Congenital Limb Deficiency & Acquired Amputation in Children
- The central principle is that CHILDREN ARE NOT SMALL ADULTS: the GROWING skeleton, open physes, remarkable functional ADAPTATION, and the unique stump behaviour of children mean that adult amputation principles cannot simply be transferred - paediatric amputee care has its own rules. Adaptation is not the same as prosthetic acceptance: UPPER-limb prosthesis rejection is common (most of all in unilateral congenital below-elbow deficiency, where the SENSATE residual limb is often the better tool), while LOWER-limb prostheses are seldom rejected because nothing substitutes for a limb to stand on.
- Where feasible, DISARTICULATION (amputation THROUGH a JOINT) is PREFERRED over a TRANSOSSEOUS (through-bone) amputation in the growing child, because it PRESERVES the distal PHYSIS (maintaining limb length and growth), produces a robust END-BEARING stump, and crucially AVOIDS TERMINAL BONY OVERGROWTH, which affects cut bone ends but not disarticulations - and as much length and as many growth plates as possible should be preserved.
- TERMINAL BONY OVERGROWTH is the COMMONEST complication of a paediatric transosseous (through-bone) stump: appositional new bone forms at the cut end (most often the humerus, fibula, tibia and femur), creating a sharp bony spike that tents or penetrates the skin, causes pain and bursae, and requires surgical REVISION (stump revision/resection, and capping techniques) - often more than once during growth.
- CONGENITAL limb deficiencies are uncommon birth defects that may go undetected on prenatal ultrasound until birth; a child with a congenital limb difference should have a DIAGNOSTIC EVALUATION to rule out SYNDROMES involving other organ systems or known associations - so the work-up looks beyond the limb.
- ACQUIRED paediatric amputation is most commonly due to TRAUMA (the leading cause), with tumour (limb-salvage versus amputation/rotationplasty), and infection/sepsis (e.g. meningococcal purpura fulminans) as other causes; the principles of preserving length, growth plates and joints, and favouring disarticulation, still apply.
- MANAGEMENT is MULTIDISCIPLINARY and FAMILY-CENTRED: prosthetic fitting is timed to DEVELOPMENTAL MILESTONES (e.g. a lower-limb prosthesis around the time of pulling-to-stand/walking, an upper-limb prosthesis around sitting/bimanual development), with prostheses upsized/replaced as the child grows; ongoing management addresses overgrowth, phantom sensation (less troublesome and less often painful than in adults, especially in congenital cases), psychosocial support and the family's goals - and a multidisciplinary, family-centred approach leads to a successful, functional and fulfilling life.
- “Children are NOT small adults: growing skeleton, terminal bony overgrowth, excellent adaptation. Preserve length + growth plates + joints. But adaptation is not acceptance - UPPER-limb prostheses are often rejected (sensate residual limb wins), LOWER-limb ones rarely.
- “Prefer DISARTICULATION over transosseous amputation - preserves the physis, gives an end-bearing stump, and AVOIDS terminal bony overgrowth (the commonest paediatric stump complication; needs revision, often repeatedly).
- “Congenital limb difference -> evaluate for a SYNDROME/associations; acquired -> usually TRAUMA. Multidisciplinary, family-centred care; fit prostheses at developmental milestones.
In the growing child, disarticulation (through a joint) beats transosseous amputation - it preserves the physis (length/growth), is end-bearing, and avoids terminal bony overgrowth.
The commonest paediatric transosseous-stump complication - a painful bony spike that tents/penetrates the skin (humerus, fibula, tibia, femur) - needing revision, often repeatedly during growth.
How Children Differ
Paediatric amputee care differs fundamentally from the adult: the growing skeleton and open physes drive length and growth, children adapt remarkably, and their stumps behave differently. The two consequences that dominate practice are (1) the preference for disarticulation over a transosseous amputation - to preserve the distal physis (length/growth), give an end-bearing stump, and avoid terminal bony overgrowth; and (2) terminal bony overgrowth itself, the commonest complication of a through-bone stump, where appositional bone at the cut end forms a painful spike that needs revision. The general rule is to preserve length, growth plates and joints.
