Epithelioid Haemangioma & Haemangioendothelioma
- The EPITHELIOID VASCULAR TUMOURS OF BONE form a SPECTRUM of increasing aggressiveness: the BENIGN (locally aggressive) EPITHELIOID HAEMANGIOMA, the INTERMEDIATE-grade EPITHELIOID HAEMANGIOENDOTHELIOMA (EHE), and the HIGH-GRADE malignant ANGIOSARCOMA - so grading the lesion is central to management and prognosis.
- EPITHELIOID HAEMANGIOMA is a BENIGN vascular tumour (locally aggressive) composed of well-formed vessels lined by plump EPITHELIOID endothelial cells; in bone it appears as a lytic, sometimes expansile and often MULTIFOCAL lesion, and is generally treated successfully by curettage or excision with a low recurrence rate.
- EPITHELIOID HAEMANGIOENDOTHELIOMA (EHE) is an INTERMEDIATE, low-to-moderate-grade MALIGNANT vascular tumour characterised molecularly by the WWTR1-CAMTA1 gene fusion (with a less common YAP1-TFE3 variant); it typically occurs in bone, soft tissue, liver and lung and is frequently MULTIFOCAL, and its behaviour ranges from relatively indolent to metastatic - so it cannot be assumed benign.
- DO NOT LEAVE 'VARIABLE BEHAVIOUR' UNSTRATIFIED - AND DO NOT LET MULTIFOCALITY DO THE STRATIFYING. In a 62-case series with confirmed CAMTA1/TFE3/WWTR1 alterations, 5-year overall survival was 78.8 percent, and survival did NOT correlate with age, sex, tumour site, MULTIFOCALITY or MULTIORGAN involvement. The two independent predictors were TUMOUR SIZE OVER 30 MM and ATYPICAL HISTOLOGY (at least 2 of: high mitotic activity, high nuclear grade, coagulative necrosis - present in 35.5 percent). A three-tier system built on those two separated 5-year overall survival of 100 PERCENT, 81.8 PERCENT and 16.9 PERCENT. A small synaptophysin-positive subset (6.4 percent) fell entirely in the high-risk group.
- These tumours are of ENDOTHELIAL origin, confirmed by VASCULAR immunomarkers (CD31, ERG, FLI1, CD34); EHE additionally shows nuclear CAMTA1 expression reflecting the WWTR1-CAMTA1 fusion, which is a valuable diagnostic discriminator from other epithelioid lesions (including metastatic carcinoma, which the epithelioid morphology can mimic).
- A characteristic clinical feature is MULTIFOCALITY - multiple lytic lesions, often clustered in one region or limb (or one anatomic region across organs) - which can be mistaken for metastatic disease; the differential includes metastasis, other vascular tumours, and (at the malignant end) ANGIOSARCOMA, which must be excluded because it is highly aggressive. Multifocality is a DIAGNOSTIC clue, not a prognostic one - it did not predict survival in the largest series, so a patient with several lesions should not be counselled as though that alone were the bad sign.
- MANAGEMENT is driven by GRADE and EXTENT: localised epithelioid HAEMANGIOMA is treated by CURETTAGE/EXCISION; EHE is treated by WIDE RESECTION where resectable, with SYSTEMIC THERAPY and multidisciplinary management for multifocal/metastatic or unresectable disease (and surveillance given variable behaviour); ANGIOSARCOMA requires aggressive multimodality treatment - all coordinated through a specialist sarcoma centre.
- “Epithelioid vascular tumours of bone are a SPECTRUM: epithelioid HAEMANGIOMA (benign/locally aggressive) -> epithelioid HAEMANGIOENDOTHELIOMA/EHE (intermediate malignant) -> ANGIOSARCOMA (high-grade malignant). Grade is central.
- “Often MULTIFOCAL lytic lesions (mimic metastases). Endothelial markers (CD31/ERG/FLI1). EHE = WWTR1-CAMTA1 fusion (nuclear CAMTA1; YAP1-TFE3 variant).
