Schatzker Classification | Three-Column Concept | Staged Surgery
SCHATZKER
Critical Must-Knows
- CT is ESSENTIAL for surgical planning - reveals posterior column and true depression
- Wrinkle sign indicates safe soft tissue for ORIF (no wrinkles = no surgery)
- Three-column concept: Lateral, Medial, Posterior - each needs specific approach
- Bicondylar patterns (V-VI) require staged approach and dual plating
- Single lateral plate fails in bicondylar fractures - this is a common exam trap
Clinical Pearls
- "Hoffa fragment = posterior column involvement requiring specific approach
- "Medial plateau fracture = high-energy until proven otherwise
- "Moore classification for fracture-dislocation patterns
- "Rasmussen radiological criteria for articular reduction assessment
Clinical Imaging
Imaging Gallery




Critical Tibial Plateau Exam Points
Soft Tissue First
Wrinkle test mandatory before ORIF. No wrinkles = spanning ex-fix. High-energy (V-VI) = staged approach.[5] Compartment syndrome in 10-15%.
Three-Column Concept
CT-based surgical planning. Lateral column = anterolateral approach. Medial = anteromedial/posteromedial. Posterior = separate posterior approach.
Articular Reduction
Under 2mm step-off goal. Reduce depression through cortical window. Raft screws support subchondral bone. Bone graft prevents subsidence.
Classification = Treatment
Schatzker I-III = lateral plating. IV = medial plate essential. V-VI = dual plates staged. Single lateral plate in bicondylar = FAILURE.
Quick Decision Guide
| Patient | Fracture Pattern | Treatment | Key Pearl |
|---|---|---|---|
| Young, good soft tissue | Schatzker I (lateral split) | Percutaneous lag screws | Simple pattern = simple fix |
| Elderly, osteoporotic | Schatzker II (split-depression) | ORIF with elevation + bone graft | Support the subchondral bone |
| Any age, pure depression | Schatzker III | Arthroscopic-assisted vs open | Elevate via cortical window |
| High-energy mechanism | Schatzker IV (medial) | Medial buttress plate required | High-energy = ligament injury |
| Polytrauma, tense swelling | Schatzker V-VI | STAGE: Ex-fix → wait → dual ORIF | Wrinkle sign before definitive |
SPlIT-D-PURESchatzker Classification
| S | Split (Type I) Pure lateral split - low energy |
| D | Depression + Split (Type II) Most common type |
| P | Pure depression (Type III) Depression without split |
| M | Medial (Type IV) High-energy, varus mechanism |
| B | Bicondylar (Type V) Both condyles, intact metaphysis |
| D | Dissociation (Type VI) Metaphyseal-diaphyseal separation |
| S | Split (Type I) Pure lateral split - low energy | P | Pure depression (Type III) Depression without split | B | Bicondylar (Type V) Both condyles, intact metaphysis |
| D | Depression + Split (Type II) Most common type | M | Medial (Type IV) High-energy, varus mechanism | D | Dissociation (Type VI) Metaphyseal-diaphyseal separation |
Hook:Split patterns (I-III) are LOW energy, Medial + Bicondylar + Dissociation (IV-VI) are HIGH energy!
WRINKLESoft Tissue Management
| W | Wait 7-14 days minimum for high-energy |
| R | Reduce swelling first Elevation, ice, splint |
| I | Ice and elevation Above heart level |
| N | No surgery on tense skin Wrinkle test mandatory |
| K | Keep spanning ex-fix Bridge until soft tissue ready |
| L | Look for blisters Clear = epidermis only, blood = full thickness |
| E | Elevate limb above heart Continuous until wrinkle positive |
| W | Wait 7-14 days minimum for high-energy | N | No surgery on tense skin Wrinkle test mandatory | E | Elevate limb above heart Continuous until wrinkle positive |
| R | Reduce swelling first Elevation, ice, splint | K | Keep spanning ex-fix Bridge until soft tissue ready | ||
| I | Ice and elevation Above heart level | L | Look for blisters Clear = epidermis only, blood = full thickness |
Hook:WRINKLE test = No wrinkles on skin, no surgery on fracture!
