Toddler's Fracture | Cozen's Phenomenon | Tibial Spine
KEY INJURY PATTERNS
Critical Must-Knows
- Toddler's fracture: spiral tibia in 9 months to 3 years, limping child, X-ray often normal initially
- Cozen's phenomenon: progressive valgus after proximal tibial metaphyseal fracture, self-corrects
- Tibial spine fracture = pediatric ACL injury - treat based on displacement
- Floating knee in children: ipsilateral femur and tibia fractures - high energy
- Intact fibula may cause valgus deformity in tibial shaft fractures
Clinical Pearls
- "Negative X-ray does not rule out toddler's fracture - treat clinically if suspected
- "Cozen's valgus peaks at 12-18 months then spontaneously corrects - observe
- "Tibial spine Type III = surgical (ORIF or arthroscopic reduction)
- "Age over 10 years: consider flexible IM nails for tibial shaft fractures
Critical Exam Concepts
Toddler's Fracture
Non-displaced spiral tibia in walking child 9 months to 3 years. X-ray often negative initially. Clinical diagnosis - limp, refuse to bear weight. Cast 3-4 weeks even if X-ray negative.
Cozen's Phenomenon
Progressive valgus after healed proximal tibial metaphyseal fracture. Develops 6-12 months post-injury, peaks at 18 months. Self-corrects by skeletal maturity. DO NOT overcorrect initially.
Tibial Spine Fractures
Pediatric ACL equivalent. Meyers-McKeever classification. Type I/II = non-operative (extension cast). Type III/IV = surgical reduction and fixation.
Floating Knee
Ipsilateral femur and tibia fractures = high energy. Screen for other injuries. May need surgical stabilization of both levels. Higher complication rate.
Quick Decision Guide by Fracture Type
| Fracture | Age | Key Feature | Treatment |
|---|---|---|---|
| Toddler's fracture | 9 months - 3 years | Spiral tibia, often occult | Cast 3-4 weeks |
| Proximal metaphyseal | 3-10 years | Risk of Cozen's valgus | Cast, observe for valgus |
| Tibial spine | 8-14 years | ACL equivalent | Type III = surgical |
| Shaft fracture | All ages | High remodeling | Cast or flexible nails |
| Floating knee | Any age | High energy | Surgical stabilization |
SPIRALToddler's Fracture Features
| S | Spiral fracture pattern Classic oblique/spiral non-displaced |
| P | Pain with weight bearing Refuses to walk, limps |
| I | Imaging often negative X-ray may be normal initially |
| R | Rotational mechanism Twisting injury from fall |
| A | Age 9 months to 3 years Typically walking age |
| L | Low energy injury Minor fall, no significant trauma |
| S | Spiral fracture pattern Classic oblique/spiral non-displaced | I | Imaging often negative X-ray may be normal initially | A | Age 9 months to 3 years Typically walking age |
| P | Pain with weight bearing Refuses to walk, limps | R | Rotational mechanism Twisting injury from fall | L | Low energy injury Minor fall, no significant trauma |
Hook:SPIRAL describes both the fracture pattern and key features!
VALCozen's Phenomenon
| V | Valgus deformity develops Progressive valgus 6-18 months post-injury |
| A | After proximal tibial metaphyseal fracture Classic location |
| L | Leaves spontaneously Self-corrects by skeletal maturity |
| V | Valgus deformity develops Progressive valgus 6-18 months post-injury |
| A | After proximal tibial metaphyseal fracture Classic location |
| L | Leaves spontaneously Self-corrects by skeletal maturity |
Hook:VAL-gus develops then VAL-ishes (vanishes)!
1234Meyers-McKeever Tibial Spine
| 1 | Type I - Minimally displaced Non-operative, extension cast |
| 2 | Type II - Anterior hinge Usually non-operative, may need reduction |
| 3 | Type III - Completely displaced Surgical fixation required |
| 4 | Type IV - Comminuted Surgical fixation required |
| 1 | Type I - Minimally displaced Non-operative, extension cast | 3 | Type III - Completely displaced Surgical fixation required |
| 2 | Type II - Anterior hinge Usually non-operative, may need reduction | 4 | Type IV - Comminuted Surgical fixation required |
Hook:Type 3+ = Surgery (the 3 looks like a backwards S for Surgical)
Overview and Epidemiology
Age Distribution
Different tibial fracture patterns occur at different ages. Toddler's fracture (9 months to 3 years), proximal metaphyseal Cozen's type (3-10 years), tibial spine (8-14 years), shaft fractures (all ages).