- “Management by grade/extent: curettage/excision (haemangioma) -> wide resection +/- systemic therapy (EHE, esp. multifocal/metastatic) -> aggressive multimodality (angiosarcoma). Specialist sarcoma centre.
- “Stratify EHE properly: 5-year survival 78.8% overall (n=62), but 100% / 81.8% / 16.9% by SIZE over 30mm and ATYPICAL HISTOLOGY. Multifocality and multiorgan involvement did NOT predict survival. Ask for synaptophysin - the 6.4% expressing it were all high-risk.
Epithelioid haemangioma (benign) -> epithelioid haemangioendothelioma/EHE (intermediate malignant, WWTR1-CAMTA1) -> angiosarcoma (high-grade). Grade determines treatment and prognosis.
Often multifocal lytic lesions that mimic metastases. Confirm endothelial origin (CD31/ERG) and EHE fusion (nuclear CAMTA1); exclude angiosarcoma.
The Spectrum & Diagnosis
The epithelioid vascular tumours of bone span from the benign (locally aggressive) epithelioid haemangioma, through the intermediate-grade epithelioid haemangioendothelioma (EHE) with its WWTR1-CAMTA1 fusion, to the high-grade angiosarcoma. They are endothelial (CD31, ERG, FLI1, CD34), present as lytic, often multifocal bone lesions (which can mimic metastases), and EHE shows nuclear CAMTA1. Grading is central: epithelioid haemangioma is benign with low recurrence after curettage/excision, EHE is malignant with variable (indolent to metastatic) behaviour, and angiosarcoma is highly aggressive and must be excluded.
- Grade
- Benign (locally aggressive)
- Key features
- Plump epithelioid endothelium; lytic, often multifocal; curettage/excision, low recurrence
- Grade
- Intermediate (low-moderate malignant)
- Key features
- WWTR1-CAMTA1 (YAP1-TFE3 variant); bone/soft tissue/liver/lung; multifocal; variable behaviour
- Grade
- High-grade malignant
- Key features
- Aggressive, poor prognosis - the lesion to exclude
Histology and Imaging That Grade the Spectrum
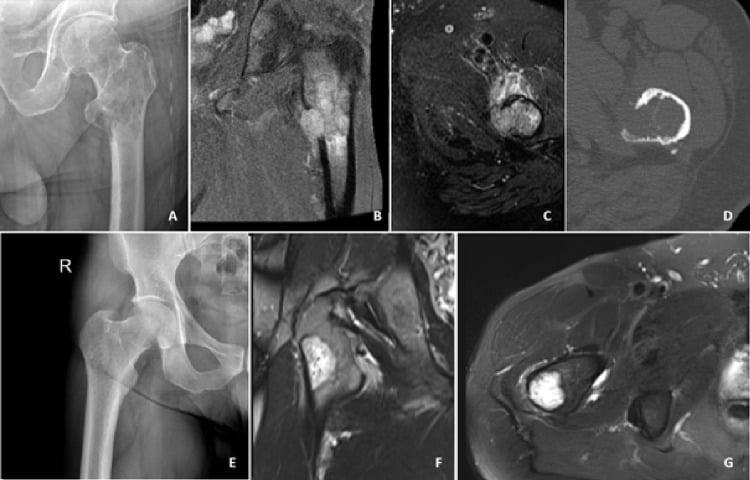
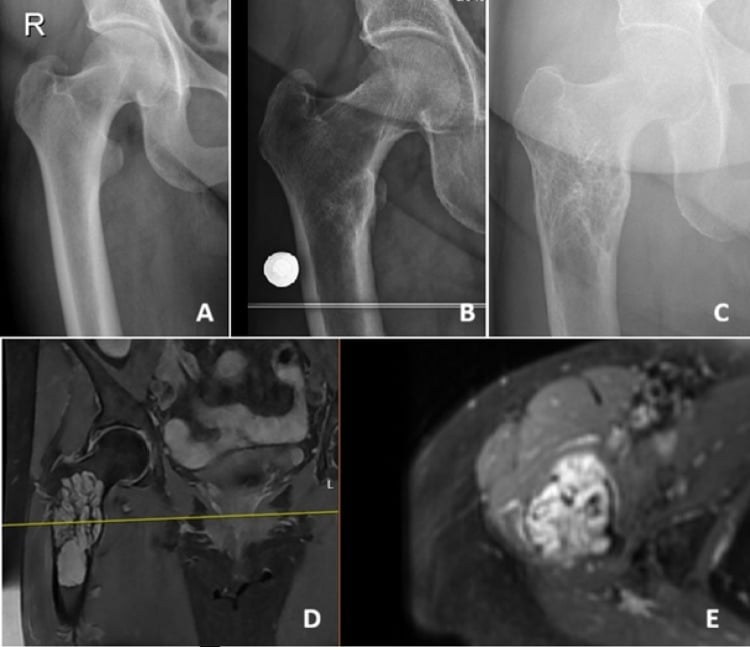
- The radiographic pattern. All appear as lytic bone lesions: epithelioid haemangioma is often well-defined (sometimes expansile/multiloculated, occasionally with a sclerotic rim); EHE is lytic and may be more permeative with cortical destruction. The multifocal lesions cluster regionally - several bones of one limb or anatomic region - which is the hallmark that distinguishes them from randomly scattered metastases.
- The histology that grades it. Epithelioid haemangioma - well-formed vessels lined by plump epithelioid endothelium, often an eosinophil-rich background, minimal atypia. EHE - cords and nests of epithelioid cells in a distinctive myxohyaline (chondroid-like) stroma, with the classic intracytoplasmic vacuoles / primitive lumina ("blister cells") that may contain red cells, and mild-to-moderate atypia. Angiosarcoma - anastomosing channels, marked atypia, high mitoses and necrosis.