LMPThree-Column Surgical Planning
| L | Lateral column Anterolateral approach, lateral plate |
| M | Medial column Anteromedial or posteromedial approach |
| P | Posterior column Posteromedial +/- posterolateral approach |
| L | Lateral column Anterolateral approach, lateral plate |
| M | Medial column Anteromedial or posteromedial approach |
| P | Posterior column Posteromedial +/- posterolateral approach |
Hook:Lateral-Medial-Posterior = Every column needs its own approach and plate!
Overview and Epidemiology
Why This Topic is High-Yield
Tibial plateau fractures test your understanding of articular fracture principles, soft tissue management, and staged surgery. Examiners focus on classification, when NOT to operate, approach selection, and complication avoidance.
Demographics
- Bimodal distribution: Young (high-energy) + Elderly (low-energy)
- Lateral plateau more common (55-70%)
- Male predominance in young, female in elderly
- Sports injuries, MVA, falls from height
Clinical Impact
- Weight-bearing articular surface injury
- Long-term OA risk (10-30%)[8,9]
- Associated soft tissue injuries common
- Significant rehabilitation required
- Work and function implications
Anatomy and Biomechanics
Critical Anatomy - Posterior Vessels
The popliteal artery lies directly posterior to the tibia, separated by only the popliteus muscle. During posterior approaches, the neurovascular bundle must be carefully protected. Tethering at the soleal arch makes it vulnerable to injury with posterior displacement.
Surface Anatomy
Lateral Plateau
- Convex surface - less congruent with femoral condyle
- Higher position (3mm proximal to medial)
- More prone to depression fractures
- Lateral meniscus covers 80%
Medial Plateau
- Concave surface - greater congruency
- Larger weight-bearing surface (60%)
- Stronger subchondral bone
- Medial meniscus covers 50%
Tibial Slope: 7-10° posterior slope - must restore during fixation
Intercondylar Eminence: Central, contains ACL and PCL insertions
Classification Systems
Schatzker Classification (1979)[1]
Schatzker Classification Summary
| Type | Pattern | Mechanism | Treatment |
|---|---|---|---|
| I | Lateral split (wedge) | Low-energy valgus | Lag screws ± buttress plate |
| II | Lateral split-depression | Low-energy valgus | ORIF: elevate, graft, buttress plate |
| III | Pure lateral depression | Low-energy axial | Elevation, raft screws, graft |
| IV | Medial plateau fracture | HIGH-energy varus | Medial buttress plate essential |
| V | Bicondylar (split) | HIGH-energy axial | Dual plating, staged approach |
| VI | Metaphyseal-diaphyseal dissociation | HIGH-energy | Staged, dual/ring fixation |

Key Distinction
Type II vs Type III: Type II has a split component (cortical break), Type III is pure depression (cortex intact). This changes surgical approach - Type II can be opened like a book to access the depression.

Clinical Assessment
History
- Mechanism: Axial load + valgus/varus (bumper fracture)
- Energy level: Fall height, MVA speed
- Comorbidities: Osteoporosis, diabetes, smoking
- Anticoagulation status: Affects timing
- Functional demands: Activity level, occupation
Examination
- Look: Swelling, bruising, deformity, wounds
- Feel: Tenderness, crepitus, effusion
- Move: Limited by pain, instability
- Special: Neurovascular status MANDATORY
- Compartments: Assess all four leg compartments
Mandatory Assessment
Vascular: Palpate dorsalis pedis and posterior tibial pulses. Calculate ABI if ANY concern. Popliteal artery injury in 2-3% of tibial plateau fractures.
Neurological: Common peroneal nerve (foot drop), posterior tibial nerve (sole sensation).
Compartments: Pain with passive stretch of toes, tense compartments, pain out of proportion. Low threshold for fasciotomy.
Critical for Surgical Timing
Soft Tissue Checklist
- Open fracture? (Gustilo classification)
- Fracture blisters? (Clear vs blood-filled)
- Tension? Tenting? Impending necrosis?
- Wrinkle test: Can you see skin wrinkles over anterior tibia?
- No wrinkles = too swollen for ORIF
- Document in notes with photos
- Wrinkle positive + good skin = proceed to ORIF
- Wrinkle negative = spanning external fixator
- Wait 7-14 days for swelling to resolve
Blistering
Clear blisters = epidermis only, can operate through. Blood-filled (hemorrhagic) blisters = full-thickness injury, AVOID incisions through these areas.
