Anterior Cortex = HIGH RISK | Posteromedial = Low Risk | MRI Gold Standard
- Anterior cortex = HIGH RISK - tension side, poor healing, may need surgery
- Posteromedial = LOW RISK - compression side, heals well with rest
- Dreaded black line = anterior cortex stress fracture visible on XR/CT
- MRI is gold standard - shows bone marrow edema before XR changes
- Female athlete triad - amenorrhea, eating disorder, osteoporosis = risk factor
- Complete fracture risk if anterior cortex not treated appropriately
- “Anterior cortex stress fractures may require prophylactic IM nailing
- “XR may be normal for 2-6 weeks - order MRI if high clinical suspicion
- “Return to sport based on pain-free activity, not arbitrary timeframes
- “Ask about training errors - sudden increase in volume/intensity
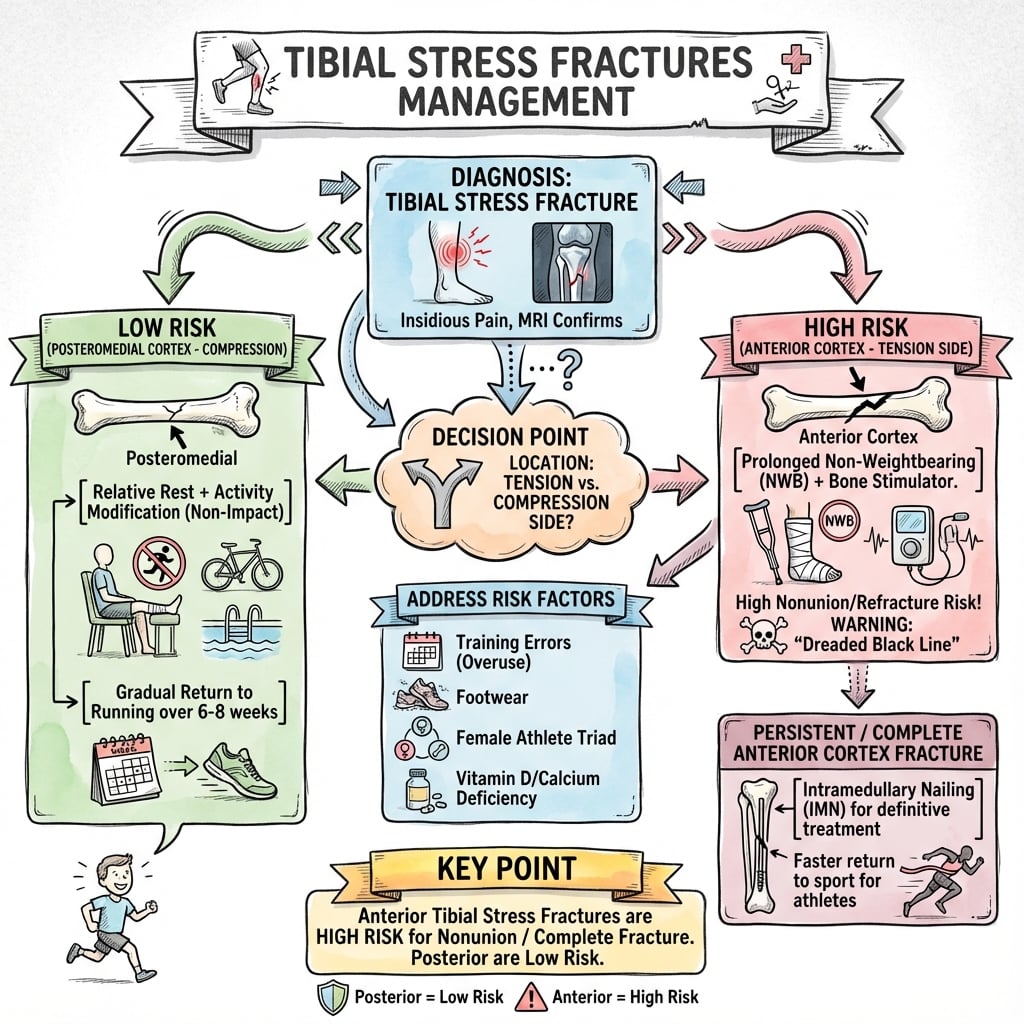
Anterior cortex stress fractures are HIGH RISK for non-union and complete fracture. They occur on the tension side with poor blood supply. The "dreaded black line" on imaging is ominous.
