Glenoid Track in Shoulder Instability
- Bone loss in anterior shoulder instability is BIPOLAR: it involves both the anterior GLENOID (a bony Bankart fragment or attritional/erosive loss) and the posterosuperior humeral head (a HILL-SACHS impaction lesion), and because the two interact during instability, both must be assessed TOGETHER rather than in isolation.
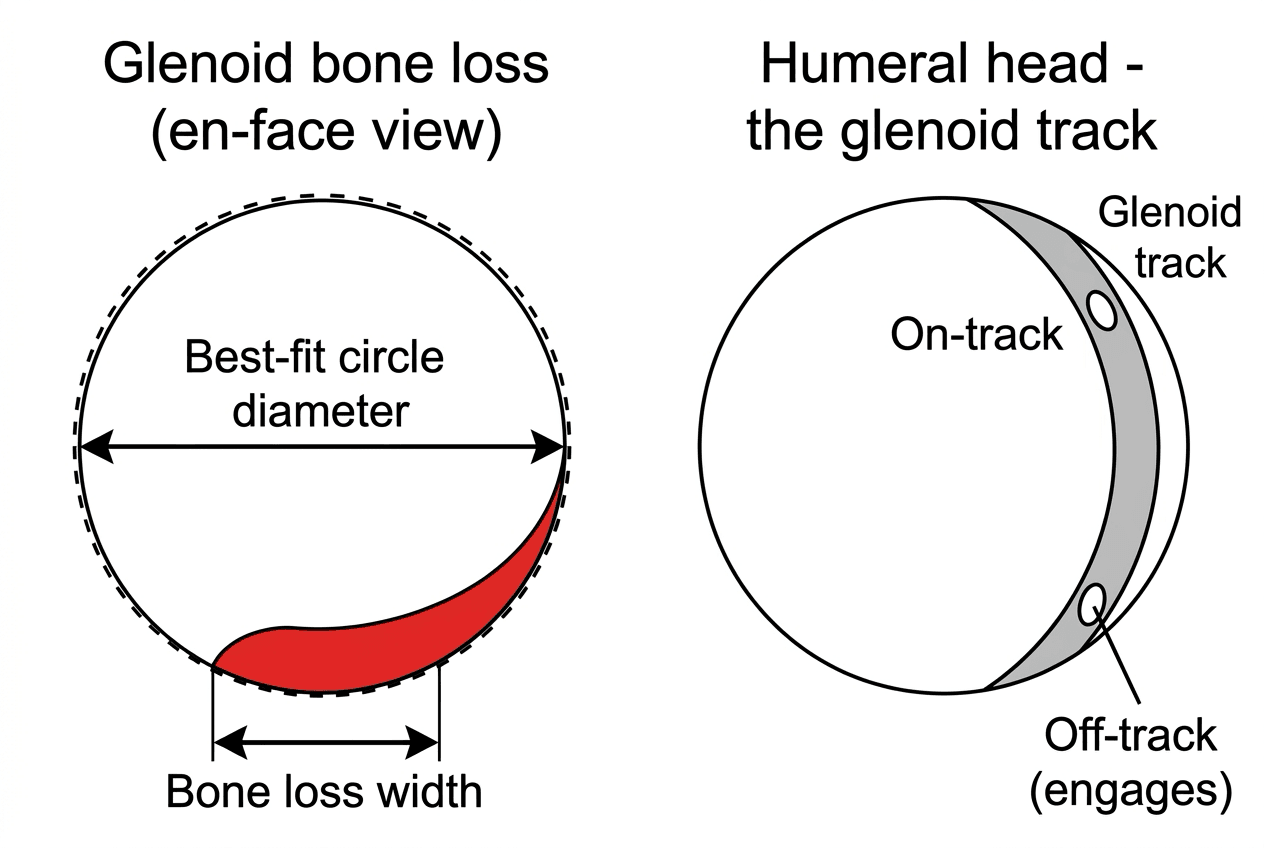
- GLENOID bone loss is quantified on an EN-FACE (sagittal-oblique) reconstruction using a best-fit circle of the inferior glenoid (the inferior glenoid is normally a near-perfect circle), expressing the defect as a percentage of the circle; 3D CT is the GOLD STANDARD for this static assessment, and 3D MRI has been validated as a reliable alternative (with the advantage of also assessing soft tissues).