Epidemiology
- Second most common pediatric long bone fracture
- 15% of all pediatric fractures
- Peak incidence: toddlers and adolescents
- Boys more than girls (2:1)
- Left and right equal
Mechanisms
- Toddler's: low energy twist/fall
- Proximal metaphyseal: direct impact
- Tibial spine: hyperextension (bicycle)
- Shaft: direct blow or torsion
- Floating knee: high energy (MVA)
Anatomy and Biomechanics
Pediatric Tibial Anatomy
The proximal tibial physis grows faster than the distal (57% vs 43% of tibial growth). Injuries to the proximal physis have greater potential for growth disturbance.
Tibial Growth Plate Anatomy
Proximal tibial physis: Contributes 57% of tibial length. Located 1-2 cm distal to joint line. Protected by tibial tubercle apophysis.
Distal tibial physis: Contributes 43% of tibial length. Asymmetric closure (central, then medial, then lateral).
Tibial tubercle apophysis: Secondary ossification center. Vulnerable during adolescence (Osgood-Schlatter).
Classification Systems
Toddler's Fracture (CAST)
Childhood Accidental Spiral Tibial fracture
Characteristics: Age 9 months to 3 years (walking age). Non-displaced spiral or oblique fracture. Distal tibial shaft most common. Often not visible on initial X-ray. Low energy mechanism (twist, fall).
Clinical Assessment
Toddler's Fracture
- Refuses to bear weight
- Limping or not walking
- Point tenderness over tibia
- Often no swelling initially
- May have normal X-rays
- History of minor fall/twist
Tibial Spine
- Acute knee pain after hyperextension
- Knee effusion (hemarthrosis)
- Unable to extend knee fully
- Positive Lachman (if tested)
- Often bicycle handlebar injury
Floating Knee Assessment
High energy injury. Assess for associated injuries: ipsilateral hip, knee, ankle. Neurovascular exam essential. Screen for head, chest, abdominal trauma. Higher risk of compartment syndrome.
Compartment Syndrome Risk
Be vigilant for compartment syndrome especially in floating knee, both bone fractures, and high energy mechanisms. Pain out of proportion, pain with passive stretch, tense compartments.
Investigations
X-ray Protocol
Views: AP and lateral tibia/fibula. Include knee and ankle joints.
Toddler's fracture: May be negative initially. Look for subtle periosteal reaction at 10-14 days. Bone scan or MRI if clinical suspicion high.