Posteromedial stress fractures are LOW RISK. They occur on the compression side with excellent blood supply. Most heal with 6-8 weeks of activity modification.
MRI is gold standard showing bone marrow edema 2-6 weeks before XR changes. Order MRI when clinical suspicion is high but XR is normal.
Always ask about training - sudden increases in volume, intensity, or surface changes are classic precipitants. Also screen for female athlete triad.
Overview and Epidemiology
Definition
Stress fractures are overuse injuries resulting from repetitive submaximal loading that exceeds the bone's ability to remodel and repair. The tibia is the most common site.
Epidemiology
- 50% of all stress fractures occur in the tibia
- Military recruits: 1-5% incidence during basic training
- Runners: Account for majority of tibial stress fractures
- Female athletes: 2-10x higher risk than males
- Peak age: 17-25 years (high-activity athletes/military)
Risk Factors
- Female sex
- Low BMI/eating disorders
- Menstrual irregularities (female athlete triad)
- Low bone mineral density
- Previous stress fracture
- Leg length discrepancy
- Pes planus or cavus foot
- Sudden increase in training volume/intensity
- Change in running surface
- Inadequate footwear
- Poor nutrition (calcium, vitamin D deficiency)
- High Risk (Anterior)
- Anterior cortex
- Low Risk (Posteromedial)
- Posteromedial cortex
- High Risk (Anterior)
- TENSION
- Low Risk (Posteromedial)
- COMPRESSION
- High Risk (Anterior)
- Poor
- Low Risk (Posteromedial)
- Excellent
- High Risk (Anterior)
- Non-union/complete fracture
- Low Risk (Posteromedial)
- Heals well
- High Risk (Anterior)
- Dreaded black line
- Low Risk (Posteromedial)
- Periosteal reaction
- High Risk (Anterior)
- Consider surgery
- Low Risk (Posteromedial)
- Rest and activity modification
- High Risk (Anterior)
- 3-6 months
- Low Risk (Posteromedial)
- 6-8 weeks
Anatomy and Pathophysiology
Tibial Anatomy Relevant to Stress Fractures
- Located on tension side during loading
- Tensile forces promote crack propagation
- Poor periosteal blood supply anteriorly
- Cortical bone with minimal cancellous support
- "Dreaded black line" represents true cortical fracture
- Located on compression side during loading
- Compressive forces favor healing
- Rich periosteal blood supply
- More cancellous bone support
- Typically appears as periosteal reaction
Pathophysiology of Stress Fractures
- Normal activity causes microdamage
- Osteoclasts resorb damaged bone (takes 3 weeks)
- Osteoblasts lay down new bone (takes 3 months)
- If loading exceeds repair capacity, stress fracture develops
- Grade 1: Periosteal edema only
- Grade 2: Bone marrow edema
- Grade 3: Marrow edema + cortical signal abnormality
- Grade 4: Complete fracture line (with or without displacement)
The "dreaded black line" refers to the radiographic appearance of an anterior cortex stress fracture - a horizontal radiolucent line in the anterior tibial cortex. This represents a true cortical fracture and carries high risk of non-union or complete fracture if not managed appropriately.
Classification Systems
Risk-Based Classification
The most clinically relevant classification for tibial stress fractures stratifies them by anatomical location and biomechanical risk.
- Located anteriorly in mid-diaphysis
- Experiences tensile forces during loading
- Poor periosteal blood supply
- "Dreaded black line" appearance
- High risk of non-union (30-50% with conservative treatment)
- May require surgical fixation
- Insidious onset over weeks
- Pain worse with activity, improves with rest initially
- Eventually progresses to rest pain
- Often presents late due to gradual onset
- XR shows transverse lucency in anterior cortex
- CT/MRI confirms extent of cortical involvement
- Prolonged protected weight-bearing (3-6 months) if conservative
- Frequent imaging surveillance
- Strong consideration for prophylactic IM nailing
- Elite athletes often require surgical fixation for timely return
Proper technique and attention to detail ensure optimal outcomes.
