A Milder FGFR3 Skeletal Dysplasia
- HYPOCHONDROPLASIA is a common AUTOSOMAL-DOMINANT skeletal dysplasia caused by a GAIN-OF-FUNCTION mutation in FGFR3 - the SAME gene mutated in achondroplasia, making the two allelic disorders - but it produces a generally MILDER phenotype; it is among the most common skeletal dysplasias and, unlike achondroplasia (often diagnosed prenatally or at birth), is predominantly diagnosed POSTNATALLY and may be UNDER-recognised in its milder forms.
- PUT NUMBERS ON 'COMMON' - AND NOTE IT IS THE LESS COMMON OF THE PAIR. In the French national rare-disease registry, live birth prevalence was 1.31 PER 100,000 for HYPOCHONDROPLASIA (range 0.54 to 2.08) against 3.27 PER 100,000 for ACHONDROPLASIA (1.90 to 4.03) - so hypochondroplasia is recorded about 2.5 TIMES LESS OFTEN, though the authors specifically note its prevalence is probably UNDERESTIMATED because mild forms go unrecognised. Diagnosis was POSTNATAL in 65.7 percent of hypochondroplasia, whereas achondroplasia was identified PRENATALLY in 40.8 percent and at BIRTH in a further 40.6 percent.
- THE INHERITANCE PATTERN DIFFERS FROM ACHONDROPLASIA AND THAT MATTERS FOR COUNSELLING. Only 57.2 PERCENT of hypochondroplasia cases were DE NOVO, against 85.5 percent of achondroplasia (p less than 0.0001) - so roughly FOUR IN TEN are INHERITED, and a family history of mild disproportionate short stature is far more likely to be informative here than in achondroplasia. Examine and ask about the parents.
- The PHENOTYPE is DISPROPORTIONATE SHORT STATURE with mild RHIZOMELIA (proximal-limb shortening), a stocky build, mild lumbar lordosis and sometimes mild genu varum, but with relatively NORMAL/subtle facial features - so it is much less obvious than achondroplasia and often presents simply as a short child whose proportions are mildly abnormal.
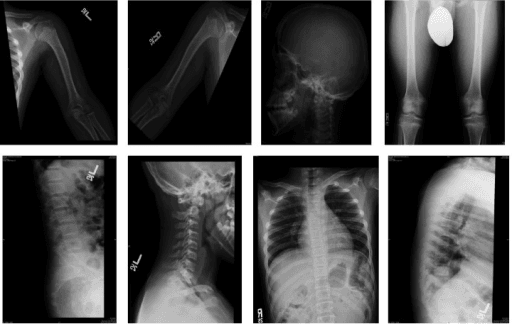
- A characteristic RADIOGRAPHIC clue is the FAILURE of the normal CAUDAL WIDENING of the lumbar INTERPEDICULAR DISTANCE (the distance between the pedicles should increase from L1 to L5; in hypochondroplasia/achondroplasia it fails to widen or narrows), together with a short, broad, squared pelvis and mildly short tubular bones - these point to an FGFR3 dysplasia.
- The DIFFERENTIAL is principally ACHONDROPLASIA (more severe, with frontal bossing, midface hypoplasia, prenatal/birth diagnosis and the important complication of FORAMEN MAGNUM stenosis), and also idiopathic short stature and SHOX-related short stature (Leri-Weill dyschondrosteosis/Turner-like features) - molecular FGFR3 testing confirms the diagnosis.
- ORTHOPAEDIC issues are generally milder than in achondroplasia but include disproportionate short stature, mild bowing (genu varum), lumbar lordosis and a degree of spinal stenosis risk; the SEVERE achondroplasia complications (marked spinal canal stenosis, foramen magnum stenosis) are less prominent but should be monitored where relevant.
- MANAGEMENT is largely SUPPORTIVE and SURVEILLANCE-based - monitoring growth, limb alignment (treating significant genu varum) and the spine - within a multidisciplinary skeletal-dysplasia service; with the emergence of FGFR3-PATHWAY (e.g. CNP-analogue) therapies for achondroplasia, similar targeted treatment for hypochondroplasia is anticipated, so timely diagnosis and access to specialist care matter.
- “Hypochondroplasia = autosomal-dominant FGFR3 gain-of-function dysplasia - the MILDER allelic relative of achondroplasia. Disproportionate short stature + mild rhizomelia; NORMAL/subtle face; often diagnosed POSTNATALLY.
