Dislocation + Radial Head + Coronoid | LCL Always Torn | Address All Components
- All three components (bone and soft tissue) must be addressed for stability
- LCL repair is essential - always torn in posterior dislocation mechanism
- Radial head must be fixed or replaced (never excise)
- Coronoid tip fractures may not need fixation but LCL repair critical
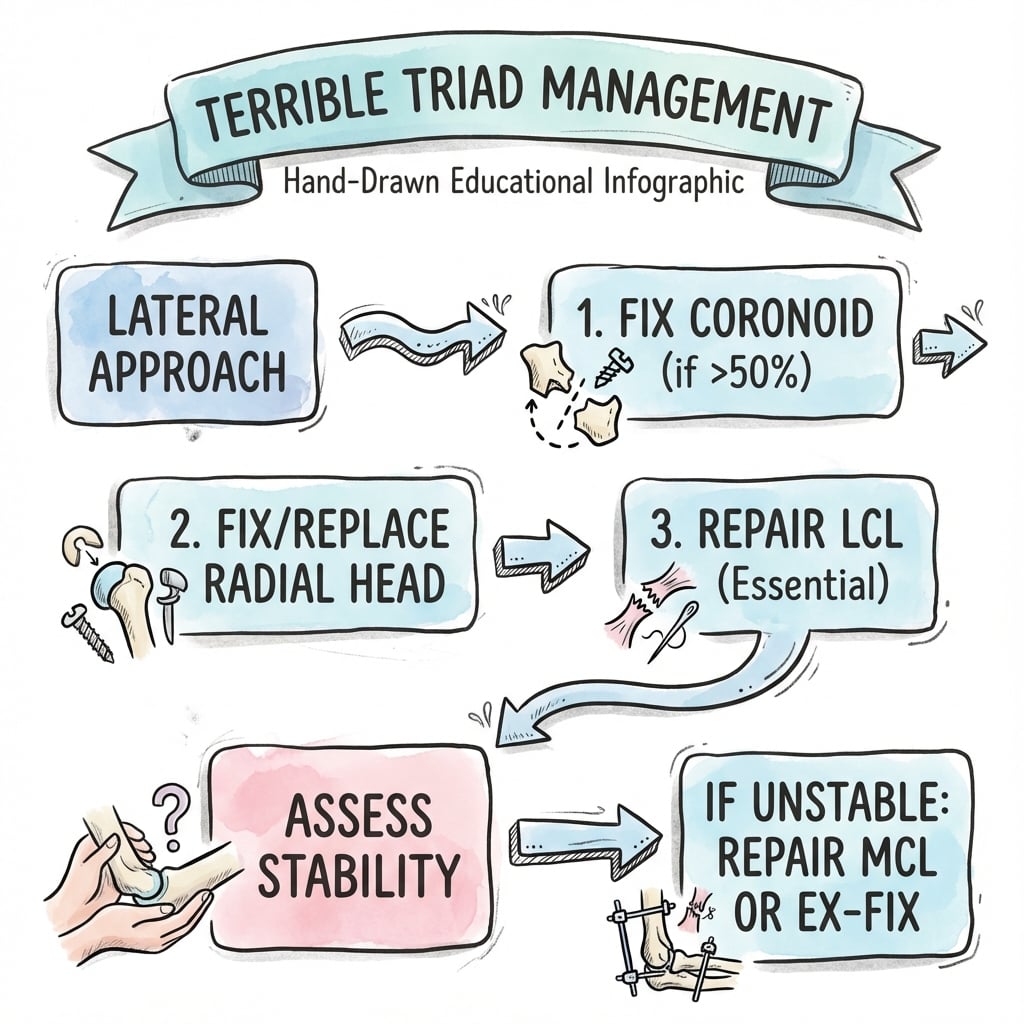
- Surgical sequence: coronoid first, radial head, LCL repair, assess MCL
- “Terrible triad = dislocation + radial head + coronoid + LCL rupture
- “Coronoid is anterior buttress - prevents posterior subluxation
- “LUCL is key component of LCL - originates from lateral epicondyle
- “Redislocation rate high if components not all addressed
Four structures need treatment: coronoid, radial head, LCL (always), and sometimes MCL. Undertreating any component leads to recurrent instability. This is a pattern, not just a radial head fracture.