Fredericson MRI Grading (Severity)
This classification grades the severity of stress injury based on MRI findings and correlates with return-to-activity timeline.
- T1 Signal
- Normal
- T2/STIR Signal
- Periosteal edema only
- Description
- Mild stress reaction
- Return Timeline
- 2-3 weeks
- T1 Signal
- Normal
- T2/STIR Signal
- Periosteal + marrow edema
- Description
- Moderate stress reaction
- Return Timeline
- 3-6 weeks
- T1 Signal
- Low signal
- T2/STIR Signal
- Marrow + cortical signal change
- Description
- Stress fracture without line
- Return Timeline
- 12-16 weeks
- T1 Signal
- Low signal
- T2/STIR Signal
- Fracture line visible
- Description
- Stress fracture with line
- Return Timeline
- 14-16 weeks
- T1 Signal
- Low signal
- T2/STIR Signal
- Complete fracture through cortex
- Description
- Complete stress fracture
- Return Timeline
- 16+ weeks or surgery
Clinical Application:
- Grade 1-2: Stress reaction - relative rest, modify activity
- Grade 3-4: True stress fracture - complete rest from running
- Anterior cortex Grade 4 with black line - surgical consideration
- Higher grades require longer recovery before return to sport
The anterior mid-diaphyseal cortex is not the only high-risk tibial stress fracture - the medial malleolus stress fracture is a second, distal high-risk site that examiners expect you to know:
- Seen in runners and jumping athletes (basketball, dancers), it arises from repetitive talar impingement against the medial malleolus and the tensile/torsional load there.
- The characteristic pattern is a vertical fracture line propagating proximally from the junction of the tibial plafond and the medial malleolus (sometimes more oblique) - not the horizontal "black line" of the anterior shaft.
- It is high-risk for delayed/non-union and progression to a complete displaced medial malleolar fracture.
- Management: a lesion with no visible fracture line may be tried in a boot / non-weight-bearing, but a visible fracture line, displacement, or the high-demand athlete is generally treated with internal fixation (one or two partially-threaded cancellous screws across the malleolus), which gives reliable union and faster return.
So when you list high-risk tibial stress fractures, name both the anterior diaphyseal cortex and the medial malleolus.
Clinical Assessment and Diagnosis
History
- Training history - recent changes in volume, intensity, surface
- Onset - insidious, activity-related
- Location of pain - anterior vs posteromedial
- Night pain (suggests more advanced injury)
- Previous stress fractures
- Dietary history, menstrual history (female athlete triad)
- Medications (bisphosphonates can cause atypical fractures)
- Anterior tibial pain (high-risk location)
- Pain at rest or night
- History of multiple stress fractures
- Signs of eating disorder/amenorrhea
Physical Examination
- Usually normal externally
- May have subtle swelling
- Point tenderness over fracture site
- Anterior cortex: tender mid-tibial anterior border
- Posteromedial: tender along posteromedial border (distal more common)
- Hop test: Single-leg hop reproduces pain (sensitive)
- Tuning fork test: Vibration over fracture site causes pain (poor specificity)
- Fulcrum test: Bending stress reproduces pain
- MTSS
- Diffuse over 5+ cm
- Stress Fracture
- Focal point tenderness
- MTSS
- Gradual
- Stress Fracture
- Progressive worsening
- MTSS
- Early in activity, improves
- Stress Fracture
- Worsens with activity
- MTSS
- Rare
- Stress Fracture
- Common if advanced
- MTSS
- Periosteal edema, no fracture
- Stress Fracture
- Bone marrow edema, fracture line
Differential Diagnosis of Exercise-Related Leg Pain
The radiographic differential of a tibial stress lesion also includes osteoid osteoma, malignancy and chronic osteomyelitis, which can mimic a stress reaction on imaging [PMID 28343329]. The clinical differential of activity-related shin pain is summarised below.
