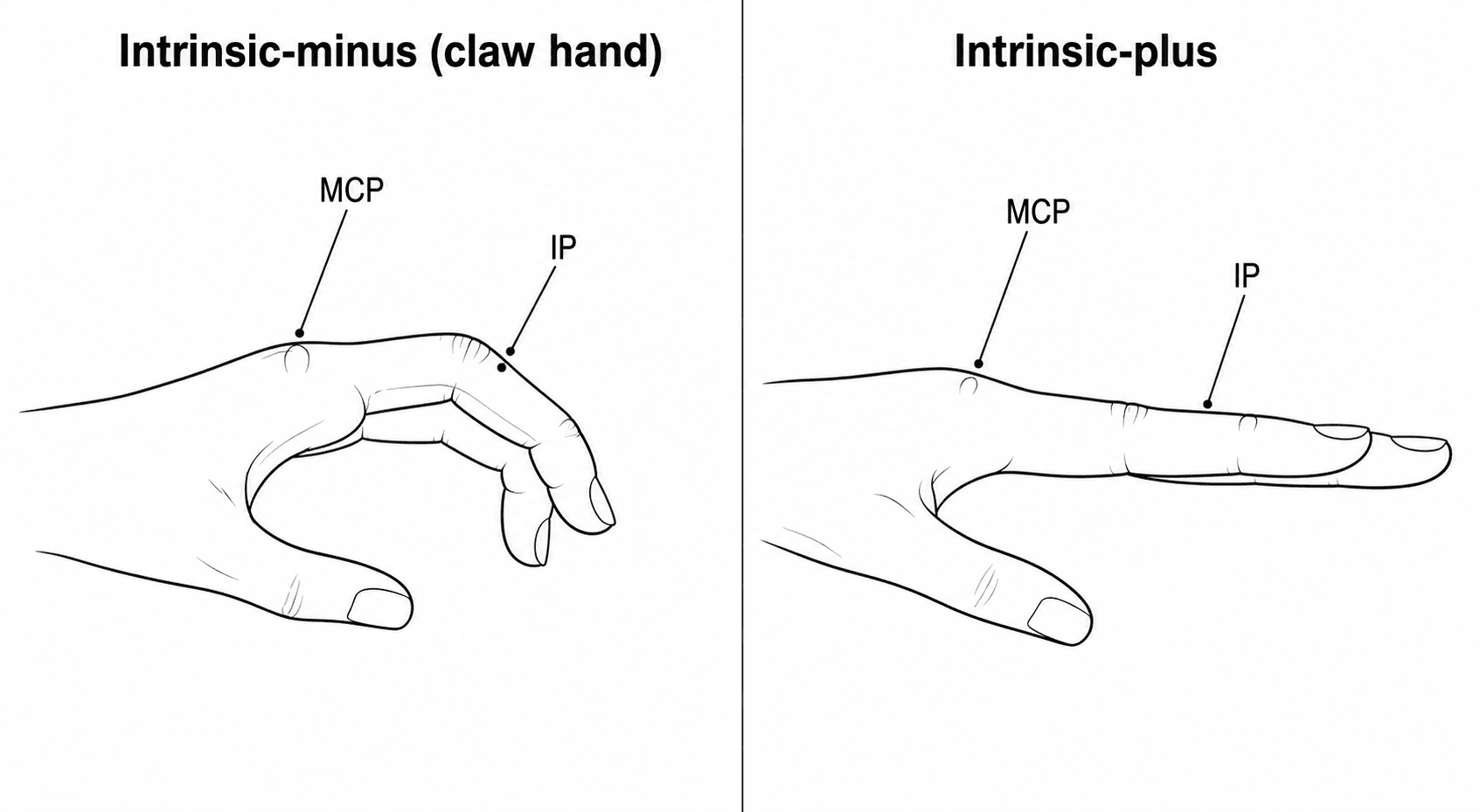
Intrinsic-Minus (Claw) vs Intrinsic-Plus - Two Opposite Deformities
- The intrinsic muscles of the hand (the INTEROSSEI and LUMBRICALS) act through the extensor expansion/lateral bands to FLEX the metacarpophalangeal (MCP) joints and EXTEND the interphalangeal (IP) joints; the lumbricals (origin FDP, insertion lateral band) are weak motors but spindle-rich and important for proprioception/precision pinch.