Q: What histological features distinguish the epithelioid vascular tumours of bone?
A: Epithelioid haemangioma - well-formed vessels + plump epithelioid endothelium, eosinophil-rich background, minimal atypia. EHE - cords/nests of epithelioid cells in a myxohyaline stroma with intracytoplasmic vacuoles / primitive lumina ("blister cells"), mild-moderate atypia. Angiosarcoma - anastomosing channels, marked atypia, high mitoses, necrosis. Radiographically all are lytic; the multifocal lesions cluster regionally (one limb) unlike scattered metastases.
Stratifying EHE: What Actually Predicts Survival
"Behaviour ranges from indolent to metastatic" is the honest starting point, but it is not an answer, and the factor most people reach for turns out to be the wrong one. In a series of 62 EHEs with confirmed CAMTA1, TFE3 or WWTR1 alterations, overall 5-year survival was 78.8 percent - and survival did not correlate with age, sex, tumour site, multifocality or multiorgan involvement. The two factors that did, on both univariate and multivariate analysis, were tumour size greater than 30 mm and atypical histology, defined as at least two of high mitotic activity, high nuclear grade and coagulative necrosis. A three-tier system built from those two separated the cohort sharply.
- Defined by
- Neither factor: 30 mm or smaller and no atypical histology
- 5-year overall survival
- 100 percent
- Defined by
- One factor: either size over 30 mm or atypical histology
- 5-year overall survival
- 81.8 percent
- Defined by
- Both factors: size over 30 mm and atypical histology
- 5-year overall survival
- 16.9 percent
- Defined by
- Synaptophysin expression (6.4 percent of cases) - all fell in the high-risk group
- 5-year overall survival
- Aggressive course
Q: A patient has EHE with several lesions in one limb. What determines the prognosis?
A: Not the number of lesions. Multifocality and multiorgan involvement did not predict survival; size over 30 mm and atypical histology (two or more of high mitoses, high nuclear grade, coagulative necrosis - seen in about a third of cases) did, and together they separate 5-year survival of 100, 81.8 and 16.9 percent across low, intermediate and high risk. So the pathology report, not the lesion count, drives the conversation - and a request for synaptophysin is worth making, since the small subset expressing it behaved aggressively and lay entirely within the high-risk group. The caveats: this is a single retrospective series of 62 patients with a median follow-up of only 34 months, drawn from all sites rather than bone alone, and the system has not been validated prospectively.