- Key features
- Focal point tenderness, training error
- Pain pattern
- Worsens with activity, may have night pain
- Imaging / test
- MRI marrow oedema +/- fracture line
- Discriminator
- Focal lesion; positive hop test
- Key features
- Diffuse tenderness over 5cm or more
- Pain pattern
- Eases as run continues
- Imaging / test
- MRI periosteal oedema, no marrow oedema
- Discriminator
- Diffuse, no focal lesion
- Key features
- Tightness, cramping, paraesthesia
- Pain pattern
- Builds during exercise, relieved by rest
- Imaging / test
- Dynamic compartment pressure testing
- Discriminator
- Pressure rise post-exercise; neuro symptoms
- Key features
- Calf claudication in young athlete
- Pain pattern
- Exercise-induced, resolves with rest
- Imaging / test
- Ankle-brachial index, CT/MR angiography
- Discriminator
- Vascular, not bony; provocative ankle position
- Key features
- Well-localised, often nocturnal pain
- Pain pattern
- Night pain relieved by NSAIDs
- Imaging / test
- CT shows nidus with sclerosis
- Discriminator
- Classic NSAID-responsive night pain
- Key features
- Rest pain, systemic features
- Pain pattern
- Progressive, unrelated to activity
- Imaging / test
- MRI +/- biopsy, inflammatory markers
- Discriminator
- Red flags: weight loss, fever, mass
Investigations and Imaging
Imaging Algorithm
Radiographs may be normal for 2-6 weeks after symptom onset. If clinical suspicion is high, proceed directly to MRI. Do not dismiss the diagnosis based on normal XR alone.
- First-line imaging
- May show periosteal reaction, cortical thickening, or fracture line
- Often negative early in disease course
- "Dreaded black line" = anterior cortex stress fracture (late finding)
- Most sensitive for early diagnosis
- Shows bone marrow edema 2-6 weeks before XR changes
- Can grade severity and guide management
- T1: Low signal in marrow
- STIR/T2 fat-sat: High signal in marrow (edema)
Fredericson MRI Grading
- T1 Finding
- Normal
- T2/STIR Finding
- Periosteal edema only
- Clinical Correlation
- Stress reaction - mildest
- T1 Finding
- Normal
- T2/STIR Finding
- Periosteal + marrow edema
- Clinical Correlation
- Stress reaction - moderate
- T1 Finding
- Low signal marrow
- T2/STIR Finding
- Marrow edema + cortical signal
- Clinical Correlation
- Stress fracture - no line
- T1 Finding
- Low signal marrow
- T2/STIR Finding
- Fracture line visible
- Clinical Correlation
- Stress fracture - line visible
- T1 Finding
- Low signal marrow
- T2/STIR Finding
- Complete fracture line
- Clinical Correlation
- Complete stress fracture
- Best for assessing cortical involvement
- Shows "dreaded black line" in anterior cortex fractures
- Useful for surgical planning
- Helpful when MRI unavailable or contraindicated
- Largely replaced by MRI
- Very sensitive but less specific
- "Hot spot" at fracture site
- Can assess multiple sites simultaneously
Management
Treatment Principles
Management depends on risk stratification (location) and grade (MRI findings).
- Relative rest (pain-free activity)
- Cross-training (swimming, cycling)
- Duration: 2-4 weeks
- Gradual return to running
- Weight-bearing as tolerated in walking boot
- No running for 4-6 weeks
- Physical therapy for muscle conditioning
- Gradual return protocol over 2-4 weeks
- Total recovery: 6-8 weeks typically
- Pain-free walking
- Pain-free hopping
- Gradual increase: walk/run program
- No arbitrary time restrictions if pain-free
Proper technique and attention to detail ensure optimal outcomes.
Return to Play Protocol
- Pain-free walking (week 1-2)
- Pain-free hopping/jumping (week 3-4)
- Walk-run program (week 4-6)
- Sport-specific training (week 6-8)
- Full return when pain-free at sport intensity
- Protected weight-bearing until imaging shows healing
- Progressive loading under supervision
- Gradual return over 3-6 months
- Consider prophylactic nailing if early return required
Surgical Technique
Indications for Surgery
- Presence of "dreaded black line" on imaging
- Failed conservative management (3-6 months)
- Elite athlete requiring expedited return
- Complete fracture or displacement
- Established non-union
- Patient preference for definitive treatment
- Active infection at surgical site
- Severe osteoporosis (consider alternative fixation)
- Medical comorbidities precluding surgery
Intramedullary Nailing Technique
- Review CT scan to assess cortical involvement
- Measure tibial length on long-leg films
- Evaluate fracture location relative to planned nail trajectory
- Assess bone quality and canal diameter
- Standard tibial nail (reamed, statically locked)
- Typical nail diameter 8-10mm
- Length based on preoperative templating
- Ensure availability of locking screws
- Discuss risks and benefits of surgery
- Consent for nail removal if symptomatic
- Set realistic expectations for return to sport
- Explain postoperative rehabilitation protocol
Proper technique and attention to detail ensure optimal outcomes.