- INTRINSIC-MINUS (CLAW HAND): when the intrinsics are PARALYSED, MCP flexion and IP extension are lost, so the unopposed long extensors HYPEREXTEND the MCP joints and the unopposed long flexors FLEX the IP joints - the claw posture. The commonest causes are low ULNAR nerve palsy (claws the RING and LITTLE fingers), combined low ulnar+median palsy (claws all four fingers), and worldwide LEPROSY; also Charcot-Marie-Tooth and T1/lower brachial plexus lesions.
- The ULNAR PARADOX: a HIGH (proximal) ulnar nerve lesion produces LESS clawing than a LOW (distal) lesion, because a high lesion also paralyses the FDP to the ring and little fingers, so there is less IP flexion - paradoxically a worse (more proximal) lesion looks less clawed.
- The BOUVIER manoeuvre/test guides treatment of claw: if you passively BLOCK MCP HYPEREXTENSION (hold the MCP flexed) and the patient can then ACTIVELY EXTEND the IP joints, the extensor mechanism is intact (Bouvier-positive) and a STATIC MCP-blocking procedure (capsulodesis, or Zancolli LASSO) will correct the claw; if the IP joints still will not extend, a DYNAMIC transfer inserting into the extensor mechanism is needed.
- INTRINSIC-PLUS is the OPPOSITE deformity: intrinsic TIGHTNESS, CONTRACTURE or SPASTICITY makes the intrinsics overpull, FLEXING the MCP joints and EXTENDING the IP joints (often with thumb adduction). Causes include spasticity (stroke, cerebral palsy, head injury), ISCHAEMIC (Volkmann) contracture, trauma/scarring, rheumatoid disease, and prolonged immobilisation in the wrong position. The BUNNELL intrinsic tightness test detects it: PIP flexion is limited when the MCP is held EXTENDED (which tightens the intrinsics) but improves when the MCP is FLEXED.
- MANAGEMENT differs by deformity: for CLAW, prevent fixed contracture with anti-claw (lumbrical-bar) SPLINTING, correct any fixed PIP contracture, and for established claw use TENDON TRANSFERS (Zancolli lasso, FDS four-tail/Stiles-Bunnell, or Brand-type extensor transfers) to restore MCP flexion +/- IP extension; for INTRINSIC-PLUS, use stretching/splinting, treat spasticity (botulinum toxin), and perform a DISTAL INTRINSIC RELEASE for a fixed contracture.
- “Intrinsics FLEX MCP and EXTEND IP. Minus (paralysis) = claw (MCP hyperextended, IP flexed); Plus (tight/spastic) = MCP flexed, IP extended.
- “Ulnar paradox: HIGH ulnar lesion claws LESS than a LOW lesion (FDP to ring/little also out). Ulnar claw = ring + little fingers.
- “Bouvier test (block MCP hyperextension -> IP extend?) guides claw surgery; Bunnell test (PIP flexion worse with MCP extended) diagnoses intrinsic tightness.
Intrinsics paralysed -> MCP hyperextension + IP flexion. Think ulnar palsy/leprosy. Treat with splinting + tendon transfers.
Intrinsics tight/spastic -> MCP flexion + IP extension. Think spasticity/Volkmann. Treat with stretching, botulinum toxin, intrinsic release.
Intrinsic Muscle Function
The interossei (dorsal = abduct/DAB, palmar = adduct/PAD) and the lumbricals insert into the lateral bands/extensor expansion, giving them a unique action: they FLEX the MCP joints (they pass volar to the MCP axis) and EXTEND the IP joints (they pass dorsal to the IP axes). The lumbricals are unusual in arising from the FDP tendons and inserting on the radial lateral band, linking the flexor and extensor systems; they generate little force but are rich in muscle spindles and contribute to proprioception and precision pinch. Ulnar nerve supplies most intrinsics (all interossei, the ulnar two lumbricals, hypothenar and adductor pollicis); the median nerve supplies the radial two lumbricals and most thenar muscles. When the intrinsics fail, the MCP/IP balance is lost - and the direction of the resulting deformity depends on whether they are too WEAK (minus) or too TIGHT (plus).