The LCL (especially LUCL) is always torn in posterior dislocations. It is the primary lateral stabilizer. Must be repaired through bone tunnels or suture anchors even if coronoid is just a tip fracture.
The coronoid is the anterior buttress against posterior subluxation. More than 50% coronoid fracture or anteromedial facet fracture requires fixation. Tip fractures may be stable with LCL repair.
Never excise the radial head in terrible triad. It is a secondary stabilizer in the MCL-deficient elbow. Fix (3 or fewer fragments) or replace (more than 3 fragments).
- Component
- Coronoid fracture
- Decision
- Assess size and type
- Options
- Tip only: LCL may suffice. More than 50%: fix through lateral or anterior
- Component
- Radial head
- Decision
- Reconstruct or replace
- Options
- 3 or fewer fragments: ORIF. More than 3: arthroplasty
- Component
- LCL repair
- Decision
- Always required
- Options
- Suture anchors or bone tunnels to isometric point
- Component
- Assess stability
- Decision
- Test through arc of motion
- Options
- Stable: proceed. Unstable: consider MCL repair or hinged ex-fix
- Component
- MCL (if needed)
- Decision
- Only if unstable after lateral repair
- Options
- Medial approach, repair to sublime tubercle
TRIADTRIAD - The Three Components
Hook:TRIAD reminds you of all components - don't forget the LCL is the fourth structure
LUCLLUCL - Lateral Collateral Structure
Hook:The LUCL is the key structure in the LCL complex - always repair it
5050-25-4 Rule
Hook:These numbers guide surgical decision-making in terrible triad
Overview and Epidemiology
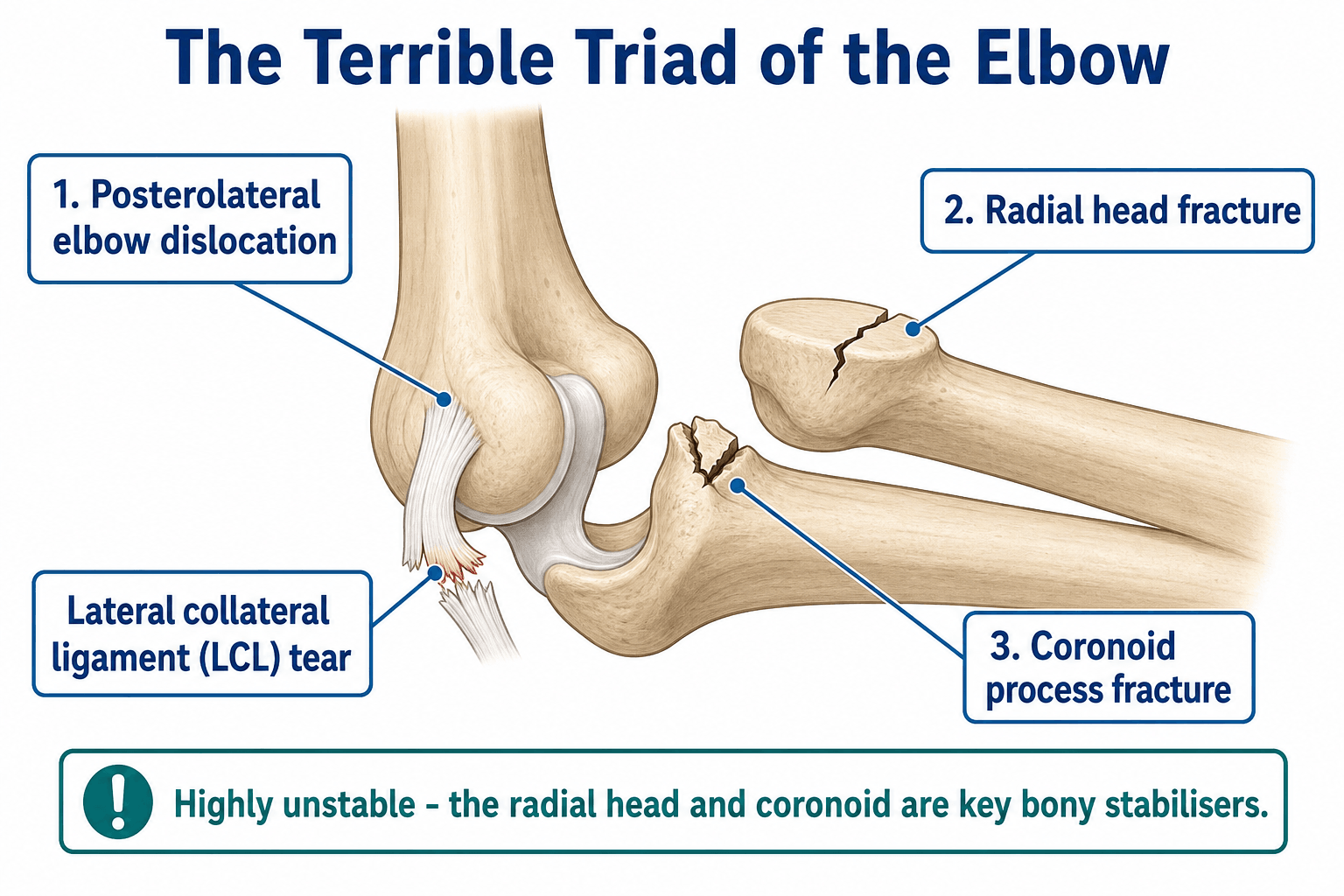
The terrible triad of the elbow describes the combination of posterior elbow dislocation, radial head fracture, and coronoid process fracture. The term "terrible" reflects the historically poor outcomes when these injuries were undertreated.
Mechanism of injury:
- Fall on outstretched hand with elbow in extension
- Axial load combined with valgus and supination moment
- Posterior dislocation occurs first
- Coronoid impacts on trochlea during reduction attempts
- Radial head impacts capitellum
Historical outcomes were poor because the soft tissue components (especially LCL) were not recognized or addressed. Modern understanding that this is a pattern of instability requiring treatment of all components has improved outcomes significantly.
