Rare Carpal Fracture | Second Metacarpal Articulation
- Rarest Carpal Fracture: Less than 1% of all carpal fractures.
- Location: Distal carpal row. Articulates with Trapezium, Capitate, Scaphoid, and 2nd MC.
- Protection: The trapezoid is well-protected (recessed in the distal row, keystone of 2nd CMC).
- Mechanism: Axial load through 2nd metacarpal (punch, fall on flexed wrist).
- Treatment: Non-displaced = Cast. Displaced/Dislocated = ORIF.
- “Trapezoid is the RAREST carpal bone to fracture.
- “Look for associated injuries (2nd CMC dislocation, scaphoid fracture).
- “CT is essential for diagnosis and surgical planning.
- “Most non-displaced fractures can be managed with immobilization.
CT is Key. Trapezoid fractures are easily missed on X-ray due to overlapping carpal bones. Get CT if suspicious.
2nd CMC Dislocation. Often associated with 2nd CMC fracture-dislocation. Assess entire carpus.
Keep in Differential. Because it's rare, it may be overlooked. Maintain high suspicion with dorsal wrist pain after axial load.
Post-Traumatic OA. Important for wrist biomechanics. Articular fractures may lead to 2nd CMC arthrosis.
| Bone | Frequency | Key Associated Injury |
|---|---|---|
| Scaphoid | ~70% | Distal Radius, Perilunate |
| Triquetrum | ~15% | Perilunate, Lunate |
| Lunate | ~3% | Kienböck's (if AVN) |
| Trapezium | ~3% | Thumb CMC, Bennett's |
| Capitate | ~2% | Scaphocapitate Syndrome |
| Hamate | ~2% | Hook fracture, Boxer's |
| Trapezoid | less than 1% | 2nd CMC Dislocation |
| Pisiform | ~1% | FCU tendon injury |
She Looks Too Pretty; Try To Catch HerCarpal Bones
Hook:Carpal bone order: Proximal then Distal.
TRAP-2Trapezoid Articulations
Hook:Trapezoid is the keystone of 2nd CMC.
PUNCHMechanism
Hook:Punch injury mechanism.
Overview and Epidemiology
Definition: Trapezoid fractures are fractures of the trapezoid bone, the second bone of the distal carpal row. It is the rarest carpal bone to fracture, accounting for less than 1% of all carpal fractures.
Epidemiology:
- Incidence: Extremely rare.
- Mechanism: Axial load through 2nd metacarpal (punch, fall on flexed wrist).
- Associated Injuries: 2nd CMC dislocation, Perilunate injury, Scaphoid fracture.
Why Rare:
- Trapezoid is recessed within the distal carpal row.
- Protected by surrounding bones.
- Strong ligamentous attachments.
- Keystone of the rigid 2nd CMC joint.
Anatomy and Pathophysiology
Anatomy:
- Location: Distal carpal row. Between trapezium (radial) and capitate (ulnar).
- Shape: Wedge-shaped. Narrow dorsally, wider volarly.
- Articulations:
- Proximal: Scaphoid.
- Distal: 2nd Metacarpal base (key articulation).
- Radial: Trapezium.
- Ulnar: Capitate.
Biomechanics:
- 2nd CMC Joint: Most stable CMC joint (index finger ray). Keystone is the trapezoid.
- Force Transmission: Axial load through 2nd MC can fracture trapezoid.
Blood Supply:
- Enters from dorsal and palmar surfaces.
- AVN is rare.
Classification
Simple Classification
- Non-Displaced: Fracture without significant articular step-off.
- Displaced: Significant displacement or articular incongruity.
- With Dislocation: Associated 2nd CMC or intercarpal dislocation.
- Comminuted: Multiple fragments (often with high-energy).
CT is necessary to classify accurately.
Clinical Assessment
History:
- Mechanism: Punch? Fall on flexed wrist? Axial load?
- Pain Location: Dorsal wrist, over 2nd MC base.
Physical Examination:
- Tenderness: Over trapezoid (dorsal, between 1st and 2nd MC bases).
- Swelling: Dorsal wrist.
- Pain: With axial loading of 2nd metacarpal.
- ROM: Painful wrist flexion/extension.
- Neurovascular: Usually intact.
