- “Distinct from a true osteochondroma (fibrocartilage not hyaline cap; NO medullary continuity). Radiograph shows the outgrowth.
- “Part of the SUBUNGUAL TUMOUR differential (glomus, osteochondroma, pyogenic granuloma) - MUST EXCLUDE subungual MELANOMA/SCC. Treat by COMPLETE marginal excision (recurs if cartilage cap left).
- “Recurrence predictors (74 cases): AGE UNDER 18 yes; sex, symptom duration, pre-op pain, TUMOUR SIZE and nail-plate destruction NO. A burr appeared more effective than other techniques.
- “Outcome figures for consent: ~85% satisfied, ~80% good/very good cosmesis; worse satisfaction tracks recurrence, younger age and post-op pain.
A fibrocartilage-capped bony outgrowth from the dorsal distal phalanx (usually the great toe) that elevates/deforms the nail - confirmed on radiograph. Treat by complete marginal excision.
Any subungual mass sits in a differential that includes subungual MELANOMA and SCC - a pigmented/ atypical/non-healing lesion must prompt biopsy.
Pathogenesis: Trauma, Metaplasia and the Zonal Histology
The lesion is trabecular bone capped by fibrocartilage, and trauma is often implicated - one mechanism ties those together and explains the histology.
The prevailing model is reactive: trauma or chronic irritation (hence the post-trauma history and the pressure-exposed great toe) provokes proliferation of cartilage at the periosteal surface, which then undergoes endochondral ossification to lay down trabecular bone. The lesion therefore grows from a proliferating cartilage cap downward into mature bone. A recurrent chromosomal translocation has also been reported in these lesions, which would suggest a neoplastic rather than purely reactive element - though the two models are not mutually exclusive, and trauma may act on a lesion that is already clonal.
From base to surface: a deep zone of mature trabecular bone arising from the distal-phalanx surface; a middle zone of maturing cartilage undergoing endochondral ossification; and a superficial fibrocartilage / proliferating fibroblastic cap. This is why the cap is fibrocartilage (not the hyaline cap of a true osteochondroma), why there is no cortico-medullary continuity, and why an early, cellular lesion can look alarming.
Diagnosis, Excision & Exclusion of Malignancy
- Diagnose: clinical (firm subungual nodule deforming the nail, often great toe, often post-trauma) plus a plain radiograph showing the bony outgrowth from the distal phalanx; ultrasound/MRI help for soft-tissue subungual lesions.
- Exclude malignancy: a subungual mass is part of a differential that includes melanoma and SCC - a pigmented, atypical, ulcerated or non-healing lesion (especially with Hutchinson's sign) needs BIOPSY.
- Treat by complete marginal excision: remove the exostosis with its fibrocartilage cap down to its base (with partial nail-plate removal for access); send for histology.
- Avoid recurrence: incomplete excision (cartilage cap left) is the main cause of recurrence - excise completely.
- Manage the nail: preserve/repair the nail bed where possible to minimise nail deformity.
The crucial safety principle for any subungual lesion is to exclude malignancy - above all subungual MELANOMA - before treating it as a benign subungual exostosis. While the subungual exostosis is a common, benign, fibrocartilage-capped bony outgrowth of the distal phalanx that is confirmed on radiograph and cured by complete marginal excision, the subungual space also harbours dangerous tumours, and a pigmented subungual lesion, a longitudinal melanonychia with Hutchinson's sign (pigment spreading to the nail fold), or an atypical, ulcerated or non-healing subungual lesion must raise suspicion of melanoma or squamous cell carcinoma and prompt biopsy. Equally, when excising a subungual exostosis, removing the lesion completely with its cartilage cap is what prevents recurrence, and the specimen should always go for histology to confirm the benign diagnosis.
The Lesion, Its Differential & Treatment
A subungual exostosis (Dupuytren's exostosis) is a benign osteocartilaginous outgrowth - trabecular bone capped by fibrocartilage - arising from the dorsal/dorsomedial distal phalanx, most often the great toe, in adolescents/young adults, often after trauma. It is distinct from a true osteochondroma (fibrocartilage rather than hyaline cap; no continuity with the medullary canal). It presents as a firm subungual nodule that elevates and deforms the nail, is often painful and may ulcerate, and is confirmed on a plain radiograph. Crucially it sits within the subungual tumour differential - glomus tumour (severe pain/cold sensitivity), osteochondroma, soft-tissue chondroma, pyogenic granuloma, and the must-not-miss subungual MELANOMA and squamous cell carcinoma - so a subungual mass is not assumed benign. Treatment is complete marginal excision (with the cartilage cap); incomplete excision recurs.