The four lesions:
- Posterior elbow dislocation
- Radial head fracture (Mason Type IV by definition)
- Coronoid fracture
- LCL rupture (always present but historically under-recognized)
Anatomy and Biomechanics
Elbow stability:
The elbow is one of the most stable joints due to:
- Primary stabilizers: ulnohumeral articulation, MCL (anterior bundle), LCL complex
- Secondary stabilizers: radial head, common flexor/extensor origins, joint capsule
Lateral collateral ligament complex:
- LUCL (Lateral Ulnar Collateral Ligament) - key structure, resists posterolateral rotatory instability
- RCL (Radial Collateral Ligament) - lateral epicondyle to annular ligament
- Annular ligament - encircles radial head
The LUCL is the primary restraint to posterolateral rotatory instability (PLRI). It originates from the lateral epicondyle (isometric point) and inserts on the supinator crest of the ulna. In terrible triad, the LUCL is always ruptured and must be repaired.
- Anterior buttress against posterior subluxation
- Insertion point for anterior MCL bundle
- Anteromedial facet - key for varus-posteromedial instability
- Secondary valgus stabilizer
- Becomes critical when MCL is deficient
- Contributes to longitudinal forearm stability
Think of elbow stability as a ring: MCL + coronoid + radial head + LCL. Breaking the ring at two or more points creates instability. In terrible triad, the ring is broken at multiple points - all must be addressed.
Classification Systems
Regan-Morrey Classification (simple)
- Description
- Tip fracture
- Involvement
- Less than 10% height
- Description
- Less than 50% of process
- Involvement
- 10-50% height
- Description
- More than 50% of process
- Involvement
- More than 50% height
O'Driscoll Classification (more comprehensive)
- Description
- Tip fractures (subtype 1 = less than 2mm, subtype 2 = more than 2mm)
- Description
- Anteromedial facet fractures (subtypes based on extension)
- Description
- Basal fractures (subtypes based on extension)
Anteromedial facet fractures (O'Driscoll Type 2) are associated with varus-posteromedial rotatory instability, a different pattern from terrible triad. Important to distinguish as treatment differs.