Intrinsic-Minus (Claw Hand)
When the intrinsics are paralysed, the long extensors hyperextend the MCP joints and the long flexors flex the IP joints - the claw. A low ULNAR nerve palsy claws the ring and little fingers (the ulnar two lumbricals/interossei), while a combined low ulnar + median palsy claws all four fingers. The ULNAR PARADOX is high-yield: a HIGH ulnar lesion claws LESS than a LOW one, because a high lesion also paralyses the FDP to ring/little, reducing the IP flexion that produces the claw. Associated ulnar signs include Wartenberg's (abducted little finger), Froment's (FPL substitutes for a weak adductor pollicis on pinch) and Jeanne's signs. The commonest worldwide cause of intrinsic-minus claw is LEPROSY; other causes are Charcot-Marie-Tooth disease and T1/lower-trunk brachial plexus lesions.

The BOUVIER manoeuvre plans surgery: passively block MCP hyperextension (hold the MCP flexed) and ask the patient to extend the fingers. If the IP joints now extend (Bouvier-positive), the extensor mechanism is intact and a STATIC MCP-blocking procedure works - an MCP volar capsulodesis or the Zancolli LASSO (an FDS slip looped around the A1/A2 pulley to flex the MCP). If the IP joints still will not extend (Bouvier-negative), a DYNAMIC transfer that inserts into the lateral bands/extensor mechanism is required - e.g. the FDS four-tail (Stiles-Bunnell) or Brand transfers (ECRB/ECRL + tendon graft) to restore MCP flexion and IP extension. Always correct a fixed PIP flexion contracture first (splint/ release), and prevent contracture early with an anti-claw (lumbrical-bar) splint that holds the MCP flexed.
Intrinsic-Plus Hand
INTRINSIC-PLUS is the opposite of claw: the intrinsics are too tight (contracture) or spastic, so they overpull, FLEXING the MCP joints and EXTENDING the IP joints, often with the thumb adducted. Causes include spasticity (stroke, cerebral palsy, traumatic brain injury), ischaemic (Volkmann) contracture, trauma/scarring of the intrinsic compartments, rheumatoid disease, and prolonged immobilisation in the wrong position (which is exactly why the protective 'intrinsic-plus' position - MCP flexed, IP extended - is used to splint a hand, since it keeps the collateral ligaments at length). The BUNNELL intrinsic tightness test detects intrinsic tightness: hold the MCP in EXTENSION (which stretches the intrinsics) and try to flex the PIP - if PIP flexion is limited with the MCP extended but improves when the MCP is flexed (relaxing the intrinsics), the test is positive for intrinsic tightness. (If PIP flexion is instead worse with the wrist/MCP flexed, suspect extrinsic/extensor tightness.)
- First, exclude an acute cause. An intrinsic-plus posture that has appeared acutely in a swollen, tender hand is an acute compartment syndrome needing decompression, not any of the measures below.
- Non-fixed/spastic: stretching and splinting, and for spasticity, botulinum toxin (or systemic/ neurosurgical spasticity management) to reduce intrinsic overpull.
- Fixed contracture: a DISTAL INTRINSIC RELEASE - excising the oblique fibres (the medial portion of the lateral bands/extensor expansion) distal to the MCP - relieves the deforming intrinsic pull while preserving MCP flexion; more proximal releases or muscle slide are options in severe ischaemic contracture.
- Treat the underlying cause (e.g. established Volkmann's) and rehabilitate.
Why the Claw Becomes Fixed: Pathomechanics & Natural History
- Force re-routing at the MCP. With the intrinsics gone, the long extensor's force is no longer shared with the MCP flexors, so it concentrates on hyperextending the MCP. Once the MCP sits hyperextended, the long extensor is "used up" proximal to the IP joints and can no longer transmit effective extension distally, so the IP joints stay flexed under the unopposed long flexors.