- “Radiographic clue (shared with achondroplasia but milder): FAILURE of caudal widening of the lumbar INTERPEDICULAR distance; short squared pelvis.
- “Differential = achondroplasia (more severe, frontal bossing, foramen magnum stenosis) / idiopathic short stature / SHOX disorders. Management = surveillance (growth/alignment/spine); FGFR3-pathway therapy emerging.
- “Know the epidemiology: live birth prevalence 1.31 per 100,000 vs 3.27 for achondroplasia (French registry, probably an underestimate); diagnosed POSTNATALLY in 65.7% vs achondroplasia prenatally in 40.8% and at birth in 40.6%. De novo in only 57.2% vs 85.5% - so around 4 in 10 are INHERITED and the parents are worth examining.
Disproportionate short stature with mild rhizomelia and subtle/normal facies, diagnosed postnatally; radiograph shows failure of caudal lumbar interpedicular widening. FGFR3 mutation.
Achondroplasia (same gene, more severe) - frontal bossing, midface hypoplasia, foramen magnum stenosis, prenatal diagnosis. Also idiopathic short stature / SHOX disorders.
What It Is, Features & Differential
Hypochondroplasia is a common autosomal-dominant skeletal dysplasia from an FGFR3 gain-of-function mutation - the same gene as achondroplasia (an allelic disorder) - but milder. It causes disproportionate short stature with mild rhizomelia, a stocky build, mild lumbar lordosis and sometimes mild genu varum, with subtle/normal facial features, so it is often diagnosed postnatally and under-recognised. The characteristic radiographic clue is failure of the caudal widening of the lumbar interpedicular distance, with a short squared pelvis. The differential is achondroplasia (more severe, frontal bossing, foramen magnum stenosis, prenatal diagnosis), idiopathic short stature, and SHOX disorders; FGFR3 testing confirms it.
- Hypochondroplasia
- FGFR3 (gain-of-function)
- Achondroplasia
- FGFR3 (gain-of-function)
- Hypochondroplasia
- Milder
- Achondroplasia
- More severe
- Hypochondroplasia
- Normal/subtle
- Achondroplasia
- Frontal bossing, midface hypoplasia
- Hypochondroplasia
- Usually postnatal/childhood
- Achondroplasia
- Often prenatal/at birth
- Hypochondroplasia
- Less prominent
- Achondroplasia
- Important complication (infancy)
- Hypochondroplasia
- Fails to widen caudally (milder)
- Achondroplasia
- Fails to widen/narrows caudally
The Epidemiology, and What It Changes in Clinic
"Among the most common skeletal dysplasias" is true of the pair, but hypochondroplasia is the less common of the two. In the French national rare-disease registry, live birth prevalence was 1.31 per 100,000 for hypochondroplasia against 3.27 per 100,000 for achondroplasia - roughly 2.5 times less often recorded - although the authors are explicit that the hypochondroplasia figure is probably an underestimate, because mild phenotypes are never referred. The diagnostic timing splits just as sharply: achondroplasia was identified prenatally in 40.8 percent and at birth in a further 40.6 percent, while hypochondroplasia was diagnosed postnatally in 65.7 percent.
Achondroplasia is a de novo disease in 85.5 percent of cases. Hypochondroplasia is de novo in only 57.2 percent, so about four in ten are inherited from a parent who may themselves be undiagnosed and simply short. That makes the family history, and looking at the parents' proportions, genuinely useful here in a way it rarely is in achondroplasia - and it changes the recurrence-risk conversation.
These are registry data from one country, counting patients who reached a specialist service - so they measure diagnosed prevalence, not true prevalence, and the achondroplasia figure is explicitly France-specific because of the national rate of termination for medical reasons. One author is employed by the manufacturer of vosoritide, which is worth knowing when a paper argues for strengthened diagnostic pathways ahead of a targeted therapy.
Management
- Confirm the diagnosis: clinical/radiographic features + FGFR3 molecular testing.
- Surveillance: monitor growth, limb alignment (treat significant genu varum), and the spine (lordosis, stenosis risk) within a skeletal-dysplasia service.
- Orthopaedic intervention: for significant deformity (guided growth/osteotomy for bowing) or symptomatic spinal stenosis - generally less often than in achondroplasia.
- Take a family history and look at the parents: about 4 in 10 cases are inherited, unlike achondroplasia where 85.5 percent are de novo - the affected parent is often undiagnosed and simply short.