Clinical Presentation and Assessment
History:
- Mechanism (FOOSH, sports, MVA)
- Any sense of the elbow "going out"
- Previous elbow problems
- Hand dominance, occupation
Physical examination:
- Significance
- Dislocation still present
- Action
- Reduce urgently
- Significance
- Significant injury
- Action
- Assess skin, neurovascular status
- Significance
- LCL injury, radial head fracture
- Action
- Part of the triad
- Significance
- Possible MCL involvement
- Action
- May need medial repair
- Significance
- Unstable pattern
- Action
- Surgical stabilization required
- Significance
- Nerve or vessel injury
- Action
- Document, urgent assessment
Post-reduction assessment:
- Test stability through ROM (under anesthesia if needed)
- Note angle at which re-dislocation occurs
- Valgus stress (MCL) and varus stress (LCL)
- Posterolateral rotatory stress
After closed reduction, test stability through full arc of motion. If the elbow redislocates before 30-45 degrees of extension, it is highly unstable and requires urgent surgical stabilization.
Neurovascular examination:
- Ulnar nerve (most commonly affected - up to 20%)
- Median nerve
- Radial nerve/PIN
- Brachial artery (rare but serious)
Differential diagnosis
Several elbow fracture-dislocation patterns share radiographic features with the terrible triad but have different mechanisms and treatment. Distinguishing them is a classic viva trap.
- Key components
- Posterior dislocation + radial head + coronoid tip + LCL tear
- Mechanism / distinguishing feature
- Posterolateral rotatory; coronoid is a transverse TIP fragment
- Treatment difference
- Lateral approach, fix/replace radial head, repair LCL
- Key components
- Anteromedial facet + LCL injury, radial head usually intact
- Mechanism / distinguishing feature
- Varus posteromedial rotatory; fragment is the medial facet, not the tip
- Treatment difference
- Medial buttress plate; radial head often spared
- Key components
- Olecranon/proximal ulna fracture + coronoid, radial head often intact
- Mechanism / distinguishing feature
- Trochlear notch disrupted; ulnohumeral apposition lost posteriorly
- Treatment difference
- Restore trochlear notch with dorsal plate
- Key components
- LCL (and variable MCL) tear only, no fracture
- Mechanism / distinguishing feature
- Stable concentric reduction; redislocates only in extreme extension
- Treatment difference
- Closed reduction, early motion, rarely surgery
- Key components
- Radial head fracture without dislocation or coronoid injury
- Mechanism / distinguishing feature
- No instability; concentric joint on all views
- Treatment difference
- ORIF or replacement of the head alone
Investigations
- AP and lateral elbow (confirm dislocation, identify fractures)
- May be limited by patient pain
- AP and lateral (confirm reduction, assess fractures)
- Assess concentric reduction
- Look for radial head and coronoid fractures
- All terrible triad injuries should have CT
- Assess coronoid fragment size (percentage of height)
- Assess radial head (fragment number, reconstructability)
- Look for loose bodies
- 3D reconstruction helpful for visualization
CT scan is mandatory before surgery. It allows accurate assessment of coronoid fragment size (determines if fixation needed) and radial head fragments (determines ORIF vs arthroplasty). Don't operate without CT.
Key CT findings to document:
- Coronoid: percentage of height involved, fragment type
- Radial head: number of fragments, reconstructability
- Associated injuries (capitellum, medial epicondyle)
- Loose bodies in joint
Management
Emergency department:
- Closed reduction of elbow (usually in ED under sedation)
- Post-reduction X-rays
- Splint at 90 degrees
- Assess stability (may defer to OR if too painful)
- CT scan for surgical planning
Terrible triad injuries require surgical intervention. Do not discharge with plan for delayed surgery. Recurrent instability, stiffness, and heterotopic ossification increase with delay.