Differential Diagnosis of the Acute Painful Swollen Knee After Injury
Differential Diagnosis
| Diagnosis | Discriminating Features | Key Investigation |
|---|---|---|
| Tibial plateau fracture | Bony tenderness over the plateau, valgus/varus mechanism, lipohaemarthrosis, axial-load injury | AP/lateral radiographs then CT |
| Tibial spine (eminence) avulsion | Younger patient, ACL-type mechanism, central bony fragment without articular depression | Radiograph / CT; MRI for ACL |
| Distal femur / Hoffa fracture | Tenderness localised to femoral condyle, coronal split on lateral film | CT (coronal plane fracture often missed on X-ray) |
| Knee dislocation / multiligament injury | Gross instability, dimple sign, high suspicion for vascular injury | Vascular assessment, ABI, CT angiography |
| Patellar fracture / extensor mechanism rupture | Anterior tenderness, inability to straight-leg-raise, palpable gap | Radiograph; ultrasound/MRI for tendon |
| Isolated ligament/meniscal injury (no fracture) | Effusion without bony tenderness, normal radiographs, mechanism-specific instability | MRI |
| Pseudo-fracture: bone bruise / osteochondral injury | Effusion, normal radiographs, focal subchondral signal | MRI |
Investigations
Imaging Protocol
Standard knee series: AP, lateral, oblique views
Key measurements:
- Tibial plateau angle (joint line)
- Condylar widening
- Depression depth
- Stress views if ligamentous injury suspected
Mandatory for surgical planning in ALL displaced fractures.
What CT reveals:
- True articular depression (often underestimated on X-ray)
- Posterior column involvement (missed in 30% on X-ray)
- Comminution and fragment size
- Coronal plane fracture lines
Reconstructions: Axial, coronal, sagittal, 3D
Indications:
- Suspected meniscal injury (for surgical planning)
- Ligamentous injury evaluation
- Occult fracture in non-displaced injuries
Timing: Usually done post-operatively or after swelling subsides.

CT Findings That Change Management
Posterior column involvement (seen on CT) requires ADDITIONAL posterior approach - cannot be addressed through anterolateral approach alone. This is WHY CT is mandatory!
Management Algorithm
Indications for Conservative Management
Absolute Indications
- Non-displaced or minimally displaced (under 2mm step-off)
- Stable knee on stress testing
- Low functional demand patient
- Severe medical comorbidities precluding surgery
Protocol
- Long leg cast or hinged knee brace
- Non-weight-bearing 6-8 weeks
- Progressive ROM starting week 2-4
- Serial X-rays to monitor position
- Full weight-bearing by 12 weeks
Close Monitoring Required
Weekly X-rays for first 2-3 weeks to monitor for displacement. If any secondary displacement, convert to operative management.
Surgical Technique
Pre-operative Planning
Consent Points
- Infection: 2-5% superficial, 1-2% deep
- Wound complications: 5-10% (higher in Schatzker V-VI)
- Nerve injury: Peroneal nerve at risk (1-2%)
- Stiffness: Common, may need MUA/arthrolysis
- Malunion/nonunion: 5-10%
- Post-traumatic OA: 10-30%
- Hardware removal: May be needed
Equipment Checklist
- Plates: Lateral locking plate, medial buttress plate, posterior plates
- Screws: Lag screws, raft screws, locking screws
- Graft: Bone graft substitute or autograft
- C-arm: Two image intensifiers ideal
- Reduction tools: Femoral distractor, reduction clamps, bone tamp
- Fluoro views: AP, lateral, Schatzker views
For Lateral Column
Position: Supine, bump under hip, slight knee flexion
Step-by-Step
Landmarks: Line from fibular head to Gerdy's tubercle
Curved incision parallel to lateral joint line, centered over lateral plateau
Length: 10-15cm, extensile if needed
- Incise iliotibial band in line with skin incision
- Identify and protect common peroneal nerve at fibular neck
- Retract tibiofemoral joint with Z-retractors
Nerve Protection
Common peroneal nerve wraps around fibular neck. Flex knee to relax. Never use retractors near fibular head without visualization.