- Recognised THRESHOLDS guide management: 'critical' glenoid bone loss is classically around 20-25% (above which an isolated soft-tissue Bankart repair has unacceptably high failure), and there is now emphasis on 'SUBCRITICAL' bone loss (around 13.5-20%), where outcomes of isolated Bankart repair are already compromised and augmentation should be considered.
- The GLENOID TRACK concept (Yamamoto/Di Giacomo) is the key dynamic, bipolar tool: the glenoid track is the zone of contact of the glenoid on the humeral head in the provocative abduction-external rotation position (its width is approximately 0.83 times the glenoid diameter minus the glenoid bone-loss width); if the Hill-Sachs lesion extends MEDIAL to the medial margin of the track it is 'OFF-TRACK' and will ENGAGE the glenoid rim (high recurrence risk), whereas if it stays within the track it is 'ON-TRACK'.
- These measurements DRIVE the surgical choice: an ON-TRACK lesion with minimal glenoid bone loss is suitable for an isolated arthroscopic BANKART repair; an OFF-TRACK Hill-Sachs (or significant bipolar loss) needs the Hill-Sachs addressed - typically a Bankart plus REMPLISSAGE (filling the Hill-Sachs with posterior capsule/infraspinatus) - and significant GLENOID bone loss (around 20% or more, or subcritical loss with an off-track lesion or other risk factors) needs a BONY procedure such as a LATARJET (coracoid transfer) or bone block.
- Accurate, reproducible assessment matters because under-estimating bone loss leads to recurrent instability after an inadequate soft-tissue repair: 3D CT (or validated 3D MRI) should be used to measure glenoid bone loss and the Hill-Sachs and to compute the glenoid track / on-off-track status as part of preoperative planning, integrated with clinical risk factors (age, sport, hyperlaxity) and instability scores.
- “Bone loss is BIPOLAR: anterior GLENOID (bony Bankart) + posterosuperior humeral head (HILL-SACHS) - assess BOTH together.
- “Quantify glenoid loss on EN-FACE 3D CT (gold standard; 3D MRI validated) with a best-fit inferior-glenoid circle; subcritical ~13.5-20%, critical ~20-25%.
- “GLENOID TRACK: track width ~0.83 x glenoid diameter - glenoid bone-loss width; Hill-Sachs medial to the track = OFF-TRACK (engages). Drives Bankart (on-track) vs +remplissage (off-track) vs Latarjet (significant glenoid loss).
Bone loss is bipolar (glenoid + Hill-Sachs). Measure glenoid loss on en-face 3D CT (gold standard) with a best-fit inferior-glenoid circle; subcritical ~13.5-20%, critical ~20-25%.
Compute the glenoid track: a Hill-Sachs medial to the track margin = OFF-TRACK (engages, high recurrence). This drives Bankart vs remplissage vs Latarjet.
Bipolar Bone Loss, Quantification & the Glenoid Track
Bone loss in anterior instability is bipolar - both the anterior glenoid (bony Bankart/attritional loss) and the posterosuperior humeral head (Hill-Sachs) - and the two interact, so both are assessed together. Glenoid bone loss is quantified on an en-face (sagittal-oblique) 3D CT with a best-fit circle of the inferior glenoid (3D CT is the gold standard; 3D MRI is a validated alternative); thresholds are subcritical (~13.5-20%) and critical (~20-25%). The glenoid track concept is the key dynamic tool: the track is the glenoid's contact zone on the humeral head in abduction-external rotation (width approximately 0.83 x glenoid diameter minus the glenoid bone-loss width); a Hill-Sachs lesion medial to the medial margin of the track is OFF-TRACK (it engages the rim, high recurrence) whereas one within the track is ON-TRACK. These measurements drive the surgical choice.

- Bone status
- Glenoid loss minimal; Hill-Sachs on-track
- Typical procedure
- Arthroscopic Bankart repair
- Bone status
- Hill-Sachs engages; glenoid loss subcritical
- Typical procedure
- Bankart + remplissage
- Bone status
- Glenoid loss ~20%+ (or subcritical + off-track / high risk)
- Typical procedure
- Bony procedure (Latarjet / bone block)
- Bone status
- Large glenoid + large Hill-Sachs
- Typical procedure
- Latarjet (+/- humeral-side procedure)
How the Numbers Drive Surgery
- On-track, minimal glenoid loss: isolated arthroscopic Bankart repair.