Tibial spine: AP and lateral knee. CT if surgical planning needed.
Management
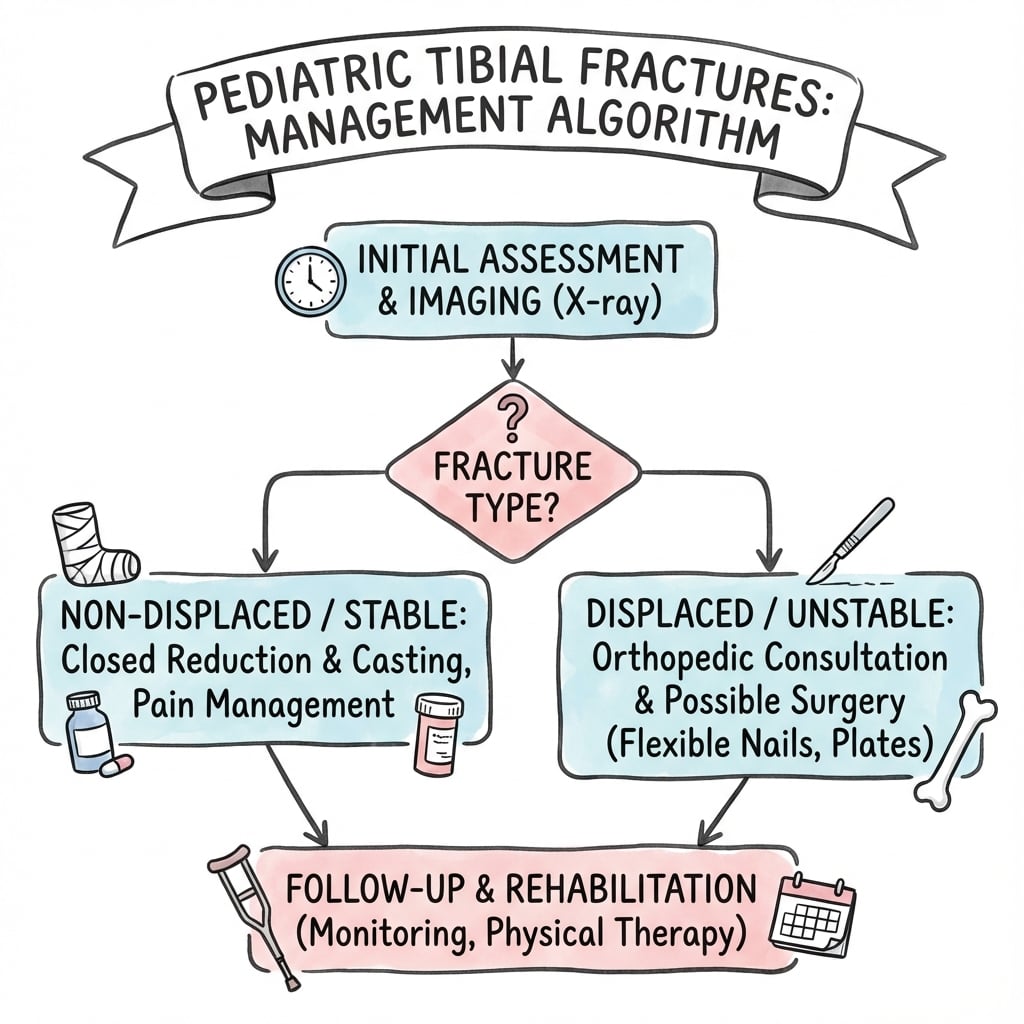
Age-Based Treatment Principles
Under 6 years: Cast treatment for most fractures. High remodeling potential. 6-10 years: Cast for stable, operative for unstable or acceptable alignment not achieved. Over 10 years: Consider flexible IM nails for shaft fractures. Lower remodeling potential.
Toddler's Fracture Management
Treatment: Long leg cast or walking boot for 3-4 weeks.
Key points:
- Treat clinically even if X-ray negative
- No reduction needed (non-displaced)
- Rapid healing in this age group
- Follow-up X-ray at 2 weeks shows callus
Prognosis: Excellent. Heals rapidly with no long-term sequelae.
Acceptable Deformity in Pediatric Tibia
Angulation: Up to 10 degrees in sagittal plane, 5 degrees in coronal plane. Shortening: Up to 1-1.5 cm (will remodel with growth). Rotation: Minimal accepted (does not remodel). Younger children tolerate more deformity due to greater remodeling potential.
Surgical Technique Considerations
Flexible IM Nailing (TENS/ESIN)
Indications: Age over 6-10 years, unstable shaft fractures, polytrauma.
Entry points: Medial and lateral distal metaphysis (avoid physis).
Nail size: 40% of medullary canal at isthmus.
Key points: Pre-contour nails for apex anterior angulation. Avoid proximal entry (tibial tubercle physis damage).
Complications
Complications by Fracture Type
| Complication | Fracture Type | Management |
|---|---|---|
| Cozen's valgus | Proximal metaphyseal | Observe - self-corrects by maturity |
| Malunion | Shaft fractures | Remodeling or corrective osteotomy if needed |
| ACL laxity | Tibial spine | Proper reduction and fixation, ACL rehab |
| Compartment syndrome | Floating knee, high energy | Urgent fasciotomy |
| Growth arrest | Physeal injuries | Bar resection or corrective procedures |
| Nonunion | Rare in children | Operative intervention if occurs |
Cozen's Phenomenon
Progressive valgus deformity after proximal tibial metaphyseal fracture. Mechanism unclear (asymmetric growth stimulation, tethering by fibula). Develops 6-18 months post-fracture. Spontaneous correction expected by skeletal maturity. Osteotomy rarely indicated before maturity.