- Submeniscal arthrotomy to visualize articular surface
- Elevate anterior tibialis muscle from lateral tibial surface
- Expose metaphysis for plate application
For Type II (split-depression):
- Open the split fragment like a book
- Visualize depressed articular fragments
- Use bone tamp to elevate depression
- Pack with bone graft
- Reduce split fragment over elevated joint
- Provisional K-wire fixation
- Lag screws for split component
- Raft screws (subchondral) to support elevated segment
- Apply lateral buttress/locking plate
- Final imaging in all planes
Intraoperative Troubleshooting
Common Problems and Solutions
| Problem | Cause | Solution |
|---|---|---|
| Cannot visualize articular surface | Inadequate exposure | Use femoral distractor to open joint, extend arthrotomy, consider arthroscopy |
| Depressed fragment won't elevate | Impacted into metaphysis | Use larger tamp, more force, consider wider cortical window |
| Elevated fragment subsides | No subchondral support | Add raft screws, more bone graft, check for void |
| Condylar widening persists | Inadequate reduction of split | Re-apply reduction clamp, add lag screw across condyle |
| Poor bone quality, screws toggle | Osteoporosis | Use locking screws, consider cement augmentation, longer construct |
| Posterior column unreducible | Wrong approach | Add posteromedial or posterolateral approach |
Complications
Complications by Timing and Severity
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Wound dehiscence/infection | 5-10% | Schatzker V-VI, diabetes, smoking, early surgery | Early: debridement, ABx. Late: may need flap |
| Compartment syndrome | 5-10% | High-energy, polytrauma, prolonged surgery | Four-compartment fasciotomy URGENT |
| Deep venous thrombosis | 10-20% | Immobility, no prophylaxis | Prophylaxis mandatory, anticoagulation |
| Post-traumatic OA | 10-30% | Poor reduction, cartilage damage, malalignment | Activity modification, eventual arthroplasty |
| Malunion/varus collapse | 5-10% | Poor fixation, single plate for bicondylar | High tibial osteotomy if symptomatic |
| Stiffness | 15-25% | Delayed mobilization, prolonged immobilization | Early physio, may need MUA or arthrolysis |
| Hardware prominence | 10-20% | Thin soft tissue, prominent plate | Hardware removal when healed |
Compartment Syndrome
High-energy tibial plateau fractures have 5-10% compartment syndrome risk. Monitor closely postoperatively. Pain out of proportion, pain with passive toe stretch, tense compartments = fasciotomy. Clinical diagnosis - do not wait for compartment pressure measurements if clinical suspicion.
Varus Collapse
Varus collapse occurs when medial column is not adequately supported. Single lateral plate in bicondylar fracture allows medial column to collapse. Prevention: dual plating, adequate medial buttress.
Postoperative Care and Rehabilitation
Rehabilitation Protocol
- DVT prophylaxis: Enoxaparin or TED/pneumatic boots
- Pain control: Multimodal, consider nerve block
- Wound care: Monitor for hematoma, infection
- ROM: Start passive ROM in CPM if available
- Weight-bearing: Toe-touch or non-weight-bearing
- Weight-bearing: Non-weight-bearing or touch-weight-bearing
- ROM goals: 0-90° by 6 weeks
- Exercises: Quad sets, straight leg raises, gentle ROM
- X-rays: 2 weeks, 6 weeks for union assessment
- Remove sutures: 2-3 weeks
- Weight-bearing: Progressive based on radiographic healing
- ROM goals: Full ROM by 12 weeks
- Strengthening: Progressive resistance exercises
- X-rays: 12 weeks for union confirmation
- Full weight-bearing: When radiographic union confirmed
- Return to work: Sedentary 6-8 weeks, manual labor 4-6 months
- Return to sport: 6-12 months depending on sport
- Surveillance: Annual X-rays for OA development
Weight-Bearing Protocol
- Schatzker I-III: May allow early protected WB
- Schatzker IV-VI: Strict NWB 6-8 weeks minimum
- Osteoporotic bone: Extended protected WB
- Progression based on radiographic healing
Red Flags to Watch
- Increasing pain or swelling (infection?)