- Off-track Hill-Sachs (with subcritical glenoid loss): address the Hill-Sachs - Bankart + remplissage (fill the Hill-Sachs with posterior capsule/infraspinatus) to make it functionally on-track.
- Significant glenoid bone loss (~20% or more, or subcritical loss with an off-track lesion / high-risk patient): a bony procedure - Latarjet (coracoid transfer, restoring glenoid arc + the sling effect) or a glenoid bone block.
- Integrate clinical risk: age, sport (contact/collision), hyperlaxity and instability scores modify the thresholds.
- Measure accurately: use 3D CT (or validated 3D MRI) for glenoid loss, the Hill-Sachs and the glenoid track preoperatively - under-estimating bone loss is a key cause of recurrence.
The central error in shoulder instability surgery is performing an isolated soft-tissue Bankart repair while under-estimating or ignoring bone loss, because an off-track Hill-Sachs or significant glenoid bone loss will cause the repair to fail with recurrent instability. The bone loss is bipolar, so both the glenoid and the Hill-Sachs must be measured and combined in the glenoid-track assessment: a Hill-Sachs that is off-track, or glenoid bone loss in the subcritical-to-critical range, signals that the soft-tissue repair needs augmentation - remplissage for the engaging Hill-Sachs, and a bony procedure such as a Latarjet for significant glenoid loss. Use 3D CT (or validated 3D MRI) to quantify bone loss and compute on/off-track status preoperatively, and integrate clinical risk factors, rather than deciding from a plain film alone.
How Glenoid Bone Loss Is Actually Measured
Quantifying glenoid loss needs a defined technique, not just a percentage. Because the inferior two-thirds of the glenoid is normally a near-perfect circle, on the en-face (sagittal-oblique) view you fit a best-fit circle to the intact inferior glenoid - or, most accurately, use the contralateral normal glenoid as a one-to-one template. There are then two main methods, and they do not give the same number:
- Width (linear) method - the width of the defect as a fraction of the circle's diameter. Quick, but it tends to slightly over-read the percentage compared with the area method.
- Surface-area (Pico) method - the area of the missing segment as a fraction of the circle's total area, often referenced against the contralateral glenoid surface.
Because the same defect yields a different percentage by each method, always state which method you used when quoting a value against the subcritical/critical thresholds. The type of loss matters as much as the amount: a discrete bony-Bankart fragment may be repairable/incorporated if it is of adequate size and unites, whereas purely attritional/erosive loss has no fragment to fix and generally behaves worse - so describe both the amount and the morphology. (The bony-Bankart lesion itself is covered in Bankart Lesions and Glenoid Fractures; the point here is the measurement.)
The plain films still have named jobs
Radiographs do not quantify bone loss, but "don't decide from a plain film" is not the same as "don't take one", and a viva will ask which views:
- AP in external rotation and the Stryker notch view profile the Hill-Sachs lesion.
- The West Point axillary is the plain view for the anteroinferior glenoid rim - it projects the anteroinferior quadrant free of overlap and shows rim erosion or a bony fragment.
- The Bernageau (glenoid profile) view shows the anterior glenoid rim in profile and demonstrates the "cliff" or blunting of erosive loss.
- A standard AP may show loss of the normal glenoid contour, which is one of the ISIS points above.
Two further recognitions belong here. At arthroscopy, the "inverted pear" glenoid - where the normally pear-shaped glenoid loses its wider inferior half and looks like an upside-down pear - corresponds to substantial loss, conventionally quoted in the region of 25 to 30%, and is the intra-operative equivalent of the critical threshold. And the contralateral-template method has a limit worth stating: it assumes side-to-side symmetry, which is generally but not universally true, and it is unusable in the patient with bilateral instability - so a best-fit circle on the affected side is the fallback.
Fit a best-fit inferior-glenoid circle (or a contralateral template) and quantify by the width/linear method (slightly over-reads) or the surface-area/Pico method (area-based) - state which, because the percentage differs. Distinguish a repairable bony-Bankart fragment from worse-behaving attritional loss.