Postoperative Care
Post-Treatment Protocol
Cast immobilization. Non-weight bearing. Monitor for compartment syndrome in high-energy injuries.
X-ray at 2-3 weeks to confirm alignment. Toddler's fracture usually healed. Weight bearing as tolerated in cast.
Remove cast when clinically and radiographically healed. Begin weight bearing. Tibial spine: begin ROM.
Follow proximal metaphyseal fractures for Cozen's valgus. Document and reassure. Tibial spine: assess for ACL laxity.
Outcomes and Prognosis
Prognosis by Fracture Type
Toddler's fracture: Excellent prognosis. Complete healing in 3-4 weeks. No long-term sequelae.
Proximal metaphyseal: Good prognosis despite Cozen's phenomenon. Most remodel by skeletal maturity.
Tibial spine: Good outcomes with proper treatment. Residual ACL laxity possible but usually not symptomatic.
Shaft fractures: Excellent prognosis. High union rates. Good remodeling potential in younger children.
Special Considerations
Floating Knee (Pediatric)
Definition: Ipsilateral femur and tibia fractures.
Mechanism: High energy trauma (MVA, fall from height).
Associated injuries: Knee ligament injuries (40-80%), vascular injuries, other trauma.
Management: Usually requires surgical stabilization of both levels. Femur typically flexible nails. Tibia cast or nails depending on pattern.
Complications: Highest risk of compartment syndrome. LLD possible.
Differential Diagnosis
The limping or non-weight-bearing child
A toddler refusing to weight-bear with a normal radiograph has a broad differential. The job is to separate a benign occult fracture from infection, malignancy and non-accidental injury before reassuring the family.
Differentiating Pediatric Tibial Fracture Patterns and Mimics
| Condition | Typical age | Key discriminator | Pitfall to avoid |
|---|---|---|---|
| Toddler's fracture | 9 months - 3 years | Point tibial tenderness, low-energy twist, periosteal reaction at 10-14 days | Calling it 'normal' on day 1 film |
| Osteomyelitis / septic arthritis | Any | Fever, raised CRP/ESR, warmth, refusal to move joint | Casting an infected limb |
| Non-accidental injury | Pre-ambulatory or inconsistent history | Mechanism-injury mismatch, other injuries on survey | Failing to safeguard a young child |
| Transient synovitis | 3-8 years | Hip-referred pain, recent viral illness, settles quickly | Missing a tibial source of pain |
| Bone tumour / cyst (pathological) | Any | Pain before injury, lytic lesion, trivial trauma | Treating fracture without imaging the lesion |
| Cozen's valgus vs true malunion | 3-10 years | Cozen's appears 8-19 months after a healed metaphyseal fracture | Blaming initial treatment for late valgus |
Controversies and Areas of Uncertainty
Cozen's: predict or just watch?
Age, sex and initial angulation do not reliably predict who develops late valgus, and the deformity usually self-corrects. Routine prophylactic intervention is not justified; the debate is how long to observe before offering guided growth.
Tibial spine: suture vs screw vs anchor
Comparative data favour suture-based fixation for function and lower implant-removal rates, but no high-quality randomised trial defines the optimal construct. Open versus arthroscopic reduction also remains debated.
Operative threshold in adolescents
The angulation/shortening a growing tibia will remodel is age-dependent and imprecise. Heavier, older adolescents behave more like adults, narrowing the case for purely closed treatment.
Imaging the occult toddler's fracture
MRI, bone scan and ultrasound can confirm occult fractures, but most authorities treat clinically without advanced imaging. The controversy is cost and radiation versus diagnostic certainty.
Evidence Base and Key Studies
How to read these cards
Each card below is anchored to a verified PubMed record (PMID and DOI shown). Use the level of evidence and sample size to judge how heavily to lean on a given statement in a viva.
