Axillary Nerve + PCHA Compression | Overhead Athlete | Neurogenic vs Vascular | Diagnosis of Exclusion
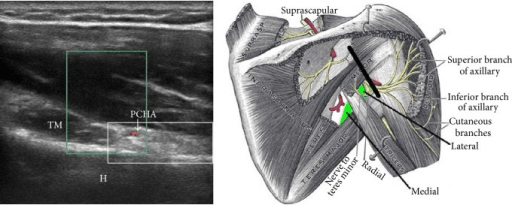
- Quadrilateral space contents - axillary nerve and posterior circumflex humeral artery (PCHA)
- Overhead athletes (throwers, volleyball, swimmers) are the classic group
- Diagnosis of exclusion - no single gold-standard test; rule out cuff, suprascapular nerve, cervical radiculopathy
- Isolated teres minor atrophy on MRI is sensitive but poorly specific for compressive QSS
- Non-operative for at least 6 months before considering surgical decompression
- “Symptoms reproduced by sustained abduction-external rotation for about 1 minute
- “Point tenderness over the quadrilateral space, lateral to the scapula
- “Image-guided quadrilateral space block giving pain relief supports the diagnosis
- “Vascular subtype can present as digital ischaemia in a young dominant-arm athlete
There is no gold-standard test. Rotator cuff disease, suprascapular neuropathy, and cervical radiculopathy are far more common - exclude them first before invoking QSS.
Isolated teres minor atrophy on MRI is sensitive but NOT specific. It is more often due to cuff tears or idiopathic traction than to true compressive QSS.
Separate neurogenic (axillary nerve) from vascular (PCHA thrombosis, aneurysm, distal emboli). Vascular QSS can be a limb-threatening emergency.
Symptoms are reproduced by sustained abduction and external rotation (the throwing/cocking position) and by point pressure over the quadrilateral space.
Overview and Epidemiology
Quadrilateral space syndrome (QSS), also written quadrangular space syndrome, is a relatively rare condition in which the axillary nerve and the posterior circumflex humeral artery (PCHA) are compressed as they pass through the quadrilateral space of the posterior shoulder. The result is a constellation of poorly localised symptoms - posterolateral shoulder pain, paraesthesia in a non-dermatomal pattern, and sometimes deltoid or teres minor weakness - that overlap with much more common shoulder problems.
The condition was first described in the early 1980s and remains uncommon, which is exactly why it is a high-yield exam trap: it is the diagnosis you reach only after excluding rotator cuff disease, suprascapular neuropathy, and cervical radiculopathy.
QSS classically affects young adults (roughly 20 to 40 years) who perform repetitive overhead arm movements - baseball pitchers, volleyball and tennis players, swimmers, and throwers. The dominant arm is usually involved. Fibrous bands are the most commonly implicated cause; true space-occupying lesions (paralabral cysts, osteochondroma, tumour, aneurysm) are less common but important to find.
Key epidemiological points:
- True compressive QSS is rare; large MRI series show that isolated teres minor atrophy is far more often explained by cuff disease or idiopathic traction than by genuine compression.
- The neurogenic subtype is the more common presentation; the vascular subtype is rarer but can be limb-threatening.
- Because the syndrome is uncommon and the symptoms are vague, diagnostic delay is the rule, and many patients are treated for presumed cuff or cervical pathology first.
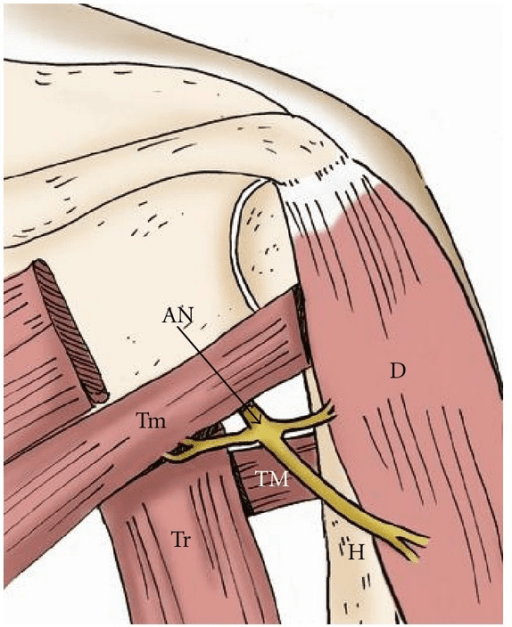
Pathophysiology and Anatomy
The quadrilateral space is a four-sided gap in the posterior shoulder bounded by:
- Superior: teres minor
- Inferior: teres major
- Medial: long head of triceps brachii
- Lateral: surgical neck of the humerus
Its two contents - the axillary nerve and the posterior circumflex humeral artery - are the structures at risk in QSS.