Management
- Epithelioid haemangioma (benign): curettage (with grafting) or excision - low recurrence.
- EHE (intermediate malignant): wide resection where resectable; systemic therapy and multidisciplinary management for multifocal/metastatic or unresectable disease; surveillance given variable behaviour.
- Angiosarcoma: aggressive multimodality treatment.
- All: confirm endothelial origin (CD31/ERG) and EHE fusion (nuclear CAMTA1); exclude metastatic carcinoma (epithelioid mimic) and angiosarcoma; manage at a specialist sarcoma centre; planned biopsy before definitive surgery.
- Ask the pathologist for the risk factors, not just the diagnosis: maximum dimension, whether the histology is atypical (mitoses, nuclear grade, necrosis), and synaptophysin - these, not the number of lesions, are what the prognosis turns on.
The two ends of the spectrum have their own pages. The high-grade lesion that must be excluded is covered under angiosarcoma, and the pattern these tumours are most often mistaken for under metastatic bone disease. The simple vascular lesion at the far benign end, with its characteristic corduroy and polka-dot appearances, is haemangioma of bone, and in the spine vertebral haemangioma - neither is part of the epithelioid group but both enter the differential of a lytic vascular lesion.
The central caution with epithelioid vascular tumours of bone is that they form a spectrum, and the benign epithelioid haemangioma, the intermediate-grade epithelioid haemangioendothelioma and the high-grade angiosarcoma can look similar (epithelioid endothelial cells, lytic often multifocal bone lesions), so the grade must be established rather than assumed. Multifocality is characteristic and can be mistaken for metastatic disease, which should not lead to nihilism, while the epithelioid morphology can mimic metastatic carcinoma, which must be excluded with vascular immunomarkers (CD31, ERG) and, for EHE, the nuclear CAMTA1/WWTR1-CAMTA1 fusion. Crucially, angiosarcoma - the highly aggressive malignant end of the spectrum - must be excluded, because it changes both prognosis and treatment. Management is therefore grade- and extent-based and best delivered through a specialist sarcoma multidisciplinary team, with a properly planned biopsy before any definitive surgery.
Molecular Signatures Across the Spectrum
- Epithelioid haemangioma. Carries a FOS gene rearrangement (and, in a subset, FOSB), especially in bone and cellular/atypical cases; the FOSB immunostain can be positive. This is distinct from the EHE fusion and helps confirm the benign end.
- Epithelioid haemangioendothelioma. The WWTR1-CAMTA1 fusion from t(1;3)(p36;q25) in about 90%, reflected in nuclear CAMTA1; the less common YAP1-TFE3 variant (younger patients, more vasoformative, TFE3-positive).
- A related FOSB entity. Pseudomyogenic (epithelioid-sarcoma-like) haemangioendothelioma carries a SERPINE1-FOSB fusion (and is FOSB-positive) - typically a young male with multifocal lesions in one limb; worth knowing as the other FOSB-driven vascular tumour.
Q: What are the molecular signatures across the epithelioid vascular tumour spectrum?
A: Epithelioid haemangioma (benign) - FOS (or FOSB) rearrangement (FOSB immunostain). EHE (intermediate malignant) - WWTR1-CAMTA1 t(1;3) in ~90% (nuclear CAMTA1), with a YAP1-TFE3 variant (TFE3+). Pseudomyogenic HE - SERPINE1-FOSB. So the fusion partner (CAMTA1 vs the FOS/FOSB family) helps place the tumour on the spectrum.
Mnemonics & Memory Aids
VESSEL
Hook:VESSEL: Vascular/endothelial, Epithelioid cells, Spectrum (benign->EHE->angiosarcoma), Several lesions, EHE fusion (CAMTA1), Lytic - treat by grade.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Multiple lytic lesions are found in the bones of one limb in a young adult, and biopsy shows an epithelioid vascular tumour. How do you think about this?”