Cozen's Phenomenon: Natural History and Resolution
- Retrospective series of 33 children (6 months to 14 years), mean follow-up 8.8 years
- 15 of 33 developed late valgus between 8 and 19 months (mean onset 12.5 months)
- 24 of 33 developed tibial elongation; neither finding correlated with age at injury
- Maximum valgus subsequently corrected to near the initial post-treatment angle by final follow-up
Guided Growth for Persistent Cozen's Deformity
- Largest reported series (19 patients, 24 Cozen's phenomena) treated with medial proximal tibial guided growth
- Corrective osteotomy abandoned because of frequent recurrent valgus
- Mechanical axis and medial proximal tibial angle corrected in all but one patient
- Five recurrences after implant removal; managed by repeat or retained metaphyseal screw
Tibial Eminence Fractures: Surgical Outcomes Systematic Review
- Systematic review of 12 studies of operatively treated Meyers-McKeever type II-IV fractures
- Open reduction showed higher Tegner/Lysholm scores and less arthrofibrosis than arthroscopic fixation
- Arthroscopic suture fixation outperformed arthroscopic screw fixation on functional scores
- Screw fixation carried the highest rate of implant removal
Arthroscopic Fixation Techniques for Pediatric Tibial Eminence Fractures
- Narrative review confirming arthroscopic reduction as the contemporary standard for surgical TEFs
- Anchor, suture and screw constructs gave broadly comparable clinical and radiographic results
- Suture/anchor techniques minimise physeal damage and are favoured in skeletally immature knees
- Higher-quality comparative studies are still needed to define the optimal construct
Titanium Elastic Nails for Pediatric Tibial Shaft Fractures
- 19 consecutive children (mean age 12.2 years) with unstable tibial shaft fractures treated with TENs
- All united at a mean of 11 weeks; final mean angulation 2 degrees sagittal, 3 degrees coronal
- No leg-length discrepancy or physeal arrest; entry-site irritation in 26 percent
- 12 excellent, 6 satisfactory and 1 poor result by Flynn criteria
Adolescent Tibial Shaft Fractures: Treatment Outcomes and Risk Factors
- 52 patients aged 10-18 years treated by ESIN, interlocking nail, plate, external fixator or cast
- No significant difference in union rate between fixation methods
- Open fractures had longer time to union and a 5.5-fold higher complication risk
- Heavier body weight correlated with lower radiographic union scores at 12 weeks
Occult Toddler's-Type Tibial Fractures
- Described subtle, easily missed occult tibial fractures in infants and young children
- Radiographic findings parallel the classic spiral toddler's fracture of Dunbar
- Knowledge of mechanism plus focused exam allows confident diagnosis
- Reinforces that initial radiographs are frequently unremarkable
Foundational Classification & Description (Historical)
- Meyers-McKeever (1959/1970) defined the tibial spine fracture classification still used today
- Cozen (1953) first described post-traumatic proximal tibial valgus
- Dunbar et al. (1964) coined the 'toddler's fracture' as a childhood accidental spiral tibial fracture
- These remain the eponymous source descriptions for the entities on this page
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Limping Toddler
"A 2-year-old child is brought to ED by his mother. He has been refusing to bear weight on his left leg since yesterday after a fall from a low chair. On examination, there is no obvious swelling but tenderness over the distal tibia. X-rays appear normal. How would you manage this?"
Scenario 2: Proximal Tibial Fracture with Progressive Valgus
"You are seeing an 8-year-old boy in clinic 12 months after he sustained a proximal tibial metaphyseal fracture that was treated in a cast. The fracture has healed but the parents are worried because his leg has become progressively bowed outwards. Examination confirms a 12 degree valgus deformity. How would you manage this?"
Scenario 3: Tibial Spine Fracture
"A 12-year-old girl fell off her bicycle and presents with a swollen, painful right knee. She cannot fully extend her knee. X-ray shows a tibial spine fracture that appears displaced by about 8mm with complete loss of contact. How would you manage this?"
Scenario 4: Floating Knee with Rising Pain
"A 10-year-old is brought in after being struck by a car. He has ipsilateral closed femoral shaft and tibial shaft fractures. Six hours after admission the nursing staff report escalating pain and increasing analgesia requirement despite the leg being splinted. How do you proceed?"
MCQ Practice Points
Toddler's Fracture Question
Q: A 2-year-old refuses to walk after a fall. X-ray is normal. What is the management? A: Treat as toddler's fracture with cast 3-4 weeks. Clinical diagnosis is sufficient. X-ray may be negative initially.