Investigations
Imaging:
- X-ray (PA, Lateral, Oblique): May show fracture, but often missed due to overlap.
- CT Scan: Essential for diagnosis. Defines fracture pattern, displacement.
- MRI: Rarely needed. For occult fractures or soft tissue assessment.
Key Findings:
- X-ray: Subtle cortical irregularity. Overlap with scaphoid/capitate.
- CT: Clearly delineates fracture. Assess articular involvement.
Management Algorithm
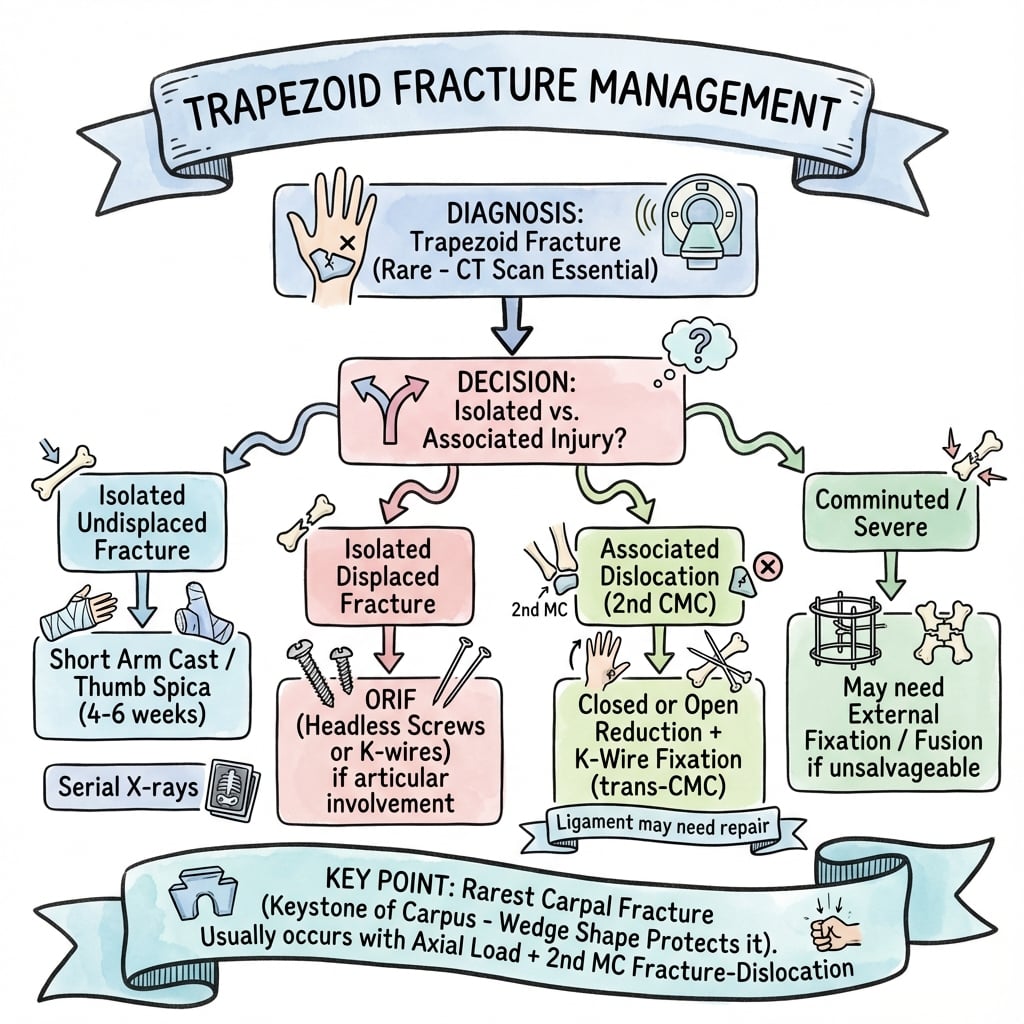
Non-Displaced Fractures
Conservative Management.
- Immobilization: Short arm cast or thumb spica for 4-6 weeks.
- Follow-up: Repeat X-ray/CT at 4-6 weeks for healing.
- Rehabilitation: ROM exercises after cast removal.
Most non-displaced fractures heal well.