- Structure
- Teres minor
- Relevance
- Innervated by axillary nerve - atrophies in QSS
- Structure
- Teres major
- Relevance
- Lower border of the space
- Structure
- Long head of triceps
- Relevance
- Common site of compressive fibrous bands
- Structure
- Surgical neck of humerus
- Relevance
- Bony lateral wall
- Structure
- Axillary nerve
- Relevance
- Neurogenic QSS - deltoid + teres minor
- Structure
- Posterior circumflex humeral artery
- Relevance
- Vascular QSS - thrombosis, aneurysm, emboli
Why compression happens. The space is dynamic. During abduction and external rotation - the throwing cocking position - the borders crowd together and the cross-sectional area of the quadrilateral space falls. In repetitive overhead athletes, hypertrophy of the surrounding muscles and the development of fibrous bands (most often between the teres muscles and the long head of triceps) narrow the space further and tether the neurovascular bundle.
Neurogenic pathophysiology. Chronic compression or traction of the axillary nerve produces a focal neuropathy. Because the teres minor branch is often involved, isolated teres minor denervation and fatty atrophy is the classic (though non-specific) imaging hallmark. More severe compression of the main axillary nerve also denervates the deltoid.
Vascular pathophysiology. Repetitive compression of the PCHA against fibrous bands or the humerus causes intimal injury, which can lead to thrombosis, aneurysm formation, and distal embolisation. The clinical result may be digital ischaemia, splinter haemorrhages, or cold intolerance in the dominant hand of a young athlete - a presentation that is easy to miss if QSS is not considered.
Paralabral Cyst QSS: The Space-Occupying Cause You Must Not Miss
The classification and surgical sections repeatedly flag a paralabral cyst and warn that decompressing it alone "risks recurrence" — this space-occupying cause deserves developing, because it changes the operation.
- The mechanism. A posteroinferior labral tear acts as a one-way valve: joint fluid is pumped out through the tear and loculates into a paralabral (ganglion) cyst that tracks posteroinferiorly into the quadrilateral space, where it compresses the axillary nerve. It is the direct analogue of the spinoglenoid-notch cyst that compresses the suprascapular nerve.
- Why it matters clinically. Unlike fibrous-band QSS, this is a structural lesion with a treatable source, and MRI shows both the cyst in the quadrilateral space and the underlying labral tear — so it is one of the QSS presentations where surgery is clearly indicated rather than a six-month rehabilitation problem.
- The key surgical principle. Decompressing the cyst alone risks recurrence — the labral tear keeps refilling it. Definitive treatment addresses the labral tear (arthroscopic labral repair to close the one-way valve), with or without cyst decompression. This is exactly why this topic warns against isolated cyst decompression.
- Contrast to remember. Suprascapular nerve at the spinoglenoid notch is compressed by a cyst from a superior (SLAP-type) labral tear; the axillary nerve in the quadrilateral space is compressed by a cyst from a posteroinferior labral tear — same one-way-valve principle, different nerve and tear location.
Q: MRI shows a paralabral cyst in the quadrilateral space compressing the axillary nerve — why is simply decompressing the cyst the wrong operation? A: The cyst arises from a posteroinferior labral tear acting as a one-way valve (the axillary-nerve analogue of the spinoglenoid cyst/SLAP tear compressing the suprascapular nerve). Aspirating or decompressing the cyst alone leaves the tear to refill it and recur — the definitive treatment is to repair the labral tear (with or without cyst decompression).