Cozen's Phenomenon Question
Q: What is the management of progressive valgus 12 months after proximal tibial metaphyseal fracture? A: Observation and reassurance. Cozen's phenomenon self-corrects by skeletal maturity. Do not operate early.
Tibial Spine Classification Question
Q: Which Meyers-McKeever type requires surgical treatment? A: Type III and IV. Type I and II are typically non-operative. Type III is completely displaced and requires fixation.
Floating Knee Question
Q: What is the main complication risk in floating knee injury? A: Compartment syndrome. Floating knee is high energy with highest compartment syndrome risk. Also screen for other injuries.
Acceptable Deformity Question
Q: How much angulation is acceptable in pediatric tibial shaft fractures? A: 10 degrees sagittal, 5 degrees coronal. Younger children tolerate more. Rotation does not remodel.
Intact Fibula Question
Q: What is the risk of tibial shaft fracture with intact fibula? A: Valgus deformity. Intact fibula acts as tether, preventing shortening but may cause progressive valgus.
Guidelines, Registries & Global Practice
Global Epidemiology
- Tibia/fibula fractures are among the commonest paediatric long-bone injuries worldwide
- Bimodal pattern: toddlers (low-energy twisting) and adolescents (sport, road traffic)
- Male predominance roughly 2:1 across most published cohorts
- Mechanism shifts by setting: trampolines, scooters and cycling in high-income regions; falls and road traffic dominate elsewhere
Universal Principles
- Age-based remodelling logic is shared across all major training systems (FRCS, FRACS, EBOT, ABOS, DNB/MS)
- Toddler's fracture is a clinical diagnosis treated on suspicion regardless of resources
- Displaced tibial spine and floating-knee injuries are operative everywhere when expertise allows
- Non-accidental injury must be considered in any young, pre-ambulatory child with a tibial fracture
Side-by-Side Society / System Emphasis
| Body / System | Toddler's & shaft | Tibial spine | NAI screening |
|---|---|---|---|
| AAOS / POSNA (US) | Cast for low-energy; flexible nails for unstable adolescents | Arthroscopic suture fixation favoured for displaced | Skeletal survey under 2 years per AAP |
| BOA / BOAST (UK) | Closed treatment first; ESIN for length-unstable | Refer to paediatric ortho/sports knee service | Follow BOAST safeguarding standard |
| AO Foundation | ESIN entry distal to tubercle apophysis | ORIF/ARIF avoiding physis | Document mechanism vs injury concordance |
| EFORT / European consensus | Stable angulation thresholds by age | Suture over screw to avoid removal | National safeguarding pathways |
Registry & Evidence Notes
- No dedicated paediatric tibial-fracture implant registry exists; evidence is cohort/series level
- Trauma registries (e.g. national paediatric trauma networks) inform floating-knee and polytrauma outcomes
- Flynn criteria remain the common outcome language for flexible-nail series
High- vs Limited-Resource Practice
- High-resource: routine arthroscopy, intra-operative imaging, MRI for occult injury, guided-growth implants
- Limited-resource: closed reduction and casting prioritised; open reduction when arthroscopy unavailable
- Telemedicine and serial radiographs substitute for advanced imaging where access is constrained
- Outcomes for closed-treatable patterns remain excellent regardless of setting
PEDIATRIC TIBIAL FRACTURES
Clinical summary
Toddler's Fracture
- •Age 9 months to 3 years
- •Spiral tibia, often occult on X-ray
- •Clinical diagnosis - treat if suspected
- •Cast 3-4 weeks, excellent prognosis
Cozen's Phenomenon
- •Progressive valgus after proximal tibial metaphyseal fracture
- •Develops 6-18 months post-injury
- •Self-corrects by skeletal maturity
- •DO NOT operate early
Tibial Spine
- •Pediatric ACL equivalent
- •Meyers-McKeever I-IV
- •Type I-II: non-operative (cast)
- •Type III-IV: surgical fixation
Floating Knee
- •Ipsilateral femur and tibia fractures
- •High energy - look for other injuries
- •Highest compartment syndrome risk
- •Usually requires surgical stabilization
Acceptable Deformity
- •10 degrees sagittal plane
- •5 degrees coronal plane
- •1-1.5 cm shortening
- •Rotation: minimal (doesn't remodel)