Why Children Adapt - and Phantom Limb in the Child
Children adapt remarkably, integrate a prosthesis they do use far more readily than an adult, and have phantom sensation that is less troublesome and often absent in congenital cases. The reason for all three is the plasticity of the developing brain and how the cortical body schema forms.
The child's brain has far greater cortical plasticity, so a child integrates a prosthesis into the body schema and learns one-handed/compensatory strategies much more readily than an adult. This is the rationale for early, milestone-timed prosthetic introduction - it exploits the developmental window.
In congenital deficiency the missing limb was never represented in the cortical body schema, so phantom sensation is usually absent or minimal. In acquired amputation a phantom can occur but is generally less frequent and less troublesome than in adults and tends to diminish with growth; severe phantom pain is uncommon, so management is mainly reassurance and symptomatic (formal neuroma strategies such as TMR/RPNI are a separate topic).
Congenital absence -> no established body schema -> little or no phantom; the developing brain's plasticity is why children adapt so well and why early, milestone-based prosthetic fitting works. Phantom pain severe enough to need adult-style intervention is the exception, not the rule.
Congenital vs Acquired, and Evaluation
- Congenital limb deficiency
- Developmental (often syndromic/associated anomalies)
- Acquired amputation
- Most commonly trauma (also tumour, infection/sepsis)
- Congenital limb deficiency
- Evaluate for syndromes/other organ systems
- Acquired amputation
- Manage the injury/disease; preserve length/joints
- Congenital limb deficiency
- Lower (no cut bone end if not operated)
- Acquired amputation
- Higher with transosseous stumps
- Congenital limb deficiency
- Often absent/less troublesome (congenital)
- Acquired amputation
- More common but usually less than adults
- Congenital limb deficiency
- Reconstruction vs prosthetic pathway, family goals
- Acquired amputation
- Disarticulation preferred; prosthetic rehabilitation
For a congenital limb difference, perform a diagnostic evaluation for associated syndromes and other organ systems - the limb is not always the whole story. For an acquired amputation (most often trauma), apply the paediatric principles: preserve length, growth plates and joints, and favour disarticulation. Across both, plan the prosthetic pathway with the family.
Naming the Deficiency, and the Conditions Behind the Decision
Use the ISO/ISPO terminology, not the classical names. Congenital limb deficiencies are described as transverse or longitudinal:
- A transverse deficiency is an amputation-like absence of everything distal to a level, with the limb developed normally down to that point - the commonest is a transverse forearm deficiency.
- A longitudinal deficiency is absence of a specific bone or ray along the limb axis, with structures distal to it often partly present - fibular, tibial and femoral deficiencies are the examples that reach the orthopaedic clinic.
The classical terms - amelia, hemimelia, phocomelia - are imprecise about exactly what is missing and are largely abandoned in formal description, though they persist in conversation and in older literature. Being able to say "longitudinal fibular deficiency" rather than "fibular hemimelia" signals current practice, and more importantly it forces the description to specify which bone and how much of it.
The amputation-versus-reconstruction decisions live in the individual conditions, each of which turns on different anatomy - whether a plantigrade foot can be preserved, how much length will ultimately be missing, whether the knee is stable, whether there is a quadriceps mechanism:
- Fibular Hemimelia - the commonest longitudinal deficiency, and the classic choice between Syme or Boyd amputation and staged reconstruction with lengthening. Boyd retains the calcaneus and its heel pad, which resists the pad migration that can trouble a Syme.
- Tibial Hemimelia - where the presence or absence of a functioning quadriceps and proximal tibia dominates the decision.
- Proximal Femoral Focal Deficiency and Rotationplasty - where the ankle can be turned to serve as a knee.
