Often an Iatrogenic Shoulder Catastrophe
- DELTOID RUPTURE/AVULSION is an uncommon but disabling injury of the shoulder's prime mover; the cause most often described is IATROGENIC - DETACHMENT or avulsion of the deltoid origin from the ANTERIOR and LATERAL ACROMION after OPEN or ARTHROSCOPIC ACROMIOPLASTY or open rotator-cuff surgery - and the resulting insufficiency is a devastating problem causing poor function and debilitating pain. BE PRECISE ABOUT THE ANATOMY: the segment at risk is the anterior part of the ACROMIAL (middle) head, which arises from the acromion; the CLAVICULAR (anterior) head arises from the lateral third of the CLAVICLE and is not what an acromioplasty detaches.
- TREAT 'COMMONEST' WITH CARE - the published literature on this injury is case reports and small series, so there is no denominator. No cohort establishes what proportion of deltoid ruptures are iatrogenic, and no study gives an incidence of deltoid detachment per acromioplasty. What is defensible is that iatrogenic detachment is the mechanism most often REPORTED, not that its frequency has been measured.
- OTHER causes are TRAUMATIC rupture/avulsion (rare, high-energy or in the elderly/atrophic muscle) and secondary deltoid dehiscence or overload in MASSIVE IRREPARABLE ROTATOR CUFF tears, where the deltoid is the principal remaining elevator.
- The clinical consequence is DELTOID INSUFFICIENCY: WEAKNESS of shoulder abduction/elevation, PAIN, a visible or palpable DEFECT/dimple over the deltoid, and ANTEROSUPERIOR ESCAPE of the humeral head (when combined with cuff deficiency) - producing significant functional disability that activities of daily living tolerate poorly.
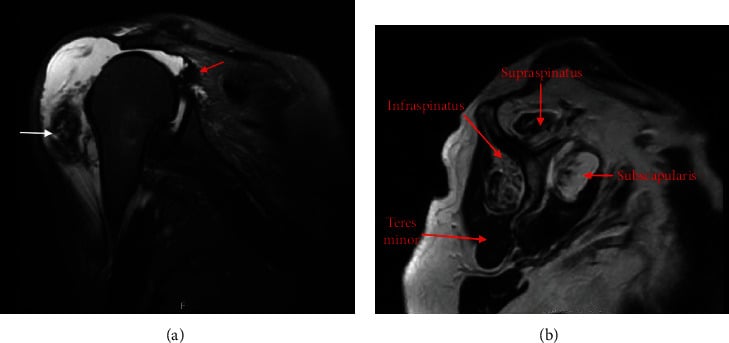
- DIAGNOSIS is by CLINICAL examination (deltoid contour defect, weakness, the operative history) supported by IMAGING - ULTRASOUND and especially MRI to define the deltoid defect, retraction and any associated cuff pathology.
- TREATMENT is difficult: surgical REPAIR/RECONSTRUCTION of the deltoid (direct repair to the acromion - e.g. transosseous/suture-anchor repair - or, for larger/chronic defects, local flap/allograft reconstruction) is undertaken for symptomatic insufficiency, but results are variable and the repair is technically demanding (there are no firmly established standard guidelines) - so realistic expectations are important.
- The dominant clinical message is PREVENTION: during open or arthroscopic acromioplasty and cuff surgery the deltoid ORIGIN must be PROTECTED and, where detached/split, METICULOUSLY REPAIRED (secure deltoid-to-acromion reattachment) - because an iatrogenic deltoid detachment is far easier to avoid than to reconstruct, and a postoperative deltoid defect should be recognised and repaired early rather than left.
- THE PREVENTION ARGUMENT GOES ONE STEP FURTHER THAN TECHNIQUE. A complication of an operation is only worth risking if the operation works. In the CSAW trial - 313 patients, 32 UK hospitals, placebo-controlled - arthroscopic subacromial DECOMPRESSION was no better than arthroscopy alone (Oxford Shoulder Score difference -1.3 points, 95% CI -3.9 to 1.3) and both surgical arms beat no treatment by only 2.8 and 4.2 points against a pre-specified clinically important difference of 4.5. So for subacromial pain with an intact cuff, the surest way to avoid an iatrogenic deltoid injury is to question the indication before questioning the technique.
- “Deltoid rupture/avulsion = uncommon but disabling; the mechanism most often REPORTED is IATROGENIC detachment of the anterior-lateral ACROMIAL origin at acromioplasty/open cuff surgery (the clavicular head comes off the clavicle, not the acromion). Also traumatic / massive-cuff-related. The literature is case reports - there is no measured frequency.
- “Consequence = DELTOID INSUFFICIENCY: weak abduction/elevation, pain, contour defect, anterosuperior escape. Diagnose with examination + MRI/ultrasound.