Surgical Technique
Dorsal Approach
Incision: Dorsal longitudinal incision centered over 2nd MC base
Structures at Risk:
- Radial artery (anatomical snuffbox)
- Extensor tendons (EPL, ECRL, ECRB)
- Superficial branch radial nerve
Exposure: Capsulotomy between 2nd and 3rd extensor compartments
Complications
| Complication | Risk Factor | Management |
|---|---|---|
| Post-Traumatic Arthrosis | Articular fracture | Fusion (CMC) / Excision |
| Malunion | Inadequate reduction | Osteotomy / Accept |
| Stiffness | Prolonged immobilization | Physiotherapy |
| Non-union | Rare (good blood supply) | Bone graft / Fixation |
Postoperative Care
After Cast/Conservative:
- ROM exercises at 4-6 weeks.
- Strengthen at 6-8 weeks.
After ORIF:
- Splint 2 weeks, then cast/removable splint.
- ROM at 4-6 weeks.
- K-wire removal at 6-8 weeks if used.
Outcomes
- Non-Displaced: Good prognosis with immobilization.
- Displaced/Dislocated: Risk of 2nd CMC arthrosis if not anatomically reduced.
Evidence Base
Relative Incidence of Carpal Fractures
- Prospective audit of 1,000 consecutive hand fractures in Bergen, Norway over ~10 months.
- Carpal bones accounted for 18% of all hand fractures; the scaphoid alone made up 10.6% of the total series.
- Trapezoid fractures were essentially absent from this unselected series, confirming their status as the rarest carpal fracture.
Occult Undisplaced Trapezoid Fracture
- Two cases of isolated, undisplaced trapezoid fracture diagnosed with CT/MRI after negative or equivocal radiographs.
- Authors argue the lesion has historically been under-diagnosed and that modern cross-sectional imaging makes detection more frequent.
- Both undisplaced fractures healed with immobilisation alone.
First True Isolated Trapezoid Fracture
- First reported isolated trapezoid fracture with NO accompanying dislocation or associated metacarpal, carpal or distal radius injury.
- Managed non-operatively with a favourable clinical outcome.
- Reviews presentation, diagnostic workup and treatment of trapezoid fractures generally.
Trapezoid Dislocation — Missed on Plain Films
- Isolated trapezoid dislocation following high-speed motor-vehicle trauma.
- Highlights that these injuries are commonly missed on standard radiographs.
- Management invariably required open reduction and internal fixation.
Palmar Trapezoid Dislocation in Polytrauma
- Rare palmar trapezoid dislocation with associated distal radius fracture in a major-trauma patient.
- Distracting injuries risk misdiagnosis or delayed diagnosis of the carpal component.
- ORIF performed after stabilisation of major injuries yielded satisfactory hand and wrist function.
2nd CMC Fracture-Dislocation with Trapezoid Fracture
- Dorsal 2nd CMC dislocation with trapezoid fracture plus a Rolando fracture after a road-traffic crash.
- Treated by closed reduction with percutaneous K-wires then CT-guided open trapezoid reduction and K-wire fixation.
- Literature review of 71 cases of injuries involving 2nd CMC dislocation; good pain-free outcome at 1 year.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your next step?”
“Answer the question.”
“Provide the ranking.”
MCQ Practice Points
Q: What is the rarest carpal bone to fracture? A: Trapezoid (less than 1% of carpal fractures).
Q: Where is the trapezoid located? A: Distal carpal row. Between the trapezium (radial) and capitate (ulnar). Articulates with the 2nd metacarpal distally.
Q: What is the typical mechanism for trapezoid fracture? A: Axial load through the 2nd metacarpal (e.g., punch injury, fall on flexed wrist).
Q: What is the most common associated injury with trapezoid fractures? A: 2nd CMC (carpometacarpal) fracture-dislocation.
Q: What imaging is best for trapezoid fractures? A: CT scan. X-rays often miss trapezoid fractures due to overlapping bones.