Although the default is operative, a small subset can be managed non-operatively, and this is the answer to the classic viva follow-up. The criteria for a trial of non-operative care are strict: a small or minimally displaced radial head fracture that does not block forearm rotation, a small coronoid (tip) fragment, and — the decisive test — a concentric, stable reduction maintained through a functional arc of motion (typically extension to about 30 degrees) confirmed on examination and live fluoroscopy, with the ulnohumeral and radiocapitellar joints congruent. Such patients are mobilised early in a hinged brace blocking terminal extension, with close weekly radiographs for the first 2-3 weeks to detect any subluxation (watch for the drop sign / ulnohumeral widening). Any loss of concentric reduction, a block to motion, or a larger fragment mandates conversion to surgery — the threshold to operate stays low because missed instability does badly.
Surgical Technique
Lateral approach (Kocher or extended lateral) is standard.
- Interval between anconeus and ECU
- Identify and protect LCL origin
- Excellent access to radial head and lateral coronoid
- Extension of Kocher
- Better access to coronoid through radial head defect
- Can split common extensor origin
- Do not detach LCL from epicondyle (it's already torn)
- Use torn LCL as a window
- Identify LUCL for later repair
Working through the existing disruption avoids further soft tissue damage and maintains surgical exposure.


SEQUENCESEQUENCE - Surgical Order
Hook:SEQUENCE keeps you on track - coronoid, radial head, LCL, then assess stability
Complications
- Incidence
- 5-15% (modern techniques)
- Prevention/Management
- Address all components, adequate LCL repair
- Incidence
- 20-40%
- Prevention/Management
- Early motion, avoid over-immobilization
- Incidence
- 10-20%
- Prevention/Management
- Indomethacin prophylaxis, early motion
- Incidence
- 10-30%
- Prevention/Management
- Anatomic reduction of articular surfaces
- Incidence
- 10-15%
- Prevention/Management
- Careful retraction, may need transposition
- Incidence
- 5-10%
- Prevention/Management
- Adequate fixation, hardware removal if symptomatic
- Incidence
- Rare (less than 5%)
- Prevention/Management
- Adequate fixation, bone graft if at-risk
- Most serious complication
- Usually due to undertreated components
- Prevention: meticulous surgical technique addressing all structures
- Treatment: revision surgery, may need hinged ex-fix
- Very common after complex elbow trauma
- Goal: functional arc (30-130 degrees)
- Prevention: early motion (within first week)
- Treatment: physiotherapy, dynamic splinting, surgical release
Heterotopic ossification (HO) is common in terrible triad. Consider prophylaxis with indomethacin 75mg/day for 2-3 weeks or single-dose radiation. Early motion also reduces HO risk.
Postoperative Care and Rehabilitation
Post-surgical protocol:
- Posterior splint at 90 degrees
- Elevation, ice
- Wound monitoring
- Finger motion encouraged
- Remove splint, begin ROM
- Active and active-assisted motion
- May use hinged brace if stability concerns
- Avoid terminal extension if any instability
- Progressive ROM
- Goal: functional arc by 6 weeks
- Dynamic splinting if stiff
- Avoid varus stress and forced extension
- Begin pronation/supination as tolerated
- Full active ROM expected
- Begin gentle strengthening
- Progressive loading
- Wean from brace if used
- Progressive strengthening
- Return to work (desk work earlier)
- Sports depending on demands
- May take 6-12 months for full recovery
Key rehabilitation principles:
- Early motion is critical but must balance with stability
- Avoid varus stress (stresses LCL repair)
- Hinged brace allows motion while limiting terminal extension
- Patient education about activity restrictions
- Long-term outcome depends heavily on rehabilitation compliance
Outcomes and Prognosis
Outcomes with modern treatment:
Modern understanding and treatment of all components has dramatically improved outcomes compared to historical series.
- Good/Excellent
- 40-50%
- Key Issues
- Undertreatment of soft tissues
- Good/Excellent
- 70-85%
- Key Issues
- All components addressed
Prognostic factors:
- Coronoid fragment size (larger = worse prognosis)
- Quality of repairs
- Associated injuries (MCL, capitellum)
- Time to surgery (delay increases stiffness and HO)
- Patient compliance with rehabilitation
The key to good outcomes is recognizing this as a pattern of instability and addressing all components: coronoid (fix if significant), radial head (fix or replace), LCL (always repair). Undertreating any component leads to poor results.