Classification
QSS is most usefully classified by the predominant compressed structure, because this drives both the presentation and the management.
Neurogenic QSS (axillary nerve compression)
- More common subtype
- Symptoms: vague posterolateral shoulder and lateral arm pain, paraesthesia in a non-dermatomal pattern, fatigue and weakness with overhead activity
- Signs: point tenderness over the quadrilateral space; symptoms reproduced by sustained abduction-external rotation; teres minor +/- deltoid atrophy in chronic cases
- Workup driver: MRI for teres minor / deltoid denervation; EMG/NCS; diagnostic block
- Management driver: non-operative rehab first; decompression (release of fibrous bands +/- neurolysis) if refractory
Clinical Assessment
History. Ask about the sport and the dominant arm. The typical patient is a young overhead athlete with insidious, poorly localised posterolateral shoulder pain that is worse with the arm abducted and externally rotated, and who may describe paraesthesia down the lateral arm that does not follow a dermatome. In the vascular subtype, ask specifically about cold hands, colour change, and finger pain.
Examination.
- Inspection: look for deltoid or teres minor wasting in chronic cases (often subtle).
- Palpation: point tenderness over the quadrilateral space, felt just lateral to the lateral scapular border, is a useful (if non-specific) sign.
- Provocation: holding the arm in abduction and external rotation for about one minute reproduces the pain and paraesthesia.
- Neurology: test deltoid and teres minor power and the regimental-badge sensory patch over the lateral deltoid.
- Vascular: check distal pulses, capillary refill, and inspect the fingertips for emboli or splinter haemorrhages.
Always actively exclude the common mimics: rotator cuff disease (impingement signs, cuff weakness), suprascapular neuropathy (infraspinatus +/- supraspinatus wasting, spinoglenoid or suprascapular notch cyst - NOT teres minor), and cervical radiculopathy (neck pain, Spurling test, dermatomal pattern). QSS is what remains when these are excluded.
- Distinguishing Feature
- Posterolateral pain worse in abduction-ER; teres minor atrophy
- Confirming Test
- MRI + diagnostic block; angiography if vascular
- Distinguishing Feature
- Infraspinatus (+/- supraspinatus) wasting, NOT teres minor
- Confirming Test
- MRI spinoglenoid/paralabral cyst; EMG suprascapular nerve
- Distinguishing Feature
- Painful arc, cuff weakness, night pain
- Confirming Test
- Ultrasound / MRI cuff
- Distinguishing Feature
- Neck pain, dermatomal symptoms, positive Spurling
- Confirming Test
- MRI cervical spine; EMG
- Distinguishing Feature
- Acute severe pain then patchy weakness/atrophy
- Confirming Test
- EMG (multifocal), clinical course
Investigations
There is no single diagnostic test for QSS; the workup is built to exclude mimics and to support the clinical impression.
Plain radiographs - usually normal; obtained to exclude bony lesions (osteochondroma), old fracture, or calcification.
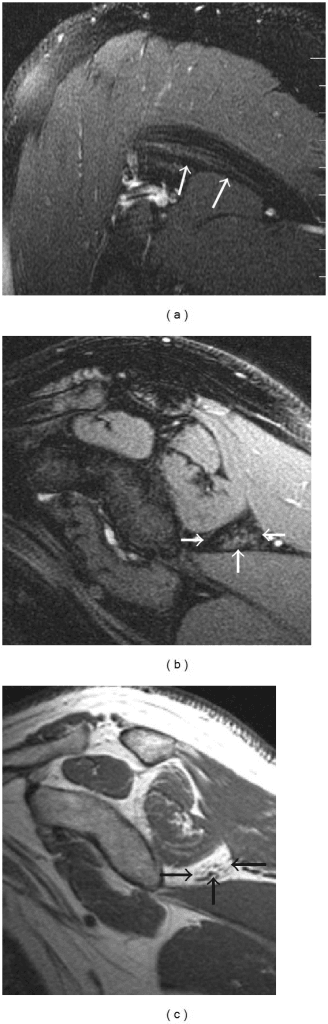
MRI - the most useful single test. Look for:
- Teres minor denervation / fatty atrophy (sensitive but not specific)
- Deltoid denervation in more advanced axillary nerve involvement
- Space-occupying lesions - paralabral cyst, mass, or PCHA aneurysm
Ultrasound - increasingly used; can dynamically assess the PCHA during abduction-external rotation with colour Doppler and can guide a diagnostic block.