Why There Are Two Thresholds, and What Each One Means
The subcritical band around 13.5-20% and the critical one around 20-25% are not two guesses at the same number - they measure two different failures, and knowing which is which is the examinable point.
The distinction comes from the quartile analysis that coined the term. Recurrent dislocation rose sharply only in the highest quartile: failure was 7.3% below about 20% bone loss versus 27.8% above it, so the classical 20-25% "critical" figure is a re-dislocation threshold. But patient-reported function deteriorated much earlier. Above about 13.5%, WOSI scores fell to a level consistent with an unacceptable outcome - and they did so even in the patients whose repair never re-dislocated.
That last clause is the whole point, and it changes how the operation is judged. A shoulder that is quantified as a success because it has not dislocated again can still be a functional failure, so counting recurrences alone systematically flatters isolated Bankart repair in the subcritical range. It is why "the repair held" is not a sufficient answer for a young, high-demand patient with 15% bone loss, and why augmentation is discussed well below the classical critical figure.
Two caveats keep this honest. The cohort was 72 patients at a single military institution with a high level of mandatory physical activity, which is close to the worst case, so 13.5% is a warning line rather than a universal mandate - a sedentary, older, first-time dislocator with 15% loss is a different proposition from a 22-year-old infantry soldier or collision athlete. And the study was a Level III retrospective cohort, not a randomised comparison of repair against augmentation.
The Clinical Half of the Decision
Bone loss decides the operation only in combination with the patient, and the page's instruction to "integrate clinical risk" needs the actual instrument.
The Instability Severity Index Score (ISIS) is the scoring system to name, built from six preoperative variables scored out of 10:
- Criterion scoring
- 20 years or under
- Points
- 2
- Criterion scoring
- Competitive
- Points
- 2
- Criterion scoring
- Contact or forced overhead
- Points
- 1
- Criterion scoring
- Present on examination
- Points
- 1
- Criterion scoring
- Visible in external rotation
- Points
- 2
- Criterion scoring
- Loss of the normal contour
- Points
- 2
- Criterion scoring
- Above 6 = arthroscopic Bankart likely to fail
- Points
- 10
A score above 6 predicts an unacceptable recurrence rate after arthroscopic Bankart repair - of the order of 70% in the original series - and is the conventional trigger to offer an open or bony procedure instead. Note what the last two items imply: two of the ten points come from plain radiographs, which is a reminder that the score was designed as a rapid clinical screen, not as a substitute for the CT quantification described above. Use both - the score to flag the high-risk patient, the imaging to decide what the bone actually needs. The score is developed further in Bankart Lesions and Anterior Shoulder Instability.
The other clinical modifiers worth stating explicitly are a first dislocation before 20, a high number of prior dislocations, seizures (which drive very high recurrence and bilateral disease), generalised laxity on the Beighton score, and occupational demand - the soldier, the firefighter and the collision athlete all sit at the aggressive end of any threshold.
Computing On- vs Off-Track in Practice
- Glenoid track width = about 0.83 times the diameter of the intact inferior glenoid, minus the width of the anterior glenoid bone loss (so glenoid loss shrinks the track).
- Hill-Sachs interval (HSI) = the width of the Hill-Sachs lesion plus the "bone bridge" (the intact bone between the medial margin of the Hill-Sachs and the edge of the rotator-cuff footprint).
Then compare: if the Hill-Sachs interval is greater than the glenoid track width, the lesion is OFF-TRACK (it will engage the rim - high recurrence); if the interval is less than the track width, it is ON-TRACK. This is precisely what "the Hill-Sachs extends medial to the medial margin of the track" means. Critically, because glenoid bone loss is subtracted from the track width, more glenoid loss can flip an otherwise on-track Hill-Sachs to off-track - the bipolar interaction captured in a single calculation, and the reason both bones must be measured together. (The Hill-Sachs lesion itself is covered in Hill-Sachs Lesions, and the filling procedure in Remplissage.)
Compute on/off-track from two measured numbers: the Hill-Sachs interval (Hill-Sachs width plus bone bridge) versus the glenoid track width (about 0.83 times the intact glenoid diameter minus the glenoid bone-loss width). HSI greater than the track = OFF-TRACK (engages). Because glenoid loss shrinks the track, more glenoid loss can convert an on-track lesion to off-track.