- “Repair/reconstruction is DIFFICULT (variable results, no firm standard). PREVENTION is key: protect + securely repair the deltoid origin at shoulder surgery; recognise/repair an iatrogenic detachment early.
Most often iatrogenic - anterior-deltoid detachment after acromioplasty/open cuff surgery -> deltoid insufficiency (weak elevation, pain, contour defect, anterosuperior escape).
Repair/reconstruction is difficult with variable results. Prevent it: protect and securely repair the deltoid origin at surgery; recognise and repair an iatrogenic detachment early.
Deltoid Anatomy: Why the Anterior Origin Is Vulnerable
- Three heads. The anterior (clavicular) head arises from the lateral third of the clavicle; the middle (acromial) head from the acromion - a strong multipennate segment and the main power abductor; and the posterior (spinous) head from the scapular spine. All three converge on the deltoid tuberosity of the lateral humerus.
- Which part is actually vulnerable - be precise. It is the acromial (middle) head, and specifically its anterior portion arising from the anterior and lateral acromion, that is resected around, exposed or detached in acromioplasty and in the deltoid-splitting or deltoid-off approaches for open cuff surgery. The clavicular (anterior) head arises from the clavicle, not the acromion, so an acromioplasty does not detach it - which is why the loose shorthand "the anterior deltoid comes off the anterior acromion" misleads. What is lost is the anterior-lateral acromial origin, and because that segment sits directly over the humeral head it is exactly the part whose failure produces weak forward elevation and a visible dimple at the acromial edge.
- Innervation - the axillary nerve. The deltoid is supplied by the axillary nerve (C5-6) from the posterior cord, which passes through the quadrangular space and runs on the deep surface of the deltoid about 5 cm below the acromial edge - which is why a deltoid-splitting approach is limited to roughly 5 cm distal to the acromion to avoid denervating the anterior deltoid.
Q: Describe the deltoid anatomy relevant to its rupture/avulsion.
A: The deltoid has three heads - anterior (clavicular, from the lateral third of the clavicle), middle (acromial, multipennate, the power abductor) and posterior (spinous, from the scapular spine) - converging on the deltoid tuberosity. The part violated at acromioplasty or open cuff surgery is the anterior portion of the acromial (middle) head, arising from the anterior and lateral acromion - not the clavicular head, which comes off the clavicle. Say "the anterior-lateral acromial origin", not "the anterior deltoid comes off the acromion". It is innervated by the axillary nerve (C5-6), which runs on the deep surface about 5 cm below the acromion - so a deltoid-splitting approach is kept within roughly 5 cm of the acromion to avoid denervation.
Detachment versus Axillary Nerve Palsy
A deltoid that is weak and wasted after shoulder surgery has two very different causes - a mechanical deltoid detachment and an axillary nerve palsy - and the distinction changes the treatment entirely.
- Mechanical detachment. A palpable or visible contour defect/dimple, weakness corresponding to the detached segment, normal sensation, and a normal EMG; MRI shows the deltoid defect and retraction. Treated by repair/reconstruction.
- Axillary nerve palsy. Deltoid weakness and wasting without a mechanical defect, often with numbness over the "regimental-badge" area (upper lateral arm over the deltoid), and denervation on EMG/nerve conduction studies; MRI shows diffuse denervation oedema/atrophy rather than a torn origin. Managed by observation/neurolysis, or nerve grafting for a confirmed complete lesion.
- They can coexist (e.g. after a traumatic anterior dislocation or extensive surgery), so seek both a defect and a neurological deficit - EMG/nerve conduction and MRI usually separate them.
The wider context sits on neighbouring pages. The indication that puts the deltoid origin at risk in the first place is discussed under subacromial impingement, where the randomised evidence on decompression is set out in full. The secondary dehiscence pattern belongs with massive rotator cuff tears and, once the head has migrated and the joint has worn, rotator cuff arthropathy; the operative approaches that split the deltoid are covered under rotator cuff tears.
Q: How do you distinguish an iatrogenic deltoid detachment from an axillary nerve palsy?
A: A detachment gives a palpable/visible contour defect, segment-specific weakness, intact sensation and a normal EMG, with MRI showing a torn/retracted origin - treated by repair. An axillary nerve palsy gives deltoid weakness and wasting without a mechanical defect, often numbness over the regimental-badge area, and denervation on EMG/nerve conduction, with MRI showing denervation atrophy - managed by observation/neurolysis or nerve grafting. They can coexist, so seek both; EMG and MRI usually separate them, and the distinction changes the treatment entirely.
Causes, Consequences & Management
Deltoid rupture/avulsion is uncommon but disabling, most often iatrogenic - detachment of the anterior deltoid's anterior-lateral acromial origin (the front of the acromial/middle head) after open/arthroscopic acromioplasty or open cuff surgery - and occasionally traumatic or secondary to massive irreparable cuff failure. The result is deltoid insufficiency: weak abduction/elevation, pain, a contour defect, and anterosuperior escape of the humeral head. Diagnosis is clinical (defect, weakness, operative history) plus MRI/ultrasound. Treatment is difficult - direct repair to the acromion (transosseous/suture-anchor) or flap/allograft reconstruction for larger/chronic defects - with variable results and no firm standard, so the dominant message is prevention: protect and securely repair the deltoid origin at surgery.