Electromyography / nerve conduction studies - may show axillary neuropathy and help exclude suprascapular and cervical causes, but can be normal in early or purely vascular disease.
Angiography (CT, MR or catheter) - reserved for suspected vascular QSS; dynamic imaging in abduction-external rotation may be required to demonstrate PCHA occlusion or aneurysm that is not seen in the neutral position.
Image-guided quadrilateral space / axillary nerve block - meaningful pain relief after a local anaesthetic block within the quadrilateral space, in the right clinical context, is one of the most useful confirmatory findings.
A young dominant-arm athlete presenting with digital ischaemia, cold intolerance, or distal emboli may have vascular QSS. This warrants urgent vascular imaging (Doppler then angiography) and vascular surgical involvement - acute ischaemia can require emergent thrombolysis or thrombectomy.
The Diagnostic Quadrilateral-Space Block
The block is cited throughout as the single most useful confirmatory test — here is how it is done and what it does (and does not) prove.
- What it is. An image-guided (ultrasound or fluoroscopic) injection of local anaesthetic (with or without corticosteroid) into the quadrilateral space around the axillary nerve.
- A positive result. Meaningful, temporary relief of the patient's characteristic posterolateral pain after the block, in the right clinical context, supports the quadrilateral space as the pain source and predicts a better response to decompression; added corticosteroid can also be therapeutic.
- Why it is central here. Because QSS is a diagnosis of exclusion with no gold-standard test and MRI teres minor atrophy is non-specific, a positive block is one of the few findings that localises the problem to the space — it is the confirmatory step in the work-up (the "C" in the SPACE approach).
- Its limits. The block is supportive, not definitive: a placebo response is possible, a poorly targeted injection can give a false negative, and a positive block does not distinguish neurogenic from vascular disease — so it never replaces excluding the mimics or screening for the vascular subtype.
Q: An image-guided quadrilateral-space local-anaesthetic block relieves the patient's pain — what does this tell you? A: It localises the pain to the quadrilateral space and, in the right clinical context, supports the diagnosis and predicts a better decompression outcome — the key confirmatory test given there is no gold standard. But it is supportive, not definitive (placebo response and mistargeting are possible) and does not exclude the vascular subtype — still screen for digital ischaemia.
Management Algorithm
Management is stepwise and depends on subtype. The default for neurogenic QSS is a prolonged non-operative trial; the threshold for early surgery is much lower in vascular disease or when a structural lesion is found.
Non-operative management (first-line, at least 6 months for neurogenic QSS)
- Activity / training modification - reduce provocative overhead loading; correct throwing mechanics
- Physiotherapy - posterior capsule and teres muscle stretching, scapular stabilisation, rotator cuff and periscapular strengthening
- NSAIDs for symptom control
- Image-guided injection - a quadrilateral space corticosteroid/local anaesthetic injection can be both diagnostic and therapeutic
A trial of at least 6 months is recommended before considering surgery in neurogenic QSS, because many athletes improve with load management and rehabilitation.
Surgical Technique
Open posterior quadrilateral space decompression
- Positioning: lateral decubitus or prone/semi-prone with the affected arm draped free
- Incision: centred over the posterior border of the deltoid, lateral to the posterior axillary fold
- Interval: retract the posterior border of deltoid to reveal the interval between teres minor and teres major
- Identify and protect: find the nerve to teres minor, trace it deep to the axillary nerve, and protect the posterior circumflex humeral vessels throughout
- Decompress: divide compressive fibrous bands around the nerve; free movement of the nerve confirms adequate release
- Lesion: excise any paralabral cyst, mass, or address an aneurysm as indicated
Complications
- Persistent posterolateral shoulder pain and loss of overhead performance
- Progressive axillary neuropathy with teres minor and deltoid weakness/atrophy
- Vascular: PCHA thrombosis, aneurysm, and distal embolisation causing digital ischaemia - potentially limb-threatening
- Iatrogenic axillary nerve injury (the very structure being protected)
- Injury to the posterior circumflex humeral vessels with bleeding or haematoma
- Incomplete decompression with persistent symptoms
- Recurrence (e.g. paralabral cyst recurrence if the labral tear is not addressed)
- Standard wound complications - infection, stiffness
Because isolated teres minor atrophy is common and usually NOT due to compressive QSS, the most clinically relevant pitfall is operating on a patient who does not have true QSS. Reserve surgery for refractory cases with a coherent clinical picture or a demonstrable structural lesion.