- Clue
- Bony outgrowth on radiograph; nail elevation; great toe
- Note
- Benign; fibrocartilage cap; marginal excision
- Clue
- Severe pinpoint pain, cold sensitivity, blue-red nail-bed spot
- Note
- Benign; MRI; excision
- Clue
- Bony outgrowth with medullary continuity
- Note
- Benign; differs from exostosis (hyaline cap, continuity)
- Clue
- Friable, bleeding/rapid lesion
- Note
- Benign but mimics malignancy
- Clue
- Pigment, Hutchinson's sign, non-healing/atypical lesion
- Note
- MALIGNANT - must not miss; biopsy
Operative Technique and Outcomes
Complete marginal excision including the cartilage cap is the operation, and incomplete removal recurs - so both the technique and the outcomes the patient should be counselled about matter.
- Under tourniquet/ring block, avulse or partially remove the overlying nail plate for access; a dorsal or distal "fishmouth" incision exposes the lesion.
- Excise the exostosis at its base on the distal phalanx (osteotome/rongeur down to the cortex) and - critically - remove the entire fibrocartilage cap, because the retained cap is the source of recurrence. Send the specimen for histology to confirm the benign diagnosis (and exclude malignancy).
- Preserve and repair the nail bed/matrix where possible to limit nail deformity; the nail plate regrows over months.
- Counsel: complete excision is curative with low recurrence; an incompletely excised cap recurs; warn about possible transient nail-plate deformity and the small recurrence risk, with follow-up to confirm resolution.
The operation is nail-plate access -> excise at the base -> remove the whole fibrocartilage cap -> histology. The retained cartilage cap is what recurs, so completeness (not width) is the goal; protect the nail bed to limit deformity.
What Actually Predicts Recurrence - and What Does Not
Completeness of excision is the surgical principle, but it is not the only thing that determines whether a lesion comes back, and several factors a clinician might reasonably expect to matter turn out not to.
A retrospective study of 74 patients who underwent dorsal-approach excision of a subungual exostosis or subungual osteochondroma, reviewed at a minimum of six months:
- Association with recurrence
- ASSOCIATED with recurrence
- Association with recurrence
- No significant effect
- Association with recurrence
- No significant effect
- Association with recurrence
- No significant effect
- Association with recurrence
- No significant effect
- Association with recurrence
- No significant effect
The practical readings are that a skeletally immature patient carries the higher recurrence risk and should be followed and counselled accordingly, and that a big lesion, a long history or a badly damaged nail do not by themselves predict a return - so they should not be used to stratify follow-up. Note that the series pooled subungual exostosis with subungual osteochondroma, which are related but not identical lesions.
Technique and What the Patient Can Expect
The same series found that the technique using a burr appeared more effective than the alternatives, which sits naturally with the principle that the retained cartilage cap is the source of recurrence - a burr takes the base flush to the phalangeal cortex in a way an osteotome and rongeur may not.
For counselling, it supplies the figures the operation otherwise lacks: 85% of patients were satisfied with the procedure and close to 80% rated the cosmetic result good or very good. Worse satisfaction was strongly associated with recurrence - and, separately, with younger age and with the intensity of post-operative pain, which is a reminder that analgesia and expectation-setting are part of the result.
Recurrence is not predicted by the things that look most alarming. Age under 18 was associated with recurrence, while sex, symptom duration, pre-operative pain, tumour size and nail-plate destruction were not. A burr appeared more effective than other techniques, consistent with the retained cartilage cap being what recurs. Counsel with the numbers: about 85% satisfied, nearly 80% good or very good cosmesis.
Mnemonics & Memory Aids
NAIL
Hook:NAIL: Nodule deforms nail, Adolescent/post-trauma fibrocartilage cap, Image + exclude malignancy, Lesion excised completely.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A teenager has a painful firm lump under the great toenail that is lifting the nail. What is the likely diagnosis and how do you approach it?”