Mnemonics & Memory Aids
TRACK
Hook:TRACK: Track width formula, Reconstruct on 3D CT, Assess both bones (bipolar), Critical 20-25%, Know procedure (Bankart/remplissage/Latarjet).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you assess bone loss in a patient with recurrent anterior shoulder instability?”
“How does bone-loss assessment change your surgical choice?”
Concept
- Bone loss is bipolar: anterior glenoid (bony Bankart) + posterosuperior humeral Hill-Sachs
- Assess both together (they interact)
- Under-estimating bone loss -> recurrence after isolated soft-tissue repair
Quantify glenoid loss
- En-face (sagittal-oblique) best-fit circle of the inferior glenoid
- 3D CT gold standard; 3D MRI validated alternative
- Subcritical ~13.5-20%; critical ~20-25%
Glenoid track
- Track width ~0.83 x glenoid diameter - glenoid bone-loss width
- Hill-Sachs medial to the track margin = OFF-TRACK (engages, high recurrence)
- Within track = ON-TRACK
Procedure selection
- On-track + minimal glenoid loss -> arthroscopic Bankart
- Off-track (subcritical glenoid loss) -> Bankart + remplissage
- Significant glenoid loss (~20%+ / subcritical + off-track / high-risk) -> Latarjet / bone block
Evidence & Key Studies
3D MRI vs 3D CT for static bone loss and dynamic bipolar (glenoid track) assessment in instability
- 3D CT has been the gold standard for evaluating static glenoid bone loss; 3D MRI was validated as a reliable alternative for both static bone loss and dynamic morphological variables.
- Measured variables included glenoid and humeral bone loss, Hill-Sachs occupancy, glenoid track zones and distance to dislocation; both modalities accurately identified on-track/off-track lesions.
- Inter- and intra-rater reliability was good to excellent, supporting either modality for preoperative bipolar bone-loss and glenoid-track assessment.
Bone-loss-guided treatment: dynamic anterior stabilization with remplissage for off-track/bipolar loss
- Soft-tissue stabilization (dynamic anterior stabilization using the biceps) is indicated for anterior instability with anterior glenoid bone loss of up to about 20%.
- In patients with bipolar bone loss who play contact/collision sports, augmenting with Hill-Sachs remplissage further increases stability and reduces recurrence.
- Treatment selection is explicitly driven by the amount of glenoid bone loss and whether the Hill-Sachs is engaging, supporting the bone-loss/glenoid-track framework.
Redefining critical bone loss in shoulder instability: functional outcomes worsen with subcritical bone loss
- 73 shoulders after isolated arthroscopic Bankart repair at a military institution, divided into quartiles by glenoid bone loss (means 2.8%, 10.4%, 16.1%, 24.5%) at a mean 48 months.
- Re-dislocation rose only in the top quartile - 7.3% below roughly 20% bone loss versus 27.8% above it - so the classical 20-25% figure is a RECURRENCE threshold.
- Function deteriorated far earlier: above 13.5% bone loss, WOSI scores fell to a level consistent with an unacceptable outcome EVEN IN PATIENTS WHO NEVER RE-DISLOCATED, with each rising quartile predicting a worse score.
3D CT being the gold standard for static glenoid bone loss (with 3D MRI a validated alternative) and the measurement of glenoid/humeral bone loss, Hill-Sachs occupancy and on/off-track glenoid track zones come from the cited Twomey-Kozak study; the bone-loss-driven treatment thresholds (soft-tissue repair up to ~20% glenoid loss, augmenting with remplissage for bipolar/off-track loss in contact athletes) from the cited de Campos Azevedo technical note. The bipolar-bone-loss concept, the en-face best-fit-circle quantification, the subcritical/critical thresholds, the glenoid-track formula and the Latarjet-for-significant- glenoid-loss principle are standard, well-established teaching, as are the ISIS components and cut-off, the plain-film views and the inverted-pear sign. The two-threshold rationale - recurrence rising above roughly 20% while function deteriorates from about 13.5% even without re-dislocation - comes from the cited Shaha cohort. (See also Anterior Shoulder Instability, Latarjet Procedure, Bankart Lesions, Hill-Sachs Lesions and Remplissage.)