Postoperative Rehabilitation
Rehabilitation after decompression is staged and prioritises early protected motion with progressive return to overhead loading.
Sling for comfort, wound care, gentle pendulum and passive range of motion. Protect the axillary nerve repair/neurolysis.
Progress to active-assisted then active range of motion; begin scapular setting and periscapular activation. Avoid provocative abduction-external rotation loading.
Rotator cuff and deltoid strengthening, scapular stabilisation, and posterior capsule flexibility work.
Sport-specific and throwing progression once strength and painless overhead motion are restored; correct underlying mechanics. Return to sport timelines vary and are guided by symptom resolution and strength recovery.
In published case material, athletes who undergo decompression for refractory neurogenic QSS can regain deltoid bulk and strength and return to full sport, with restoration of muscle mass and durable relief reported over months to a couple of years of follow-up.
Outcomes and Prognosis
The evidence base is limited to small case series and case reports (Level 4), so prognostic statements must be cautious.
- Non-operative: many overhead athletes with neurogenic QSS improve with load management and rehabilitation, which is why a prolonged trial is recommended first.
- Surgical decompression: small series report good symptom relief and return to sport in appropriately selected refractory neurogenic cases.
- Vascular QSS: with timely diagnosis and combined vascular and decompressive surgery, distal ischaemia can be salvaged and baseline function restored; delay risks permanent tissue loss.
- Prognostic caveat: outcomes are best when the diagnosis is genuine. Operating on non-specific teres minor atrophy without a coherent clinical picture predicts a poor result.
Key Points and Practice
Q: Which two structures pass through the quadrilateral space and are compressed in QSS?
A: The axillary nerve and the posterior circumflex humeral artery (PCHA).
Q: What is the most useful single imaging test in suspected QSS, and what is its classic (if non-specific) finding?
A: MRI, looking for teres minor (+/- deltoid) denervation / fatty atrophy - sensitive but not specific.
Q: A young dominant-arm athlete presents with digital ischaemia and a dusky fingertip. Which QSS subtype is this and what is the priority?
A: Vascular QSS (PCHA thrombosis/aneurysm/emboli) - urgent vascular imaging and surgery; it can be limb-threatening.
Q: How long is non-operative treatment generally trialled before considering surgery in neurogenic QSS?
A: At least 6 months.
Guidelines, Registries and Global Practice
There are no formal society guidelines or registries specific to quadrilateral space syndrome - it is too rare, and the literature is Level 4 (case series and reports). Practice is therefore consensus-based and consistent across regions.
- QSS is a diagnosis of exclusion; rule out the common shoulder mimics first (rotator cuff disease, suprascapular neuropathy, cervical radiculopathy).
- MRI is the primary imaging test worldwide; dynamic ultrasound is a useful, inexpensive, widely available adjunct for the neurovascular bundle and for guided blocks.
- A positive image-guided quadrilateral space block is a widely accepted supportive test where the diagnosis is uncertain.
- Non-operative care for at least 6 months is the accepted first-line for neurogenic disease; surgical decompression is reserved for refractory or structural disease.
- The vascular subtype is managed jointly with vascular surgery, with endovascular therapy for acute ischaemia - a pathway that depends on local interventional radiology and vascular surgery availability.
access to dynamic angiography, musculoskeletal ultrasound, and catheter-directed endovascular therapy differs by resource setting, which influences how quickly the vascular subtype is diagnosed and treated.
Memory Aids
TILTQuadrilateral Space Borders
Hook:TILT the shoulder into abduction-ER and the quadrilateral space narrows.