- Loss of ROM (stiffness, arthrofibrosis)
- Hardware prominence (may need removal)
- Progressive deformity (loss of fixation)
Outcomes and Prognosis
Outcomes by Treatment and Pattern
| Pattern/Treatment | Good Outcomes | Key Factors |
|---|---|---|
| Schatzker I-II with ORIF | 80-90% | Anatomic reduction, stable fixation |
| Schatzker III | 75-85% | Elevation quality, graft support |
| Schatzker IV | 70-80% | Medial buttress, ligament healing |
| Schatzker V-VI staged ORIF | 60-75% | Soft tissue handling, staged approach |
| V-VI primary ORIF (poor soft tissue) | 40-60% | High complication rate |
Predictors of Poor Outcome
Poor prognostic factors:
- High-energy mechanism (Schatzker V-VI)
- Bicondylar involvement
- Greater than 10mm initial depression
- Associated ligament injury
- Post-traumatic OA precursors (cartilage damage)
- Smoking, diabetes, obesity
- Articular step-off greater than 2mm
Evidence Base
Schatzker - The Tibial Plateau Fracture: The Toronto Experience
- Original six-type classification derived from the 1968-1975 Toronto series
- Types I-III are low-energy lateral plateau injuries; Types IV-VI are higher-energy
- Medial plateau (Type IV) and bicondylar (V-VI) patterns carry the worst prognosis
- Classification stratifies fractures by mechanism, displacement and treatment
Luo - Three-Column Fixation for Complex Tibial Plateau Fractures
- Introduced the CT-based three-column (lateral, medial, posterior) concept
- Prospective cohort of 29 Schatzker V-VI three-column fractures
- Combined posterior (inverted L) and anterolateral approaches achieved satisfactory reduction in all but one case
- Posterior column involvement is poorly seen on plain films and drives approach selection
Barei - Bicondylar Fractures Treated with Dual Incisions and Medial/Lateral Plates
- 83 AO/OTA 41-C3 bicondylar fractures treated with anterolateral + posteromedial dual plating
- Satisfactory articular reduction (2mm or less) achieved in only 55% despite dual incisions
- Accurate articular reduction independently predicted better MFA functional scores (p=0.029)
- Only 2 deep infections, supporting the dual-incision strategy over a single extensile midline approach
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classification and Initial Management (~2-3 min)
"A 55-year-old woman falls off a ladder and presents with a painful swollen knee. X-rays show a lateral tibial plateau fracture with 8mm of articular depression and a split component. How would you assess and manage this patient?"
Scenario 2: Surgical Technique Deep Dive (~3-4 min)
"Walk me through your surgical technique for a Schatzker VI fracture in a 35-year-old male involved in a motorcycle accident. He is day 10 post-injury, wrinkle test is positive, and CT shows involvement of lateral, medial, and posterior columns."
Scenario 3: Complication Management (~2-3 min)
"A 45-year-old patient is day 1 post-ORIF for a Schatzker V fracture. The nurse calls because the patient has severe pain despite IV morphine, and pain with passive toe extension. How do you manage this?"
MCQ Practice Points
Classification Question
Q: A 60-year-old woman falls from standing and has lateral tibial plateau fracture with 6mm depression but no cortical split. What Schatzker type is this?
A: Schatzker Type III - pure depression without split component. Type II would have both split AND depression. This distinction is important as Type III may be treated arthroscopically.
Anatomy Question
Q: During the anterolateral approach to the tibial plateau, which structure is at greatest risk and how is it protected?
A: Common peroneal nerve at the fibular neck. Protected by flexing the knee to relax the nerve, direct visualization during dissection, and avoiding retractors at the fibular head area.
Treatment Question
Q: What is the consequence of using a single lateral plate for a Schatzker V (bicondylar) tibial plateau fracture?
A: Varus collapse of the medial column. The unsupported medial condyle collapses, leading to progressive varus malalignment. Dual plating with medial buttress is required.
Timing Question
Q: A patient with Schatzker VI fracture has tense swelling and blood-filled blisters. What is the appropriate initial management?
A: Spanning external fixator with staged delayed ORIF. Blood-filled blisters indicate full-thickness skin injury. Operating definitively risks wound dehiscence and infection. Wait 7-21 days for wrinkle test positive.
Imaging Question
Q: Why is CT scan mandatory for tibial plateau fracture surgical planning?
A: CT reveals posterior column involvement (missed in 30% on X-ray), true articular depression depth, fracture comminution, and guides approach selection. Plain X-ray underestimates depression and misses coronally-oriented fractures.
Complication Question
Q: What is the incidence of post-traumatic osteoarthritis following tibial plateau fractures, and what factors predict poor outcome?
A: 10-30% develop symptomatic OA. Predictors: articular step-off greater than 2mm, high-energy mechanism, meniscal injury, malalignment, and cartilage damage at time of injury.