Intramedullary nailing is the classic operative answer for the recalcitrant anterior cortex ("dreaded black line") stress fracture, but it has drawbacks - it does not lie directly on the tension side, and the trans-tendinous/parapatellar entry causes anterior knee pain in a substantial minority. An increasingly used alternative is anterior tension-band plating: a plate applied directly to the anterior tibial cortex across the fracture.
- It buttresses the tension side exactly where the fracture is, neutralising the tensile load that prevents healing.
- It avoids the anterior knee pain and entry-portal morbidity of the nail and does not violate the knee.
- It can be combined with debridement/drilling of the sclerotic edges and bone grafting.
- Downsides are a larger soft-tissue exposure over a poorly-vascularised anterior surface (wound concerns) and the need for plate removal if prominent.
The exam point: the operative choice for the failed anterior cortex stress fracture is nailing OR anterior tension-band plating (with adjunctive drilling/grafting) - be able to justify either by the tension-band principle.
Complications
Complete Fracture
- Anterior cortex location
- Delayed diagnosis
- Continued activity despite pain
- Dreaded black line ignored
- IM nailing if displaced
- Can treat as typical tibial shaft fracture
- Higher risk of delayed union
Non-union
- Anterior cortex stress fractures
- Delayed treatment
- Nutritional deficiencies
- Smoking
- IM nailing with reaming
- Bone grafting if needed
- Address metabolic factors
Recurrence
Prevention:
- Address underlying risk factors
- Optimize nutrition
- Gradual return to activity
- Correct biomechanical issues
- Appropriate footwear
Postoperative Care
Immediate Postoperative Management
- Weight-bearing as tolerated immediately with IM nail
- Neurovascular checks q4h first 24 hours
- Monitor for compartment syndrome (rare but serious)
- DVT prophylaxis per protocol
- Pain control with multimodal analgesia
- Discharge typically day 1-2
- Keep incisions clean and dry for 2 weeks
- Sutures/staples removed at 14 days
- Watch for signs of infection
Rehabilitation Protocol
- WBAT with crutches as needed for comfort
- ROM exercises immediately
- Ankle pumps, quad sets, straight leg raises
- Ice and elevation for swelling
- Avoid impact activities
- Progress to full weight-bearing without aids
- Advance ROM and strengthening
- Stationary bike when comfortable
- Pool exercises for cardiovascular fitness
- Continue PT 2-3 times per week
- Progressive resistance training
- Begin light jogging if pain-free walking
- Gradual increase in activity per protocol
- Sport-specific exercises after week 8
- Serial radiographs at 6 weeks, 12 weeks
- Return to full training if:
- Pain-free with all activities
- Full ROM
- Radiographic evidence of union
- Functional strength restored
- Return to competition typically 3-4 months
Follow-Up Schedule
- 2 weeks: Wound check, suture removal
- 6 weeks: Clinical exam, radiographs
- 12 weeks: Clinical exam, radiographs, consider return to sport
- 6 months: Final clinical and radiographic assessment
Activity Modification
- Radiographic union (bridging callus on XR)
- Pain-free with high-impact activity
- Full ROM compared to contralateral side
- Functional testing (single-leg hop, agility drills)
- Sport-specific skills without pain
- Address underlying risk factors (nutrition, training errors)
- Monitor for contralateral stress fractures
- Consider nail removal at 12-18 months if symptomatic
- Most nails can remain indefinitely if asymptomatic
Outcomes and Prognosis
Posteromedial (Low-Risk) Outcomes
- Union rate: Over 95% with activity modification
- Average healing time: 6-8 weeks
- Return to sport: 8-12 weeks typically
- Recurrence rate: Less than 5% if risk factors addressed
- Excellent functional outcomes
- Fredericson Grade correlates with healing time
- Grade 1-2: 3-6 weeks return
- Grade 3: 12-16 weeks return
- Nutrition and compliance critical
Anterior Cortex (High-Risk) Outcomes
- Union rate: 50-70% (high failure rate)
- Average healing time: 4-6 months (if successful)
- Non-union risk: 30-50%
- Recurrence common if premature return
- Complete fracture risk if inadequately treated