SPACEQSS Diagnostic Workup
Hook:Work through the SPACE before you blame the space.
RESTQSS Management Ladder
Hook:REST the throwing arm first; theatre is the last rung.
Clinical Imaging
Imaging Atlas
For a focused review of the bony and muscular borders and the related triangular space and triangular interval, see the dedicated Quadrangular and Triangular Spaces anatomy topic and Axillary Nerve Anatomy.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old baseball pitcher presents with insidious posterolateral pain in his dominant shoulder and lateral arm tingling, worse when his arm is cocked back to throw. Cuff strength is preserved and his neck examination is normal. How would you approach this?”
“A 22-year-old elite volleyball player reports cold intolerance and painful, dusky fingertips in her dominant hand, with one fingertip showing a small area of discolouration. Shoulder movement is full but spiking provokes arm symptoms. What is your concern and how do you proceed?”
“A radiologist reports isolated fatty atrophy of the teres minor on a shoulder MRI ordered for impingement-type pain in a 58-year-old labourer. The referring team asks whether this means he has quadrilateral space syndrome. How do you advise them?”
Anatomy (TILT)
- Superior: teres minor
- Inferior: teres major
- Medial: long head of triceps
- Lateral: surgical neck of humerus
- Contents: axillary nerve + PCHA
Two Subtypes
- Neurogenic: axillary nerve - pain, paraesthesia, teres minor atrophy
- Vascular: PCHA - thrombosis, aneurysm, distal emboli
- Vascular can be limb-threatening
Clinical
- Overhead athlete, dominant arm
- Posterolateral pain worse in abduction-ER
- Point tenderness over the space
- Diagnosis of exclusion
Investigations
- MRI: teres minor / deltoid denervation
- Dynamic ultrasound + Doppler for PCHA
- Angiography (abduction-ER) if vascular
- Quadrilateral space block to confirm
Management
- Neurogenic: non-op 6+ months first
- Decompress bands / neurolysis if refractory
- Vascular: urgent thrombolysis/thrombectomy
- Aneurysm resection + decompression
Exam Traps
- Isolated teres minor atrophy = sensitive NOT specific
- Don't miss the vascular subtype
- Suprascapular nerve = infraspinatus, NOT teres minor
- Don't operate on incidental atrophy
Evidence Base
According to PubMed, the following sources inform current understanding of quadrilateral space syndrome.
Quadrilateral Space Syndrome: A Review
- QSS is a relatively rare compression of the axillary nerve and PCHA in the quadrilateral space
- Fibrous bands are most commonly implicated; true space-occupying lesions are less common
- Symptoms are non-dermatomal posterolateral pain aggravated by abduction-external rotation
- Lidocaine block within the space giving pain relief is a useful diagnostic finding
- At least 6 months of non-operative treatment is recommended before surgery
Quadrilateral Space Syndrome (vascular and interventional perspective)
- Both the axillary nerve and PCHA are susceptible to compression in the quadrilateral space
- Overhead athletes are at greater risk; presentation may be neurogenic or vascular
- MRI may show teres minor or deltoid atrophy; angiography may show PCHA aneurysm or occlusion
- Emboli from the PCHA can cause acute upper-limb ischaemia requiring catheter-directed thrombolysis or thrombectomy
Exploring the Quadrilateral Space: Clinical Anatomy, Pathology and Imaging Insights
- MRI is the gold-standard imaging modality for QSS
- Ultrasound complements MRI by dynamically assessing neurovascular structures with Doppler
- CT and radiographs help identify bony lesions such as osteochondroma or tumour
- Conservative care (physiotherapy, ultrasound-guided steroid injection) is first-line; surgery is reserved for refractory or structural/vascular disease
Axillary Nerve Decompression for Neurogenic QSS in a Volleyball Player
- 21-year-old competitive volleyball player with 5-year progressive arm weakness and deltoid atrophy
- EMG showed deltoid denervation; MRI showed axillary nerve compression in the quadrangular space
- Posterior microsurgical decompression divided a compressive fibrotic band after failed conservative care
- Restored deltoid mass and strength by 6 months with durable relief and full return to sport at 2 years