Guidelines, Registries & Global Practice
Global Epidemiology
Tibial plateau fractures account for roughly 1% of all fractures and about 8% of fractures in the elderly, with a bimodal distribution: high-energy injuries (road traffic and fall-from-height) in younger men, and low-energy fragility fractures in older women. The lateral plateau is involved most often (Schatzker I-III predominate in most series), reflecting the physiological valgus axis of the knee. Incidence is rising in ageing high-income populations driven by osteoporotic and sporting injuries, while motor-vehicle trauma dominates in low- and middle-income settings.
Side-by-Side Guidance
International Guidance and Evidence
| Body / Source | Region | Key Position | Evidence Basis |
|---|---|---|---|
| AO Foundation / OTA principles | Global | Articular reduction (step 2mm or less), restore mechanical axis and slope, column-specific approaches, staged ORIF for compromised soft tissues | Expert consensus + cohort evidence |
| BOA / BOAST (Open Fractures, soft-tissue principles) | UK | Senior decision-making, ortho-plastic input for high-energy/open patterns, definitive fixation only when soft tissues allow | Guideline (consensus) |
| NICE (NG38 - complex fractures) | UK | Senior multidisciplinary planning, CT for intra-articular fractures, VTE assessment, regional major-trauma networks | Guideline (GRADE) |
| COTS randomised evidence | Canada | Ring fixation a valid lower-morbidity alternative to dual plating in bicondylar fractures | Level 1 RCT [PMID 17142411] |
| AAOS (intra-articular fracture principles, VTE) | USA | Anatomic articular restoration; individualised VTE prophylaxis after lower-limb trauma | Guideline / appropriate-use |
Registry & Practice Variation
There is no dedicated international tibial plateau fracture registry; most outcome data derive from trauma databases and population cohorts. Population-level Canadian data show a 10-year total knee arthroplasty rate of 7.3% after operative fixation, a 5.3-fold increase over matched controls (Wasserstein et al., [PMID 24430414]). Practice varies internationally: dual plating dominates in North America and Europe, whereas circular/ring fixation retains strong support where soft-tissue compromise is common or plating expertise is limited. Access also varies - high-income systems can deliver staged spanning external fixation within hours, whereas resource-limited settings may rely more heavily on definitive external fixation.
Australian Practice Points
- Surgical options: ORIF (column-specific plating) with bone graft/substitute for depression; ring fixation for poor soft tissues
- Networks: Complex V-VI patterns referred to major trauma services