- Congenital Lower Limb Deficiency Overview for the shared framework, and Limb Lengthening Principles and Limb-Length Discrepancy and Epiphysiodesis for the reconstruction side of the same conversation.
- Lower Limb Amputation Levels and Foot and Ankle Amputation Levels for the levels themselves.
Management & Prosthetic Pathway
- Multidisciplinary, family-centred care (orthopaedics, rehabilitation/physiatry, prosthetist, physiotherapy, psychology) built around the child's and family's goals.
- Prosthetic timing to developmental milestones: lower-limb prosthesis around pulling-to-stand/walking; upper-limb prosthesis around sitting/bimanual development - upsized/replaced as the child grows.
- Manage terminal bony overgrowth: stump revision/resection and capping when the bony spike causes pain/skin problems - often required more than once during growth.
- Phantom sensation/pain: generally less troublesome than in adults (often absent in congenital cases) - reassure and manage symptomatically.
- Ongoing: psychosocial support, periodic review through growth, and revisiting reconstruction-versus-prosthetic decisions as the child develops.
"Timed to developmental milestones" means specific milestones at specific ages. The principle is that a prosthesis is introduced when the child is developmentally ready to use it for the task it exists to perform - fitted earlier it is a burden the child discards, fitted later it is an intrusion into a body schema that has already been built without it.
- Approximate age
- Around 6 months
- What is fitted, and why then
- First UPPER-limb prosthesis - a passive mitt. It is not there to grip; it restores a surface for two-handed activity and gets the limb accepted as part of the body while the schema is forming
- Approximate age
- Around 9 to 12 months
- What is fitted, and why then
- First LOWER-limb prosthesis, matching the age at which an unaffected child would be weight-bearing. Standing is the trigger, not walking - the child needs the limb to learn to walk with, not after
- Approximate age
- Around 18 to 24 months
- What is fitted, and why then
- Active terminal device (body-powered hook or hand). Fitting an active device before the child can operate it teaches rejection
- Approximate age
- Throughout childhood
- What is fitted, and why then
- Sockets are outgrown well before the components are; expect regular re-socketing and replacement through growth, more frequently in the youngest and around growth spurts
- Approximate age
- School age onward
- What is fitted, and why then
- Activity-specific devices and the cosmetic considerations that begin to matter to the child rather than the parents
Adaptation and prosthetic tolerance are not the same thing, and conflating them leads to pushing hardware onto a child who does not need it.
Rejection is common in the upper limb, most of all in the child with a unilateral congenital below-elbow deficiency - the very group whose prosthesis is most often prescribed. The reason is straightforward once stated: the residual limb is sensate, and a short forearm with sensation is a better tool for many tasks than an insensate device that must be consciously operated. These children frequently achieve excellent bimanual function without a prosthesis, and often abandon one that has been fitted.
Lower-limb prostheses are a different matter and are seldom rejected, because there is no unaided alternative for weight-bearing - the child cannot substitute sensation for a limb to stand on.
What follows for practice. Offer the upper-limb prosthesis, fit it at the right milestone, and train its use - but treat non-use as information rather than failure, and ask what the child is actually trying to do. A child who is thriving one-handed does not need to be persuaded. The wrong conversation is one that frames the prosthesis as necessary for normality, which is a message about the child rather than about function.
A specific rate is not quoted here because the published figures vary widely with device type, deficiency level and era; the clinically useful point is the direction and the reason for it.
The two enduring lessons in paediatric amputee surgery follow from the growing skeleton. First, preserve length, growth plates and joints, and favour disarticulation over a transosseous amputation wherever feasible: a disarticulation keeps the distal physis (so the residual limb grows with the child and length is maximised), gives an end-bearing stump, and - critically - does not develop terminal bony overgrowth. Second, anticipate terminal bony overgrowth as the commonest complication of any through-bone stump in a child: appositional bone at the cut end forms a painful spike that tents or perforates the skin, and it typically requires surgical revision, often repeatedly as the child grows, so families should be counselled to expect this. Around these surgical principles, the care is multidisciplinary and family-centred, with prosthetic fitting timed to developmental milestones and upsized through growth, and - for congenital limb differences - a work-up for associated syndromes, because the limb may be one feature of a wider condition.