- Union rate: Over 90% (significantly superior to conservative)
- Average healing time: 3-4 months
- Return to sport: 3-4 months
- Complications: Low (under 5%)
- Excellent functional outcomes
- Lower recurrence with risk factor modification
Prognostic Indicators
- Posteromedial location
- Early diagnosis
- Good nutrition and bone health
- Compliance with activity restriction
- Biomechanical issues addressed
- Anterior cortex location
- Dreaded black line present
- Delayed diagnosis
- Continued activity despite symptoms
- Poor bone health/female athlete triad
- Smoking
Complications and Their Impact
- Occurs in 10-20% of untreated anterior cortex stress fractures
- Requires standard fracture management
- Delays return to sport by 6+ months
- May result in permanent activity restriction
- More common in anterior cortex (30-50% without surgery)
- Requires salvage surgery (IM nail + bone graft)
- Extended recovery (6-12 months)
- May limit return to elite competition
- Overall recurrence rate: 10-20%
- Higher if underlying risk factors not addressed
- Female athlete triad major risk factor
- Training errors most common modifiable cause
Long-Term Outcomes
- Low-risk fractures: Over 95% return to pre-injury level
- High-risk fractures (conservatively treated): 70-80% return to pre-injury level
- High-risk fractures (surgically treated): Over 90% return to pre-injury level
- Elite athletes typically require surgical management for anterior cortex
- Most patients return to full activity without restrictions
- Chronic pain rare if appropriately treated
- Recurrent stress fractures may necessitate activity modification
- Female athlete triad requires ongoing management
Guidelines, Registries & Global Practice
Global Epidemiology
Stress fractures are a worldwide overuse problem in athletes and military recruits, and the tibia is consistently the single most common site. In a 12-month prospective study of competitive track and field athletes the overall incidence was 21.1%, with the tibia accounting for 46% of stress fractures, followed by the navicular (15%) and fibula (12%) [PMID 8775123]. Among female military recruits the reported frequency of stress fractures is in the order of 5-15% during basic training [PMID 18628731]. Female sex, low bone mineral density, menstrual disturbance and low energy availability are the dominant intrinsic risk factors across populations [PMID 8947404].
- Region
- International (US-led, ACSM/AMSSM endorsed)
- Core recommendation
- Cumulative-risk point system; clearance and return-to-play categories; multidisciplinary management of low energy availability
- Evidence basis
- Consensus / expert panel
- Region
- International (Olympic movement)
- Core recommendation
- Screen all athletes (both sexes) for low energy availability; risk-stratified return-to-sport model
- Evidence basis
- Consensus / expert panel
- Region
- International narrative standard
- Core recommendation
- Anterior tibial cortex is high risk: early imaging, non-weight-bearing immobilisation, low threshold for surgery
- Evidence basis
- Narrative review (Level V)
- Region
- International imaging standard
- Core recommendation
- Grade tibial stress injury on MRI to stage severity and guide return-to-activity timing
- Evidence basis
- Level IV correlation study
Guideline Convergence and Practice Variation
There is no single dominant national-society guideline specific to tibial stress fractures; practice is shaped by sports-medicine consensus statements rather than by AAOS, NICE or BOAST documents (which do not address this entity directly). Internationally there is strong agreement on the core principles: MRI is the imaging standard for staging, low-risk posteromedial fractures are managed with relative rest and graded return, and high-risk anterior cortex fractures (the dreaded black line) warrant aggressive management with a low threshold for intramedullary nailing [PMID 26972260] [PMID 15888719]. The main areas of genuine variation are:
- Imaging access — in high-resource settings MRI is obtained early; in limited-resource settings diagnosis often relies on serial radiographs and clinical assessment, with bone scintigraphy where MRI is unavailable.