- Secondary soft-tissue changes. A persistently hyperextended MCP attenuates the volar plate and contracts the dorsal structures, while a persistently flexed PIP contracts the volar plate, checkrein ligaments and skin and lets the lateral bands drift volar - so a deformity that began as a purely dynamic imbalance becomes a fixed contracture that no transfer alone can overcome.
- Why this dictates the sequence. This is why a fixed PIP flexion contracture must be released/splinted to supple before any claw-correcting transfer, and why early anti-claw (lumbrical-bar) splinting - which blocks MCP hyperextension and forces the long extensor to reach the IP joints - both relieves the posture and prevents the cycle from fixing.
- The over-correction trap. Once MCP hyperextension is blocked or a transfer restores intrinsic pull, the same lateral-band system can tip the other way into a swan-neck (PIP hyperextension) deformity, which is why over-tensioning is avoided and PIP hyperextension is guarded against - the mechanism is set out in swan-neck deformity.
The claw fixes because a hyperextended MCP "uses up" the long extensor before it reaches the IP joints, the volar plate stretches at the MCP and contracts at the PIP, and the lateral bands drift volar. Hence: make a fixed PIP supple first, splint early to break the cycle, and don't over-tension a transfer or you trade a claw for a swan-neck.
Which Clawed Hand Is This? Localising the Short Tissue
A clawed hand is a posture, not a diagnosis, and the three commonest causes are separated at the bedside without any imaging - by asking what happens when you move the wrist, and what happens when you move the MCP.
- What is short or absent
- Ulnar intrinsics paralysed - nothing is short
- The discriminating manoeuvre
- No change with wrist position; Bouvier manoeuvre corrects IP extension when the MCP is blocked
- Other clues
- Ring and little fingers only; ulnar-territory sensory loss; Froment, Jeanne and Wartenberg signs
- What is short or absent
- The extrinsic flexors (FDP, FPL first) are fibrosed and cross both wrist and fingers
- The discriminating manoeuvre
- POSITIVE TENODESIS (cascade) SIGN - extending the wrist worsens finger flexion, flexing the wrist lets the fingers open
- Other clues
- History of forearm compartment syndrome; all digits; graded by the Tsuge classification
- What is short or absent
- The interossei and lumbricals themselves are short
- The discriminating manoeuvre
- POSITIVE BUNNELL (Bunnell-Littler) TEST - PIP flexion limited with the MCP held EXTENDED, improving when the MCP is flexed; deformity unchanged by wrist position
- Other clues
- MCP flexed with IP extended; thumb adducted into the palm; spasticity, prior ischaemia or scarring
The logic is that a muscle crossing two joints betrays itself by joint position: an extrinsic flexor crosses the wrist, so wrist position changes the fingers; an intrinsic crosses the MCP but not the wrist, so the MCP changes the PIP while the wrist does nothing; and a paralysed muscle is not short at all, so neither manoeuvre tightens anything. The two can coexist after a severe forearm compartment syndrome, and finding one does not excuse looking for the other. The tenodesis-sign discriminator and the Tsuge grading are taken in substance from our Volkmann's ischaemic contracture topic.
The Acutely Intrinsic-Plus Hand Is a Different Problem
Everything written about stretching, splinting, botulinum toxin and intrinsic release applies to an established, chronic intrinsic-plus contracture. A hand that has adopted the intrinsic-plus posture acutely - after a crush, a high-pressure injection, extravasation, a burn, prolonged compression or a high-energy metacarpal fracture - is a different clinical problem: the intrinsic compartments are tense, the hand is painful between the metacarpals, and passive stretch of the intrinsics (extending the MCP while flexing the PIP) reproduces the pain. That is acute compartment syndrome of the hand, and the treatment is urgent decompression of the affected compartments - thenar, hypothenar, adductor and the interosseous spaces as required, with carpal tunnel or Guyon canal release depending on the injury and nerve findings - not stretching, not a splint, and not an intrinsic release. Normal pulses and normal capillary refill do not exclude it, because these are small compartments and the pressure that kills muscle is far below arterial pressure. Untreated, this is precisely how an ischaemic intrinsic contracture is created. The regional diagnostic and fasciotomy detail sits in our region-specific compartment syndrome topic.