Terminal Bony Overgrowth: Mechanism and the Capping Solutions
Terminal bony overgrowth is the commonest paediatric stump complication needing revision. Its mechanism and its specific solution are worth taking together, because they explain both why a disarticulation avoids it and why simple resection alone fails.
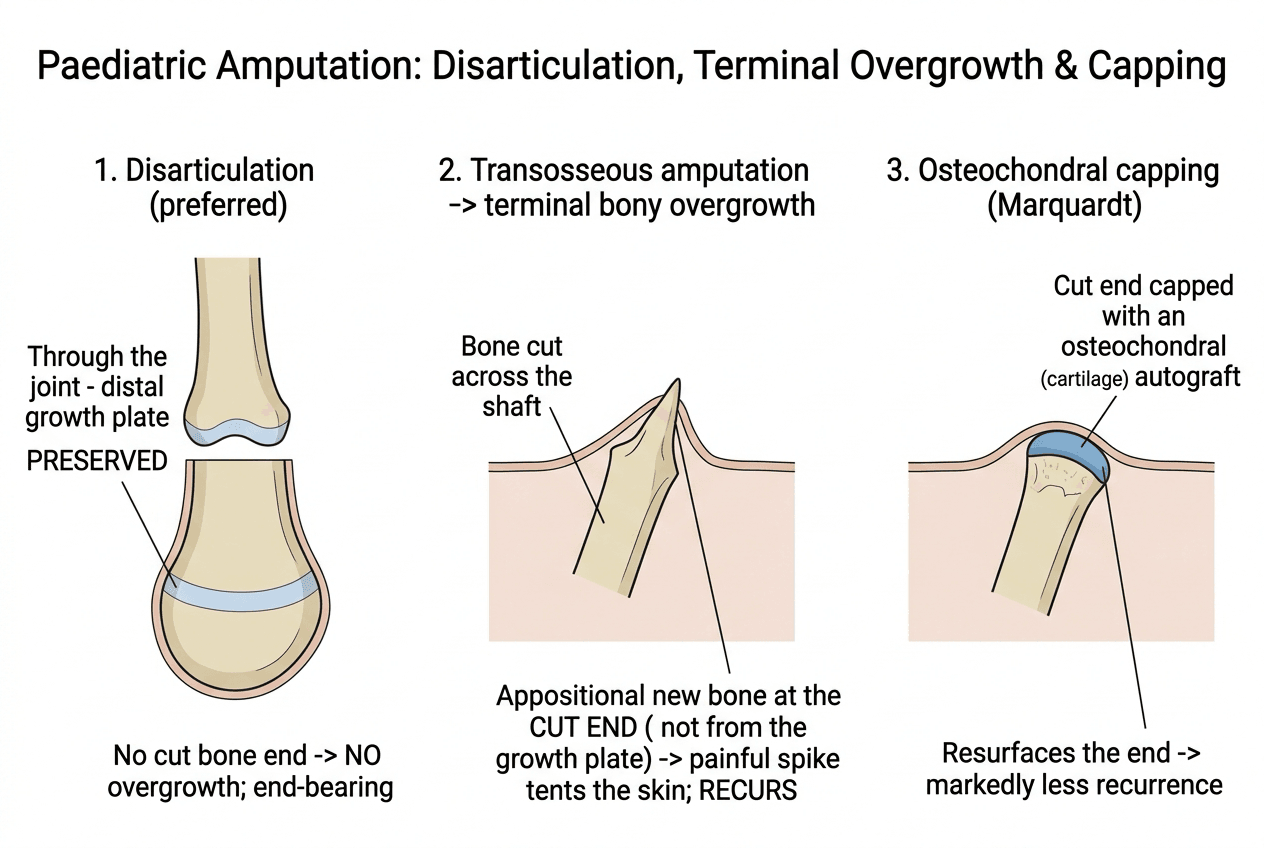
Overgrowth is appositional new bone at the cut diaphyseal end (oblique terminal/periosteal new-bone formation) - it is NOT driven by the proximal growth plate. So it occurs at the transected end of a long bone and keeps recurring through growth even when the distal physis has been removed, which is precisely why a disarticulation (no cut bone end) does not overgrow. Commonest bones, in order: humerus, then fibula, tibia, femur.