- Emerging therapy: FGFR3-pathway (CNP-analogue) treatments developed for achondroplasia are anticipated for hypochondroplasia - timely diagnosis and specialist access matter, though no trial has yet reported an outcome in hypochondroplasia.
The conditions on either side of this diagnosis have their own pages. The severe allelic disorder, with the foramen magnum stenosis that hypochondroplasia largely lacks, is achondroplasia, and the wider framework for classifying a short child is skeletal dysplasias. Where limb bowing or stature is treated surgically, the relevant principles are in limb lengthening and limb-length discrepancy and epiphysiodesis, and symptomatic canal narrowing follows lumbar spinal stenosis.
The two practical points in hypochondroplasia are recognition and correct classification. Because it is a milder FGFR3 dysplasia with subtle, often normal facial features, it is easily overlooked and is usually diagnosed postnatally - so a child with disproportionate short stature and mild rhizomelia, especially with the radiographic clue of failure of caudal widening of the lumbar interpedicular distance, should prompt consideration of an FGFR3 dysplasia and molecular confirmation rather than being labelled simply 'idiopathic short stature'. Equally, it should be distinguished from achondroplasia, which shares the gene but is more severe and carries the important infantile complication of foramen magnum stenosis; the milder hypochondroplasia phenotype generally lacks the severe canal/foramen problems, though spinal stenosis and limb bowing should still be monitored. Care is best delivered through a multidisciplinary skeletal-dysplasia service, and with FGFR3-pathway therapies emerging for achondroplasia, accurate and timely diagnosis is increasingly relevant for access to targeted treatment.
The FGFR3 Mutation and Why It Shortens the Bones
- The specific mutation. The commonest hypochondroplasia mutation is N540K (asparagine-to-lysine at codon 540, in the tyrosine-kinase-1 domain), found in about 60-70% of cases - a different codon and domain from achondroplasia's G380R (glycine-to-arginine at codon 380, in the transmembrane domain, which accounts for over 95% of achondroplasia). Rarer variants also occur, and about 30-40% of clinically-typical hypochondroplasia has no detectable FGFR3 mutation - so molecular testing can be negative and a clinical/radiographic diagnosis remains valid.
- Why the mutation shortens the bones. FGFR3 is a negative regulator of endochondral bone growth - it restrains chondrocyte proliferation and differentiation at the growth plate. A gain-of-function (constitutively active, ligand-independent) mutation drives excessive FGFR3 signalling (through the MAPK and STAT pathways), over-inhibiting the physeal chondrocytes and reducing long-bone growth.
- Severity tracks activation. The degree of receptor over-activation correlates with severity - milder N540K gives mild hypochondroplasia; G380R gives achondroplasia; the K650 mutations give the severe/lethal end.
Q: What is the FGFR3 mutation in hypochondroplasia, and how does it cause short stature?
A: The commonest is N540K (codon 540, tyrosine-kinase-1 domain) in ~60-70% - a different codon from achondroplasia's G380R (codon 380, transmembrane domain); about 30-40% of hypochondroplasia has no detectable FGFR3 mutation (so testing can be negative). FGFR3 is a negative regulator of growth-plate chondrocytes; a gain-of-function mutation drives constitutive FGFR3 signalling (MAPK/STAT) that over-inhibits chondrocyte proliferation → short bones. Severity tracks activation (N540K mild → G380R achondroplasia → K650 SADDAN/thanatophoric).
The FGFR3 Spectrum and the Emerging Therapy
- The FGFR3 spectrum (by severity). All are FGFR3 gain-of-function, with severity tracking the degree of receptor activation: hypochondroplasia (N540K, mildest) → achondroplasia (G380R) → SADDAN (Severe Achondroplasia with Developmental delay and Acanthosis Nigricans; K650M) → thanatophoric dysplasia (the lethal end; K650E and others).
- The emerging therapy - vosoritide. Vosoritide is a modified C-type natriuretic peptide (CNP) analogue. CNP binds natriuretic peptide receptor B (NPR-B) on growth-plate chondrocytes, raising cGMP, which inhibits the MAPK (RAF-MEK-ERK) arm downstream of FGFR3 - so it antagonises the FGFR3 over-signalling, restoring chondrocyte proliferation and endochondral growth. It is approved for achondroplasia (in children with open physes; a daily subcutaneous injection) and is being trialled in hypochondroplasia. The oral FGFR inhibitor infigratinib is also in trials.