Subungual exostosis
- Benign osteocartilaginous outgrowth, fibrocartilage cap
- Dorsal/dorsomedial distal phalanx, usually great toe; adolescents/young adults (often post-trauma)
- Elevates/deforms the nail; painful; confirm on radiograph
Vs true osteochondroma
- Subungual exostosis: fibrocartilage cap, NO medullary continuity, surface of distal phalanx
- Osteochondroma: hyaline cap, cortical/medullary continuity, long-bone metaphysis
- Distinct entities
Subungual tumour differential
- Benign: glomus tumour (severe pain/cold), exostosis, chondroma, pyogenic granuloma, keratoacanthoma
- Malignant (must not miss): subungual MELANOMA, squamous cell carcinoma
- Pigmented/atypical/non-healing/Hutchinson's sign -> biopsy
Treatment
- Complete marginal excision (with fibrocartilage cap) - send histology
- Incomplete excision -> recurrence; a burr appeared more effective than other techniques
- Preserve/repair the nail bed where possible
Recurrence & outcomes (74 excisions)
- PREDICTS recurrence: age under 18
- Does NOT predict: sex, symptom duration, pre-op pain, tumour size, nail-plate destruction
- ~85% satisfied; ~80% good or very good cosmetic result
- Worse satisfaction tracks recurrence, younger age and post-operative pain
- Series pooled subungual exostosis with subungual osteochondroma; no overall recurrence rate given
Evidence & Key Studies
Subungual tumours: clinicopathologic correlation with US and MR imaging (differential)
- Subungual tumours include benign solid lesions (glomus tumour, subungual exostosis, soft-tissue chondroma, keratoacanthoma, haemangioma), benign cystic lesions, and malignant tumours (squamous cell carcinoma, malignant melanoma).
- Imaging is important because of the small size, nonspecific clinical manifestations and functional significance of these lesions; ultrasound and MRI help characterise and differentiate them.
- Accurate diagnosis requires correlation of imaging with clinical and pathological findings.
Florid reactive periostitis ossificans of the humerus: differential of benign vs malignant periosteal/surface bone lesions (incl. subungual exostosis)
- Reactive/benign surface bone lesions - including subungual exostosis, bizarre parosteal osteochondromatous proliferation (Nora's lesion) and florid reactive periostitis - show imaging/histological overlap with each other and with malignant surface tumours (periosteal/parosteal osteosarcoma).
- It is important to recognise the benign entities so they are not mistaken for an aggressive neoplasm.
- A correct diagnosis (and benign vs malignant distinction) guides appropriate, conservative management.
The influence of clinical factors on treatment outcome and recurrence of surgically removed subungual osteochondroma and subungual exostosis
- Retrospective review of 74 patients who had a subungual exostosis or subungual osteochondroma removed through a dorsal approach under digital anaesthesia, assessed at a minimum of six months by questionnaire and photographs.
- Age under 18 was associated with recurrence, while sex, duration of symptoms, pre-operative pain, tumour size and destruction of the nail plate had no significant effect on it; the technique using a burr appeared more effective.
- Eighty-five per cent of patients were satisfied and nearly 80% rated the cosmetic effect good or very good; worse satisfaction was strongly associated with recurrence, and also with younger age and post-operative pain intensity.
The differential of subungual tumours (including the subungual exostosis among benign solid lesions, alongside the malignant squamous cell carcinoma and melanoma) and the role of imaging in differentiating them come from the cited Baek review; the imaging and histological overlap of benign surface bone lesions with malignant surface tumours, and the importance of not mistaking benign lesions for aggressive neoplasms, from the cited Soni review. The recurrence predictors and non-predictors, the comparative note on the burr, and the satisfaction and cosmetic figures come from the cited Dabrowski series of 74 patients, which pooled subungual exostosis with subungual osteochondroma - related but not identical lesions - and reported no overall recurrence percentage, so none is quoted here.
The reported recurrent chromosomal translocation is left unspecified because no citation confirming which translocation it is could be identified, and naming one on recollection would be worse than leaving the point general. The subungual exostosis being a benign fibrocartilage-capped outgrowth of the distal phalanx, usually the great toe and often post-traumatic, its distinction from a true osteochondroma, the nail deformity, the must-not-miss melanoma, and complete marginal excision are standard, well-established teaching. (See also Subungual Melanoma, Glomus Tumour and Osteochondroma; a grep of the osteochondroma page finds no discussion of the subungual lesion, so the distinction between the two is drawn here.)