- Timing of surgery in elite athletes — earlier nailing of anterior cortex fractures is favoured where rapid return to competition is required, whereas a longer trial of non-operative care is common elsewhere.
- Energy-availability screening — increasingly routine in high-performance and military programmes (triad/RED-S frameworks) but still under-recognised in general practice worldwide.
Registry and Preventive Evidence
Joint registries (NJR, AJRR, AOANJRR, SHAR) do not capture stress fractures, so the strongest population-level evidence comes from military and athletic cohort studies. A randomised controlled trial in 5201 female US Navy recruits showed that calcium (2000 mg) and vitamin D (800 IU) daily reduced stress fracture incidence by approximately 20% over 8 weeks [PMID 18433305], supporting nutritional optimisation as a low-cost preventive intervention across all health systems.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“22-year-old female distance runner with 4 weeks of progressive medial shin pain. Pain worse with running, improves with rest. Point tenderness posteromedial tibia. Training for marathon, increased mileage 30% over past month.”
“25-year-old male army recruit with 6 weeks of anterior tibial pain. Initially told to 'push through'. Now has pain at rest. XR shows horizontal radiolucent line in anterior cortex.”
“19-year-old elite gymnast with third stress fracture in 2 years (metatarsal, femoral neck, now tibial). BMI 17.5, amenorrhea for 8 months. Very driven to compete at upcoming nationals.”
MCQ Practice Points
Q: Which tibial stress fracture location is HIGH RISK for non-union?
A: Anterior cortex. This is the tension side of the tibia with poor blood supply. The "dreaded black line" represents a cortical fracture with high non-union risk. Posteromedial (compression side) is LOW RISK.
Q: A runner presents with 3 weeks of tibial pain. XR is normal. What is the next step?
A: MRI. MRI is the gold standard for diagnosis, showing bone marrow edema 2-6 weeks before radiographic changes. Do not dismiss stress fracture based on normal XR.
Q: What is the treatment for an anterior tibial stress fracture with a dreaded black line?
A: Strong consideration for intramedullary nailing. Conservative treatment has 30-50% non-union rate for anterior cortex stress fractures with black line. Prophylactic nailing has over 90% union rate.
Q: What are the components of the female athlete triad?
A: Energy deficiency/eating disorder, amenorrhea, and low bone density/osteoporosis. All three components increase stress fracture risk. Must be addressed holistically - treating fracture alone will lead to recurrence.
Q: What is the primary criterion for return to running after a low-risk tibial stress fracture?
A: Pain-free activity progression - not arbitrary time limits. Patient should be pain-free with walking, then hopping, before gradual walk-run program. Typical timeline is 6-8 weeks but varies by individual.
At a Glance
Tibial stress fractures account for 50% of all stress fractures and are stratified by risk based on location. Anterior cortex = HIGH RISK (tension side, poor blood supply, "dreaded black line" on imaging) - may require prophylactic IM nailing. Posteromedial = LOW RISK (compression side, excellent blood supply) - heals with 6-8 weeks rest. MRI is gold standard for diagnosis, showing bone marrow edema 2-6 weeks before X-ray changes. Always assess for training errors and screen for the female athlete triad (amenorrhea, eating disorder, osteoporosis). Medial tibial stress syndrome (MTSS) is periostitis without fracture line and rarely requires surgery.
- Risk Level
- LOW
- Imaging
- XR first, MRI if negative
- Management
- Rest, gradual return
- Timeline
- 6-8 weeks
- Risk Level
- HIGH
- Imaging
- MRI + CT (black line?)
- Management
- Extended NWB, consider surgery
- Timeline
- 3-6 months
- Risk Level
- CRITICAL
- Imaging
- CT to assess cortex
- Management
- Strong consider IM nail
- Timeline
- Surgical decision
- Risk Level
- LOW
- Imaging
- XR normal, MRI if uncertain
- Management
- Modify activity
- Timeline
- 4-6 weeks
- Risk Level
- HIGH
- Imaging
- MRI for grading
- Management
- Individualized - early surgery option
- Timeline
- Competition-dependent
ANTIStress Fracture Risk Sites
Hook:ANTI sites are AGAINST you - all high-risk for non-union!