Q: Where does hypochondroplasia sit in the FGFR3 spectrum, and what is the emerging therapy?
A: All are FGFR3 gain-of-function with severity tracking receptor activation: hypochondroplasia (N540K, mildest) → achondroplasia (G380R) → SADDAN (K650M, with developmental delay + acanthosis nigricans) → thanatophoric dysplasia (lethal; K650E). The emerging therapy is vosoritide, a CNP analogue that binds NPR-B → raises cGMP → inhibits the MAPK arm downstream of FGFR3, antagonising the over-signalling; approved for achondroplasia, being trialled in hypochondroplasia (the oral FGFR inhibitor infigratinib is also in trials).
Mnemonics & Memory Aids
FGFR3
Hook:FGFR3: FGFR3 gain-of-function, Growth (short/rhizomelic), Face subtle (postnatal), Radiographic lumbar clue, (milder) - surveillance.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has disproportionate short stature with mild proximal limb shortening but fairly normal facial features. What dysplasia would you consider, and how is it distinguished from achondroplasia?”
What it is
- Common autosomal-dominant skeletal dysplasia; FGFR3 gain-of-function
- Allelic with achondroplasia but milder; de novo in only 57 percent, so ~4 in 10 are inherited
- Live birth prevalence 1.31 per 100,000 (vs 3.27 for achondroplasia) - probably underestimated
- Diagnosed postnatally in 65.7 percent
Phenotype & radiograph
- Disproportionate short stature, mild rhizomelia, subtle/normal facies
- Mild lumbar lordosis +/- genu varum
- Failure of caudal lumbar interpedicular widening; short squared pelvis
Differential
- Achondroplasia (more severe, frontal bossing, foramen magnum stenosis)
- Idiopathic short stature; SHOX disorders (Leri-Weill/Turner features)
- Confirm with FGFR3 molecular testing
Management
- Surveillance: growth, limb alignment (genu varum), spine
- Multidisciplinary skeletal-dysplasia service
- FGFR3-pathway (CNP-analogue) therapy emerging
Evidence & Key Studies
Achondroplasia and hypochondroplasia - nationwide epidemiology (FGFR3 dysplasias)
- Retrospective analysis of the French National Registry of Rare Diseases: as of January 2024, 766 patients with achondroplasia and 408 with hypochondroplasia. Live birth prevalence, calculated from paediatric patients born 2008 to 2023, was 1.31 per 100,000 for hypochondroplasia (range 0.54 to 2.08) and 3.27 per 100,000 for achondroplasia (1.90 to 4.03).
- Achondroplasia was diagnosed prenatally in 40.8 percent and at birth in a further 40.6 percent, whereas hypochondroplasia was diagnosed postnatally in 65.7 percent (p less than 0.0001). Variants were de novo in 85.5 percent of achondroplasia but only 57.2 percent of hypochondroplasia (p less than 0.0001), so roughly four in ten hypochondroplasia cases are inherited.
- The authors state that hypochondroplasia prevalence is probably underestimated because milder forms go unrecognised, and that the achondroplasia figure is France-specific given the national rate of termination for medical reasons. The study is registry-based and one author is employed by the manufacturer of vosoritide.
The classification of hypochondroplasia as a common FGFR3 gain-of-function skeletal dysplasia (allelic with achondroplasia) causing disproportionate short stature, its predominantly postnatal diagnosis and under-recognition of milder forms, and the emergence of FGFR3-pathway therapy come from the cited Baujat epidemiological study. The specific clinical features (mild rhizomelia, subtle facies), the radiographic clue (failure of caudal lumbar interpedicular widening, squared pelvis), the differential from achondroplasia (foramen magnum stenosis) and SHOX disorders, and the surveillance-based orthopaedic management are standard, well- established teaching. The prevalence, de novo and diagnostic-timing proportions are from the French registry analysis, which measures diagnosed rather than true prevalence in a single country and whose achondroplasia figure the authors call France-specific. No trial has yet reported an outcome for vosoritide or infigratinib in hypochondroplasia; both are in trials, and the approval is for achondroplasia. There is likewise no hypochondroplasia-specific evidence for the timing of guided growth or osteotomy for genu varum, no validated spinal-surveillance interval, and no adult height data from a defined cohort - so none is quoted here.