Differential Diagnosis
The trapezoid fracture presents as dorsal wrist pain at the index-ray base after axial load — overlapping with several commoner injuries. CT is the discriminator.
| Diagnosis | Distinguishing Feature | Best Test |
|---|---|---|
| Trapezoid fracture/dislocation | Tenderness at 2nd MC base; pain on axial load of index ray; often missed on plain film | CT |
| 2nd CMC fracture-dislocation | Dorsal prominence of index MC base; cascade-line disruption; commonly coexists | Lateral/oblique radiograph + CT |
| Scaphoid fracture | Anatomical snuffbox and scaphoid tubercle tenderness; radial-sided | Scaphoid views; CT/MRI if occult |
| Trapezium fracture | Thumb-base tenderness; pain on thumb axial load (Bennett-type force) | CT; carpal tunnel/Bett view |
| Wrist sprain (no fracture) | Diffuse tenderness, no bony point tenderness; normal CT | Clinical + negative CT |
Controversies & Areas of Uncertainty
The literature on trapezoid fractures is limited to case reports and small series, so several questions remain unresolved:
- Imaging threshold: There is no consensus on which patients with a "normal" radiograph warrant CT. Most authorities favour a low threshold for cross-sectional imaging given how often the injury is missed, but the cost-effectiveness of routine CT after axial index-ray trauma is undefined.
- Screw vs K-wire fixation: No comparative data exist for displaced fragments. Headless compression screws are preferred for fragments large enough to accept them; K-wires are used for comminuted or small fragments. Choice remains surgeon preference.
- Management of the associated 2nd CMC instability: Whether transarticular K-wiring alone, ligament repair, or temporary CMC fixation gives the best long-term result is unknown — the rarity of the injury precludes trials.
- True incidence: Historical "less than 1%" figures predate routine CT. The real incidence of occult, undisplaced trapezoid fractures is probably higher than classically reported, as several authors have argued.
- Late presentation: Optimal treatment of a missed/chronic trapezoid fracture or dislocation (delayed ORIF vs excision vs limited fusion) is not established.
Guidelines, Registries & Global Practice
There are no condition-specific society guidelines or arthroplasty-registry data for trapezoid fractures given their rarity; practice is governed by general carpal-injury and hand-trauma principles.
Global epidemiology
- Carpal bones contribute roughly 18% of hand fractures, of which the scaphoid dominates (~60% of carpal fractures); the trapezoid is consistently the least frequently fractured carpal bone (classically under 1%).
- Reported cases cluster in young men after high-energy axial mechanisms (punch injury, falls on the flexed wrist, motor-vehicle trauma).
Side-by-side guideline principles
| Body | Relevant Principle |
|---|---|
| BOA / BOAST (UK) | Clinically suspected carpal injury with normal radiographs should be immobilised and re-imaged or progressed to advanced imaging rather than discharged. |
| AAOS / ASSH (US) | Cross-sectional imaging (CT) for occult or complex carpal fractures and pre-operative planning; anatomic reduction of displaced intra-articular carpal fractures. |
| AO Foundation | Articular congruity and stable fixation of displaced carpal fractures; transarticular K-wires for associated CMC instability. |
| EFORT / European consensus | Low threshold for CT in high-energy wrist trauma and polytrauma to avoid missed carpal injuries among distracting fractures. |
High- vs limited-resource practice variation
- Well-resourced settings: Ready CT access enables early detection and ORIF of displaced fractures and associated 2nd CMC dislocations; this is the main reason reported incidence is rising.
- Limited-resource settings: Reliance on plain radiographs means occult and undisplaced trapezoid fractures are frequently missed; immobilisation of the clinically suspicious wrist with delayed re-imaging is a reasonable strategy where CT is unavailable.
- Referral: Displaced fractures and fracture-dislocations warrant referral to a hand/upper-limb surgeon wherever the resource pathway allows.
Key Facts
- Rarest carpal fracture
- less than 1% of carpal fractures
- Distal row (2nd CMC)
- Punch mechanism
Diagnosis
- X-ray often negative (overlap)
- CT is essential for diagnosis
- Tenderness at 2nd MC base
- Pain with axial load of index finger
Treatment
- Non-displaced: Short arm cast 4-6 weeks
- Displaced: ORIF via dorsal approach
- Fixation: Headless screws or K-wires
- Post-op: Cast 4-6 weeks, ROM after healing
Associated
- 2nd CMC dislocation (most common)
- Perilunate injuries (greater arc)
- Scaphoid fractures (high-energy)
- Multiple carpal fractures (assess entire carpus)