Ask when the posture appeared. Chronic intrinsic-plus is stretched, splinted, injected or released. Acute intrinsic-plus in a swollen, tender hand is decompressed. The same posture, opposite operations - and the urgency belongs to the acute one alone, where the clock is muscle ischaemia rather than a contracture that has already happened.
The Thumb & the Eponymous Ulnar Signs
- What is lost. A low ulnar lesion paralyses the adductor pollicis, the deep head of flexor pollicis brevis and the first dorsal interosseous, so key pinch is weak and the index finger cannot be held abducted to stabilise pinch.
- Froment's sign. Asked to pinch a card, the patient flexes the thumb IP joint using FPL (median) to substitute for the weak adductor pollicis - a flexed thumb IP on pinch is Froment-positive.
- Jeanne's sign. The compensating long flexor pull, plus the lost adductor/FPB stabiliser, drives the thumb MCP into hyperextension during the same pinch - the MCP counterpart of Froment's.
- Wartenberg's sign. The little finger rests abducted because the ulnar-innervated third palmar interosseous (which adducts it) is out while the radially-innervated extensor digiti minimi is unopposed - the patient cannot adduct the little finger to the others.
- The intrinsic-plus thumb. In the tightness/spasticity (plus) hand the same adductor/intrinsic overpull drives a thumb-in-palm adduction posture that obstructs grasp.
- Reconstruction in principle. Beyond correcting the finger claw, restoring pinch may need an adductorplasty (a tendon transfer to recreate thumb adduction) and restoration of index abduction; the spastic thumb-in-palm needs tone management and selective release. The specific transfers are set out in tendon transfers for nerve palsy, and the broader ulnar work-up in ulnar nerve palsy and cubital tunnel syndrome.
The thumb tells the same story: lost adductor pollicis / first dorsal interosseous weaken key pinch, so FPL substitutes (Froment's), the thumb MCP hyperextends (Jeanne's), and the little finger sits abducted (Wartenberg's). In the intrinsic-plus hand the thumb is instead driven into thumb-in-palm adduction.
Mnemonics & Memory Aids
MINUS = claw
Hook:Intrinsic-MINUS = claw: MCP up, IP down.
PLUS
Hook:Intrinsic-PLUS = MCP flexed, IP extended (mirror of claw).
Frequently asked questions
What is an intrinsic-minus (claw) hand?
Intrinsic-minus hand is the claw deformity produced when the interossei and lumbricals are paralysed - classically by an ulnar nerve lesion (plus the median-innervated lumbricals in combined injuries). Without the intrinsics flexing the MCP joints and extending the IP joints through the extensor expansion, the unopposed long extensor hyperextends the MCP joints and the long flexors claw the fingers into IP flexion - most marked in the ring and little fingers.
What is the ulnar paradox?
A high (proximal) ulnar nerve lesion produces LESS clawing than a low (distal) lesion. A high lesion also paralyses the flexor digitorum profundus to the ring and little fingers, removing the flexor force that drives IP clawing; a low lesion spares FDP, so clawing is worse. Paradoxically, the more proximal and severe the lesion appears, the milder the visible deformity.
What is the Bouvier test and why does it matter?
In the Bouvier manoeuvre the examiner passively blocks MCP hyperextension and asks the patient to extend the IP joints. If full IP extension is then possible, the extensor digitorum communis can still extend the IPs once the MCPs are controlled - so splinting or a simple MCP-blocking procedure (or tendon transfer that prevents hyperextension) can restore extension. If IP extension is still impossible, the central slip/lateral band mechanism itself is deficient and needs reconstruction.
What is an intrinsic-plus hand?
Intrinsic-plus hand is the opposite deformity: the intrinsics are tight, contracted or spastic rather than paralysed, so they overpull through the extensor expansion and hold the fingers in MCP flexion with IP extension. It is tested with the Bunnell intrinsic tightness test - PIP flexion becomes harder when the MCP is held extended (stretching the tight intrinsics) than when the MCP is flexed - and occurs in rheumatoid arthritis, spasticity, compartment syndrome and post-traumatic contracture.
What is the safe position for splinting an injured hand?