Guidelines, Registries & Global Practice
Global epidemiology
The terrible triad is a subset of elbow fracture-dislocation, so its frequency tracks elbow dislocation epidemiology. Population data are consistent across continents.
- Measure
- Elbow dislocation incidence
- Figure
- 5.21 per 100,000 person-years
- Measure
- Peak age / mechanism
- Figure
- 10-19 years; ~45% sports-related
- Measure
- Elbow dislocation incidence
- Figure
- 7.7 per 100,000 per year
- Measure
- Dislocations with concomitant fracture
- Figure
- ~17%
According to PubMed, US NEISS data (Stoneback et al., DOI) give an elbow dislocation incidence of 5.21 per 100,000 person-years, peaking in adolescent males and largely sports-related, while a Taiwanese nationwide cohort (Yang et al., DOI) reports 7.7 per 100,000 per year with roughly one in six dislocations carrying an associated fracture. The terrible triad sits at the severe end of this complex-dislocation group.
Guidance across regions (principles converge)
There is no single randomised-trial-based guideline for the terrible triad; recommendations rest on the Pugh/King protocol and consistent expert consensus. The principles are essentially uniform worldwide.
- Position on the terrible triad
- Operative stabilisation as default; fix or replace radial head, address coronoid, repair LCL, then reassess; hinged fixation as salvage
- Evidence level
- Expert consensus / Level V
- Position on the terrible triad
- Early specialist (upper-limb) referral and operative management; CT before surgery; early mobilisation
- Evidence level
- Consensus / Level V
- Position on the terrible triad
- Reflects Pugh standard protocol — restore all four components to permit motion at 7-10 days
- Evidence level
- Level IV evidence base
- Position on the terrible triad
- Systematic component-by-component repair; reconstruct radial head if stable fixation achievable, otherwise replace
- Evidence level
- Level III-V
Registry and meta-analytic evidence
No national joint registry tracks terrible-triad outcomes specifically (registries capture arthroplasty episodes, not this trauma pattern), so the best pooled evidence is from systematic reviews. According to PubMed, Kyriacou et al. (DOI) found no functional difference between radial head replacement and reconstruction (MEPS 88.6 vs 88.5) but a 65% overall complication rate and ~18% reoperation rate, while Chen et al. (DOI) favoured replacement for comminuted heads.
Genuine practice variation
- Surgical approach — a meta-analysis (Meena et al., DOI) found a combined lateral-plus-anteromedial approach gave more elbow and forearm motion than a lateral-only approach, at the cost of longer operating time; lateral-only remains common where the coronoid is small and accessible through the radial head defect.
- Radial head: fix vs replace — higher-resource centres replace comminuted heads readily; in limited-resource settings reconstruction or, rarely, staged management predominates.
- Hinged external fixation — availability varies; where unavailable, surgeons rely on meticulous ligament/bone repair and protected bracing.
Be prepared to describe the systematic surgical approach to terrible triad. Know the coronoid fixation thresholds, radial head decision-making, and that LCL repair is mandatory. Understand the concept of elbow instability as a pattern requiring treatment of all components.
MCQ Practice Points
Q: What are the three osseous components of the terrible triad of the elbow? A: (1) Posterior elbow dislocation, (2) radial head fracture, (3) coronoid fracture. Note: the LCL rupture is the fourth component (soft tissue) that is always present.
Q: What is the function of the coronoid process in elbow stability? A: The coronoid is the anterior buttress that resists posterior subluxation of the ulna. It is also the insertion point for the anterior bundle of the MCL (sublime tubercle).
Q: What is the recommended surgical sequence for terrible triad repair? A: (1) Address coronoid first (fix if more than 50% or unstable), (2) radial head (ORIF or replace), (3) LCL repair (essential), (4) assess stability, (5) MCL repair if still unstable.
Q: Why must the LCL be repaired in terrible triad even if the coronoid is just a tip fracture? A: The LCL is always torn in posterior elbow dislocations. The LUCL is the primary restraint to posterolateral rotatory instability. Without repair, even small coronoid fractures can result in recurrent instability.