The spectrum
- Epithelioid haemangioma: benign (locally aggressive)
- Epithelioid haemangioendothelioma (EHE): intermediate-grade malignant
- Angiosarcoma: high-grade malignant (exclude it)
Features & diagnosis
- Lytic bone lesions, often multifocal (mimic metastases)
- Endothelial markers: CD31, ERG, FLI1, CD34
- EHE: WWTR1-CAMTA1 fusion (nuclear CAMTA1); YAP1-TFE3 variant; occurs in bone/soft tissue/liver/lung
Management
- Epithelioid haemangioma: curettage/excision (low recurrence)
- EHE: wide resection if resectable; systemic therapy + MDT/surveillance for multifocal/metastatic (no agent proven in a trial)
- EHE prognosis: size over 30mm + atypical histology -> 5-yr survival 100 / 81.8 / 16.9%; multifocality does NOT predict it
- Angiosarcoma: aggressive multimodality; planned biopsy; sarcoma-centre care; exclude metastatic carcinoma
Evidence & Key Studies
Epithelioid haemangioendothelioma - a rare vascular neoplasm (multimodal imaging)
- Epithelioid haemangioendothelioma (EHE) is a rare vascular neoplasm that typically occurs in the bone, soft tissue, liver and lung.
- Its imaging is poorly understood and often leads to misdiagnosis as other tumours; lesions can be well-defined soft-tissue masses with calcification and heterogeneous enhancement and can be FDG-avid on PET-CT.
- Diagnosis was confirmed pathologically, and EHE should be considered in the differential of such masses - underscoring that it is a malignant vascular tumour requiring tissue diagnosis.
Clinicopathologic characterization of epithelioid hemangioendothelioma in a series of 62 cases: a proposal of risk stratification and identification of a synaptophysin-positive aggressive subset
- Retrospective cohort of 62 EHEs with confirmed CAMTA1 (59 cases), TFE3 (2) or variant WWTR1-ACTL6A (1) alterations. Atypical histology - at least two of high mitotic activity, high nuclear grade and coagulative necrosis - was present in 22 tumours (35.5 percent). Over a median follow-up of 34 months, 11 patients (18 percent) died and 5-year overall survival was 78.8 percent.
- Survival did not correlate with age, sex, tumour site, multifocality or multiorgan involvement. On univariate and multivariate analysis, only tumour size greater than 30 mm and atypical histology were significantly associated with shorter survival.
- A three-tier system using those two factors stratified 5-year overall survival at 100, 81.8 and 16.9 percent for low, intermediate and high risk. Four tumours (6.4 percent) expressed synaptophysin; all were high-risk and pursued an aggressive course. The series is retrospective, single-institution, covers all anatomical sites rather than bone alone, and the system is not prospectively validated.
The nature of epithelioid haemangioendothelioma as a rare vascular neoplasm occurring in bone, soft tissue, liver and lung, its tendency to be misdiagnosed (requiring tissue diagnosis), and its malignant/FDG-avid behaviour come from the cited Chen report. The spectrum of epithelioid vascular tumours (benign epithelioid haemangioma -> intermediate EHE -> high-grade angiosarcoma), the endothelial immunophenotype (CD31/ERG/FLI1), the WWTR1-CAMTA1 (and YAP1-TFE3) fusion of EHE with nuclear CAMTA1, the multifocal lytic bone presentation, and the grade-/extent-based management are standard, well-established teaching. The survival figures, the risk stratification by size and atypical histology, the absence of prognostic weight for multifocality, and the synaptophysin-positive subset come from the Shibayama series. No randomised trial establishes a systemic agent for unresectable or metastatic EHE, so although systemic therapy is part of multidisciplinary care, no specific drug is recommended here as though its benefit were proven; nor is there a validated surveillance interval, a size threshold that mandates resection over observation, or an outcome series specific to the bone-only subgroup.