The Edinburgh (intrinsic-plus) position: wrist extended about 30 degrees, MCP joints flexed 70-90 degrees, and the IP joints fully extended. With the MCPs flexed, the collateral ligaments are at maximal length, and with the IPs extended the lateral bands cannot shorten - so immobilisation in this position prevents the MCP extension and PIP flexion contractures that otherwise develop within weeks.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is a claw hand, what causes it, and what is the ulnar paradox?”
“How do the Bouvier and Bunnell tests help you, and how does management differ between a claw hand and an intrinsic-plus contracture?”
Intrinsic function
- Interossei + lumbricals: FLEX MCP, EXTEND IP (via lateral bands)
- DAB (dorsal abduct) / PAD (palmar adduct); lumbricals: FDP->lateral band (proprioception)
- Ulnar = most intrinsics; median = radial 2 lumbricals + thenar
Intrinsic-minus (claw)
- MCP hyperextension + IP flexion (intrinsic paralysis)
- Ulnar palsy (ring/little), combined (all four), leprosy, CMT, T1/plexus
- Ulnar paradox: HIGH lesion claws LESS; signs: Wartenberg, Froment, Jeanne
Intrinsic-plus
- MCP flexion + IP extension (intrinsic tightness/spasticity)
- Spasticity (stroke/CP/TBI), Volkmann, trauma, wrong-position immobilisation
- Bunnell (Bunnell-Littler) test: PIP flexion limited with MCP extended, improves with MCP flexed
- ACUTE intrinsic-plus in a swollen tender hand = compartment syndrome -> decompress, do not stretch
- Volkmann/extrinsic contracture instead changes with WRIST position (positive tenodesis/cascade sign)
Management
- Claw: anti-claw splint, correct PIP contracture; Bouvier+ -> capsulodesis/Zancolli lasso; Bouvier- -> FDS-4-tail/Brand
- Intrinsic-plus: stretch/splint, botulinum toxin (spastic), distal intrinsic release (fixed)
- Treat the underlying cause; prevent fixed contractures early
Evidence & Key Studies
A biomechanical and evolutionary perspective on the function of the lumbrical muscle
- The lumbricals originate from the FDP tendons and insert onto the lateral band of the extensor mechanism, linking the flexor and extensor systems.
- They have the smallest physiological cross-sectional area in the upper limb (about one-tenth the motor force of the interossei) but are rich in muscle spindles, contributing to proprioception of the finger joints.
- The radial two lumbricals (median-innervated) appear functionally more important for precision pinch - relevant to the radial sparing seen in ulnar claw.
Surgical reconstruction of irreversible ulnar nerve paralysis in leprosy
- In 25 patients with irreversible ulnar claw, the FDS four-tail (Stiles-Bunnell) and Zancolli lasso procedures were compared.
- The FDS four-tail was more effective at CORRECTING the claw deformity, whereas the Zancolli lasso better restored GRIP STRENGTH.
- Pre-operative PIP extensor lag and longer paralysis time predicted worse outcomes, and swan-neck deformity could develop - reinforcing early treatment and contracture prevention.
The lumbrical origin/insertion, weak-but-proprioceptive role and the functional importance of the radial two lumbricals come from the cited Wang study, and the comparison of FDS four-tail versus Zancolli lasso for ulnar claw (and the prognostic effect of PIP extensor lag/paralysis duration) from the cited Ozkan study - a comparison of 25 patients, so the finding that the four-tail corrects the deformity better while the lasso restores more grip should be quoted as a small single-series signal rather than a settled result. The intrinsic action (flex MCP/extend IP), the ulnar paradox and the Bouvier/Bunnell tests are standard, well-established hand teaching. Leprosy is widely taught as the commonest cause of claw hand worldwide and is stated here on that basis; a PubMed search did not return a study giving a proportion or denominator for that claim, so no figure is quoted. The tenodesis (cascade) discriminator, the Bunnell-Littler naming and the Tsuge grading are taken in substance from our Volkmann's ischaemic contracture topic, and the hand-compartment decompression detail from region-specific compartment syndrome. See also ulnar nerve palsy, cubital tunnel syndrome, tendon transfers for nerve palsy and swan-neck deformity.