Q: In terrible triad, when should the radial head be replaced rather than fixed? A: When there are more than 3 fragments (unreconstructable). The radial head should never be excised without replacement as it is a critical secondary stabilizer in the MCL-deficient elbow.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old man presents after falling off a ladder. X-rays show a posterior elbow dislocation that has been reduced. Post-reduction X-rays show a radial head fracture and coronoid tip fracture. The elbow feels unstable to the ED doctor. What is your assessment and management?”
“You have performed ORIF of the coronoid (suture lasso), radial head arthroplasty, and LCL repair for a terrible triad. On testing, the elbow still redislocates at 40 degrees of extension. What do you do next?”
“A patient presents 3 weeks after a terrible triad injury that was initially splinted and sent home with plan for delayed surgery. The elbow is now stiff, with only 30-80 degrees motion, and X-ray shows early heterotopic ossification. How do you manage this?”
THE FOUR COMPONENTS
- 1. Posterior elbow dislocation
- 2. Radial head fracture (Mason IV by definition)
- 3. Coronoid fracture
- 4. LCL rupture (always present, often forgotten)
SURGICAL SEQUENCE
- 1. Coronoid: fix if more than 50% (suture, screw, or plate)
- 2. Radial head: ORIF (3 or fewer fragments) or replace (more than 3)
- 3. LCL: ALWAYS repair (suture anchors to isometric point)
- 4. Stability check: if unstable, consider MCL or hinged ex-fix
CORONOID DECISION
- Tip (less than 10%): LCL repair may be sufficient
- Less than 50% (Regan-Morrey II): consider fixation
- More than 50% (Regan-Morrey III): fixation required
- Access through radial head defect if present
RADIAL HEAD DECISION
- 3 or fewer fragments: ORIF (headless screws, safe zone)
- More than 3 fragments: arthroplasty
- NEVER excise without replacement
- Secondary stabilizer - critical in MCL-deficient elbow
LCL REPAIR
- ALWAYS required - non-negotiable
- LUCL is key component
- Repair to isometric point (center of lateral epicondyle)
- Suture anchors or bone tunnels with non-absorbable suture
TRAPS AND PEARLS
- Don't treat as simple radial head fracture
- Don't forget LCL repair
- CT is mandatory before surgery
- Early motion essential but balance with stability
- HO prophylaxis (indomethacin) recommended
Evidence Base
- 36 consecutive elbows managed with a standard protocol: radial head fixation or replacement, coronoid fixation where possible, lateral ligament and capsular repair, with selective MCL repair and hinged external fixation.
- At mean 34 months, flexion-extension arc averaged 112 degrees and forearm rotation 136 degrees. Mean Mayo Elbow Performance Score 88, with 28 of 36 good or excellent.
- Concentric stability restored in 34 of 36 elbows; 8 patients required reoperation (synostosis, recurrent instability, hardware removal/release, infection).
- Three-type classification: I (tip avulsion), II (50% or less of process), III (more than 50%). Satisfactory results in 92%, 73% and 20% of types I, II and III respectively.
- Concurrent dislocation or associated fracture rose with severity (14%, 56% and 80% for types I-III), and residual stiffness was most frequent with type III.
- Classifies coronoid fractures by anatomy: tip, anteromedial facet, and base/body. Anteromedial facet fractures are varus posteromedial rotatory fracture-subluxations and behave very differently from the terrible triad.
- Injury pattern predicts associated injuries, instability direction, surgical approach and treatment — emphasising pattern recognition over size alone.
- 9 studies, 210 patients (98 replacements, 112 reconstructions). No significant difference in mean MEPS (88.6 replacement vs 88.5 reconstruction) or range of motion.
- Reoperation rates were high in both groups (18.4% replacement, 17.9% reconstruction); overall complication rate across the cohort was 65%.
- 4 studies, 115 patients (51 repair, 64 replacement), mostly Mason II-III heads. Replacement was associated with better DASH and MEPS scores and better flexion, extension and pronation.
- Fewer post-surgical complications were reported in the replacement group than the repair group in this analysis.