Simple stump resection alone has a high recurrence. The durable solution is to cap the cut end - classically an autologous osteochondral cap (the Marquardt technique, using a cartilage-bearing autograft such as resected epiphysis or iliac apophysis) or a synthetic cap - which resurfaces the bone end and markedly reduces recurrence. Counsel families that revision may be needed more than once until skeletal maturity.
Terminal bony overgrowth is appositional (cut-end) bone, not physeal - so it recurs after plain resection. The durable fix is autologous osteochondral capping (Marquardt); the best fix of all is to avoid a cut bone end by choosing disarticulation.
Mnemonics & Memory Aids
GROW
Hook:GROW: Growing skeleton, Reserve disarticulation, Overgrowth (terminal bony), Whole child/family-centred.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How does amputation in a child differ from an adult, and why do you prefer disarticulation?”
How children differ
- Growing skeleton/open physes; excellent adaptation - but upper-limb prostheses are often rejected, lower-limb rarely
- Preserve length, growth plates and joints
- Phantom sensation usually less than adults (often absent in congenital)
Surgical principles
- Prefer disarticulation over transosseous amputation (preserve physis, end-bearing, avoid overgrowth)
- Terminal bony overgrowth = commonest through-bone stump complication
- Overgrowth needs revision (resection/capping), often repeatedly during growth
Congenital vs acquired
- Congenital limb difference: evaluate for syndromes/associations
- Acquired: most commonly trauma (also tumour, infection/sepsis)
- Plan reconstruction vs prosthetic pathway with the family
Management
- Multidisciplinary, family-centred care
- Prosthetic fitting timed to developmental milestones; upsize through growth
- Psychosocial support; periodic review; revisit decisions as the child develops
Evidence & Key Studies
Pediatric limb differences and amputations
- Congenital limb differences are uncommon birth defects that may go undetected even on prenatal ultrasound and often are not detected until birth; affected children should have a diagnostic evaluation to rule out syndromes involving other organ systems or known associations.
- The most common aetiology of acquired amputation is trauma; post-amputation complications include pain and terminal bony overgrowth.
- A multidisciplinary approach to management with the child and family can lead to a successful, functional and fulfilling life.
The need to evaluate a child with a congenital limb difference for associated syndromes, the fact that trauma is the commonest cause of acquired paediatric amputation, terminal bony overgrowth as a key complication, and the value of a multidisciplinary, family-centred approach come from the cited Le and Scott-Wyard review. The preference for disarticulation over transosseous amputation (to preserve the physis, achieve end-bearing and avoid overgrowth), the principle of preserving length/growth plates/joints, and prosthetic timing to developmental milestones are standard, well-established teaching, as is the ISO/ISPO transverse-versus- longitudinal terminology. The milestone ages given are the normal developmental ages at which sitting balance, pulling to stand and purposeful two-stage actions appear, applied to prosthetic prescription as the cited sources direct. No prosthetic rejection rate is quoted, because published figures vary widely with device type, level of deficiency and era - the direction of the finding and the reason for it are what matter clinically. (See also Congenital Lower Limb Deficiency Overview, Fibular Hemimelia, Rotationplasty and Lower Limb Amputation Levels.)