- Wait times: Public lists may delay definitive surgery beyond the ideal window - staged ex-fix bridges this gap
- Registry: No specific plateau registry; AOANJRR captures any subsequent arthroplasty
ACSQHC / Safety Standards
- VTE prophylaxis: Risk-assessed for all lower-limb trauma
- Surgical safety checklist: Team briefing, time-out, sign-out
- Consent: Document shared decision-making and alternatives
- Falls prevention: Multidisciplinary pathway for elderly fragility injuries
Medicolegal Considerations
Key documentation requirements:
- Neurovascular status pre- and post-operatively
- Soft tissue assessment and rationale for timing
- CT scan findings and surgical plan based on CT
- Informed consent including alternatives
- Intraoperative imaging confirming reduction quality
Common litigation issues:
- Compartment syndrome: Missed or delayed diagnosis
- Peroneal nerve injury: Failure to document preop status
- Wound complications: Operating on compromised soft tissue
- Malunion: Inadequate reduction or single plate for bicondylar
TIBIAL PLATEAU FRACTURES
Clinical summary
Key Anatomy
- •Lateral plateau: convex, 3mm higher, depression-prone
- •Medial plateau: concave, 60% weight-bearing, stronger bone
- •Popliteal vessels: directly posterior, at risk in posterior approaches
- •Common peroneal nerve: wraps fibular neck, at risk in lateral approaches
- •Posterior tibial slope: 7-10°, must restore
Classification (Schatzker)
- •Type I: Lateral split (wedge) - low energy - screws/plate
- •Type II: Lateral split-depression - most common - ORIF + graft
- •Type III: Pure depression - elevate, graft, raft screws
- •Type IV: Medial plateau - HIGH energy - medial plate required
- •Type V: Bicondylar - staged dual plating
- •Type VI: Metaphyseal-diaphyseal dissociation - staged, dual/ring
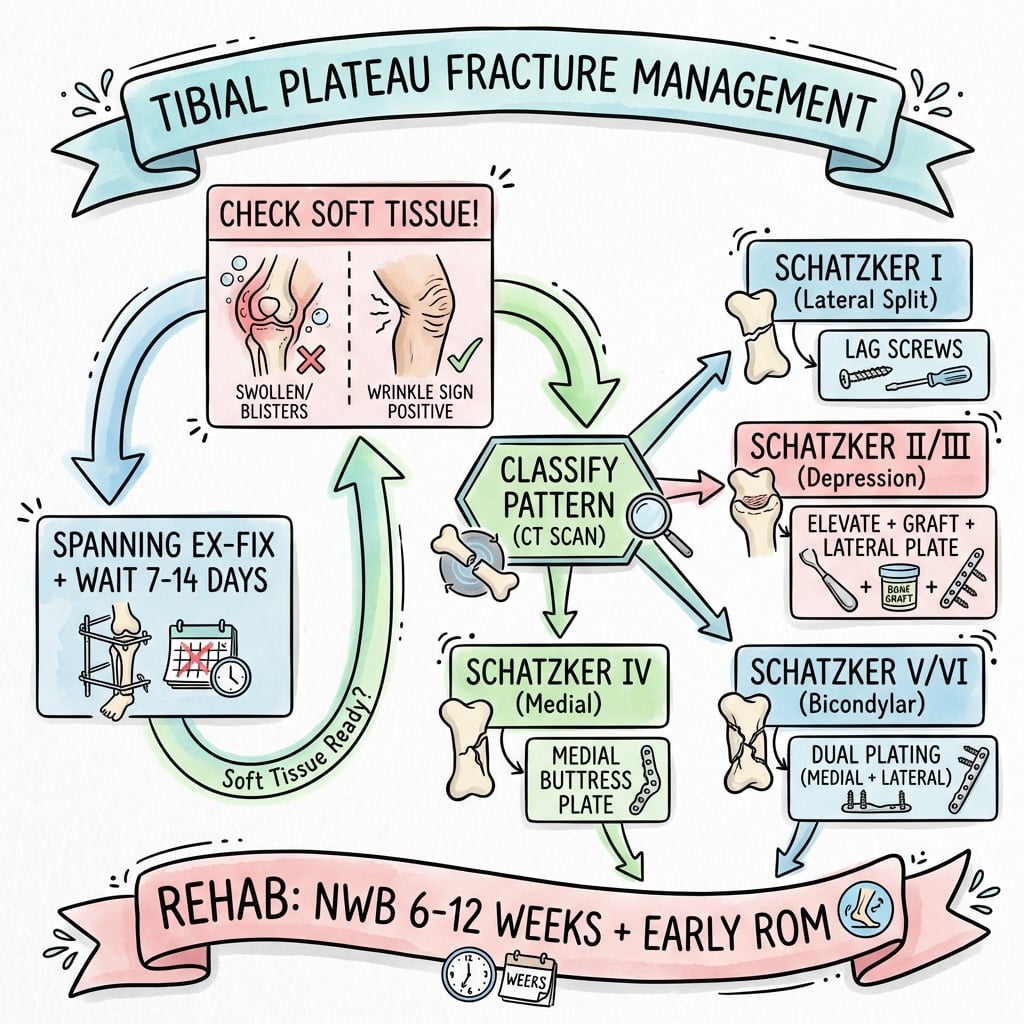
Treatment Algorithm
- •Soft tissue first: wrinkle test mandatory before ORIF
- •No wrinkles = spanning external fixator, wait 7-21 days
- •CT for ALL surgical planning (posterior column)
- •Single lateral plate for bicondylar = FAILURE
- •Articular step under 2mm, slope 7-10°, neutral alignment
Surgical Pearls
- •Three-column concept: each column needs its approach and plate
- •Anterolateral: protect peroneal nerve, flex knee
- •Posteromedial: protect popliteal vessels, flex knee
- •Submeniscal arthrotomy for articular visualization
- •Bone graft mandatory for depression patterns[6]
Complications
- •Compartment syndrome: 5-10%, pain with passive stretch
- •Wound complications: 5-10%, higher in V-VI
- •Post-traumatic OA: 10-30%[8,9]
- •Varus collapse: single plate failure in bicondylar
- •Stiffness: 15-25%, may need MUA