COMPPosteromedial - Low Risk
Hook:COMPression side has COMPlete healing potential!
EAOFemale Athlete Triad
Hook:EAO - when you don't EAt enOugh, bones suffer!
TINSTraining Error History
Hook:TINS - Training errors put you in TINS (trouble in numerous spots)!
Risk Stratification
- Anterior cortex = HIGH RISK (tension side)
- Posteromedial = LOW RISK (compression)
- Dreaded black line = surgical consideration
- MTSS = periostitis, not fracture
- Female athlete triad increases risk
Diagnosis
- XR may be normal for 2-6 weeks
- MRI is gold standard
- Fredericson grades 1-4
- CT for cortical assessment
- Point tenderness on exam
Low-Risk Management
- Rest 6-8 weeks
- Cross-training (swim, bike)
- Pain-free progression to return
- Gradual return protocol
- Address training errors
High-Risk Management
- Consider prophylactic IM nail
- Extended NWB (3-6 months) if conservative
- High non-union rate without surgery
- Complete fracture risk if ignored
- Return to sport 3-4 months post-nailing
Prevention/Nutrition
- Calcium 1000-1500mg daily
- Vitamin D over 30 ng/mL
- 10% rule for training increases
- Screen for female athlete triad
- Appropriate footwear
Evidence Base
Reamed IM Nailing for Chronic Anterior Tibial Stress Fractures
- Seven collegiate athletes with 11 chronic anterior midtibial stress fractures, all failing at least 4 months of nonoperative care, achieved clinical union at a mean of 2.7 months and radiological union at 3 months after reamed intramedullary nailing
- Mean return to sport was 4 months with a low complication rate (one insertion-site bursitis, one later traumatic distal tibial fracture)
Fredericson MRI Grading of Tibial Stress Injuries
- In 14 runners (18 symptomatic legs), MRI defined a progression from periosteal oedema through marrow involvement to frank cortical stress fracture, and correlated with an established bone-scan grading system in 14 of 18 legs
- MRI was recommended over bone scintigraphy because it more accurately correlated the degree of bone involvement with clinical symptoms while avoiding ionising radiation
Risk Factors for Stress Fractures in Track and Field Athletes
- In a 12-month prospective study of 111 athletes the stress fracture incidence was 21.1%, with the tibia the most common site
- In female athletes lower bone density, a history of menstrual disturbance, lower lean mass, leg-length discrepancy and a lower-fat diet were significant risk factors; later age of menarche and calf girth were the best independent predictors
Female Athlete Triad Coalition Consensus on Treatment and Return to Play
- The triad comprises low energy availability (with or without disordered eating), menstrual dysfunction and low bone mineral density; low energy availability is the underlying driver
- A cumulative risk-stratification point system guides clearance and return-to-play decisions, with multidisciplinary management and treatment contracts
Calcium and Vitamin D Supplementation in Female Navy Recruits (RCT)
- Randomised, double-blind, placebo-controlled trial in 5201 female Navy recruits: 2000 mg calcium plus 800 IU vitamin D daily reduced stress fracture incidence by 20% over 8 weeks (5.3% vs 6.6%, p=0.0026)
- Smoking, low physical fitness and amenorrhoea were confirmed as additional risk factors
High-Risk Stress Fractures: Diagnosis and Management
- High-risk sites (femoral neck tension side, patella, anterior tibia, medial malleolus, talus, tarsal navicular, proximal fifth metatarsal, great toe sesamoids) share a region of high tensile load and low blood flow, predisposing to delayed union and nonunion
- These require a more aggressive approach: early imaging, non-weight-bearing immobilisation, prolonged time away from sport and a careful return, with surgery often needed
IOC Consensus on Relative Energy Deficiency in Sport (RED-S): 2018 Update
- RED-S extends the female athlete triad to a broader syndrome of impaired physiological function (including bone health and stress-fracture risk) caused by relative energy deficiency, and affects male as well as female athletes
- Provides a clinical assessment and risk-stratified return-to-sport model centred on restoring energy availability