The key to deltoid rupture/avulsion is that it is, overwhelmingly, an avoidable complication of shoulder surgery. Because the front of the acromial head takes origin from the anterior and lateral acromion, open and even arthroscopic acromioplasty and open rotator-cuff procedures can detach or devitalise it, and the resulting deltoid insufficiency - weakness of elevation, pain, a contour defect and anterosuperior escape of the humeral head - is poorly tolerated and hard to reverse. Reconstruction (direct acromial reattachment, or flap/allograft for larger chronic defects) is technically demanding with variable results and no firmly established standard, so prevention is paramount: the deltoid origin must be protected during surgery and any necessary deltoid split securely repaired to bone at closure. If a deltoid detachment is recognised after surgery, it is better repaired early, before retraction and atrophy make reconstruction even harder. The injury is also seen, less commonly, after high-energy trauma and as secondary failure in massive irreparable rotator cuff disease, where the deltoid is the last remaining elevator.
Mnemonics & Memory Aids
DELTOID
Hook:DELTOID: Detachment (iatrogenic), Elevation weak, Look for defect/escape, Traumatic/cuff causes, Origin = anterior-lateral acromial, Imaging, Difficult repair (prevent it).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has weak shoulder elevation and a contour defect over the deltoid after a previous acromioplasty. What has happened and how do you manage it?”
Causes
- Iatrogenic (most often reported, never counted): detachment of the anterior-lateral acromial origin at acromioplasty/open cuff surgery
- Traumatic (rare); secondary to massive irreparable rotator cuff tear
- The acromial (middle) head arises from the acromion; the clavicular head from the clavicle
- Prevention starts with the indication: CSAW found decompression no better than placebo for subacromial pain with an intact cuff
Consequence & diagnosis
- Deltoid insufficiency: weak abduction/elevation, pain, contour defect
- Anterosuperior escape of the humeral head (with cuff deficiency)
- Examination + operative history; MRI/ultrasound (defect/retraction)
Management
- Difficult repair/reconstruction (direct acromial reattachment; flap/allograft for large/chronic) - variable results
- No firmly established standard technique
- Prevention is key: protect + securely repair the deltoid origin; repair an iatrogenic detachment early
Evidence & Key Studies
Delayed surgical repair of the deltoid following acromioplasty
- Because part of the anterior deltoid originates from the anterior acromion, there is a risk of violation and iatrogenic rupture/avulsion during arthroscopic acromioplasty.
- Deltoid insufficiency following acromioplasty can be a devastating problem leading to poor function and debilitating pain.
- Surgical repair (here, arthroscopic evaluation followed by open deltoid repair) improved pain and disability, but there are no standard guidelines and the suture-repair technique is one option for this difficult injury.
Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial
- 313 patients across 32 UK hospitals and 51 surgeons with subacromial pain for at least 3 months, intact cuff tendons, and a completed non-operative programme including exercise and at least one steroid injection, randomised 1 to 1 to 1 between decompression, investigational arthroscopy alone as a placebo, and no treatment.
- At 6 months the Oxford Shoulder Score did not differ between decompression and placebo arthroscopy (mean difference -1.3 points, 95% CI -3.9 to 1.3, p=0.31). Both surgical arms exceeded no treatment by 2.8 and 4.2 points, below the pre-specified clinically important difference of 4.5, and that gap may reflect placebo effect or postoperative physiotherapy.
- The trial excluded full-thickness cuff tears and had substantial crossover (23, 42 and 12 percent did not receive the assigned treatment by 6 months), so it does not speak to decompression performed alongside a cuff repair - but for isolated subacromial pain it questions the value of the operation.
The iatrogenic mechanism of deltoid rupture/avulsion (anterior-deltoid violation during arthroscopic acromioplasty because it originates from the anterior acromion), its devastating functional/pain consequences, and the difficulty of surgical repair (no standard guidelines) come from the cited Sherwani report. The randomised evidence questioning the value of isolated subacromial decompression comes from the CSAW trial. The deltoid-insufficiency clinical picture (weakness, contour defect, anterosuperior escape), the traumatic and massive-cuff-related causes, the deltoid's segmental origins, the MRI/ultrasound diagnosis, and the prevention principle (protect and securely repair the deltoid origin) are standard, well-established teaching. The published literature on deltoid rupture itself is case reports and small series: there is no cohort giving the proportion of deltoid ruptures that are iatrogenic, no incidence per acromioplasty, and no comparative series establishing one repair technique over another, so none of those figures is quoted here.