Destructive Arthropathy of an Insensate Joint
- A CHARCOT (NEUROPATHIC) JOINT is a progressive, DESTRUCTIVE arthropathy occurring in an INSENSATE joint: the loss of protective pain sensation and proprioception leads to repeated, unperceived microtrauma and accelerating joint destruction with fragmentation and intra-articular debris.
- At the ELBOW (and shoulder), the CLASSIC underlying cause is SYRINGOMYELIA - syringomyelia is a prevalent cause of Charcot arthropathy, notably affecting the elbow - so a neuropathic elbow should prompt a search for a cervical-cord SYRINX (other upper-limb sensory neuropathies can also cause it).
- The PRESENTATION is characteristic and paradoxical: a strikingly SWOLLEN, often grossly UNSTABLE elbow with MARKED radiographic DESTRUCTION (fragmentation, debris, sometimes an expansile destructive/'mass-like' appearance) that is RELATIVELY PAINLESS - the destruction is OUT OF PROPORTION to the patient's pain/symptoms, which is the key clue.
- DIAGNOSIS requires recognising the neuropathic picture, EXAMINING for the SENSORY deficit (dissociated sensory loss - pain/temperature - in syringomyelia), and IMAGING: radiographs/CT of the elbow (destruction/debris) and crucially MRI of the CERVICAL SPINE to detect a SYRINX - extended to the CRANIOCERVICAL JUNCTION, because a CHIARI malformation was present in 11 of 12 patients in one neurosurgical series. Check the SIDE: the syrinx was concordant with the affected limb in every patient in that series, so a contralateral syrinx should prompt a rethink.
- The crucial DIFFERENTIAL is INFECTION (septic arthritis/osteomyelitis) and TUMOUR - because the grossly destructive, sometimes expansile appearance can MIMIC malignancy or infection; a thorough work-up (and biopsy where genuinely uncertain) is needed before attributing destruction to neuropathic arthropathy, and other causes must be excluded.
- MANAGEMENT is largely SUPPORTIVE/conservative - PROTECT the joint (bracing/splinting, activity modification) and TREAT the UNDERLYING CAUSE. Decompressing the syrinx appears to protect the joint, not just the cord: in a 12-patient series none of the five who had neurosurgery deteriorated, against five of seven who did not - a small, confounded comparison, but the reason it is offered. SURGERY on the joint itself (arthrodesis, or arthroplasty) is LIMITED and considered HIGH-RISK in neuropathic joints, though no series reporting its outcome specifically at the NEUROPATHIC ELBOW was retrieved, so that caution is extrapolated rather than measured; a multidisciplinary approach (with neurosurgery) is important.
- “Charcot (neuropathic) elbow = progressive DESTRUCTION of an INSENSATE joint; the destruction is OUT OF PROPORTION to the (relatively painless) symptoms - the key clue.
- “Classic cause at the elbow/upper limb = SYRINGOMYELIA -> always MRI the CERVICAL SPINE for a syrinx (look for dissociated sensory loss). Other sensory neuropathies also cause it.
- “Differential = INFECTION and TUMOUR (the destructive/expansile appearance can mimic malignancy) - exclude them. Management = supportive (protect/brace) + treat the cause (syrinx decompression); joint surgery (arthrodesis/arthroplasty) is limited and HIGH-RISK.
A swollen, unstable, relatively painless elbow with marked radiographic destruction/debris - destruction out of proportion to symptoms = Charcot (neuropathic) joint. Examine for sensory loss.
Classic cause = syringomyelia -> MRI the cervical spine. Exclude infection and tumour (the destructive/expansile appearance can mimic malignancy).
The Cause Depends on the Site: Why the Upper Limb Points to a Syrinx
- Upper limb (elbow/shoulder/wrist/hand). Syringomyelia is the classic cause - a cervical-cord syrinx produces the upper-limb sensory loss. Other upper-limb causes are cervical spondylotic myelopathy/radiculopathy, brachial plexus injury, leprosy (Hansen disease) and peripheral nerve injury.
- Lower limb / foot (for contrast). Diabetes mellitus is now the commonest cause overall; tabes dorsalis (neurosyphilis) is the historical classic (knee/hip/spine); also alcoholic and other peripheral neuropathies, spinal cord injury, and myelomeningocele/spina bifida.
- The rule. The site points to the cause: an insensate elbow or shoulder should trigger a search for a syrinx (MRI of the cervical cord), whereas an insensate foot points to diabetes - so the location of the neuropathic joint directs the neurological work-up.
Q: Why does a Charcot elbow point to syringomyelia rather than diabetes?
A: The site points to the cause. Upper-limb Charcot joints (elbow/shoulder) are classically caused by syringomyelia (a cervical-cord syrinx causing upper-limb sensory loss) - also cervical spondylotic myelopathy, brachial plexus injury and leprosy. Lower-limb/foot Charcot joints are dominated by diabetes (commonest overall) and historically tabes dorsalis. So an insensate elbow triggers an MRI of the cervical cord for a syrinx, whereas an insensate foot points to diabetes.
The Dissociated Sensory Loss That Drives the Elbow
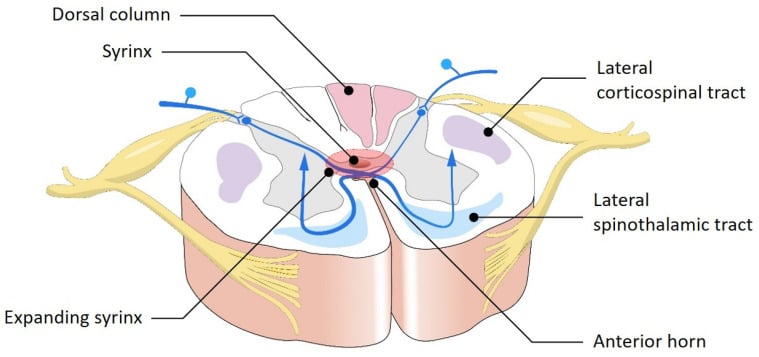
- Why dissociated. A syrinx expands the central canal and first interrupts the decussating spinothalamic fibres (pain and temperature) crossing in the anterior commissure, while the dorsal columns (fine touch, proprioception, vibration) are spared early - so there is loss of pain and temperature with preserved light touch ("dissociated" or "suspended" sensory loss), classically in a "cape"/shawl distribution over the shoulders and upper limbs.
- Why the upper limb. A cervical / upper-thoracic syrinx affects the upper limbs - which is why the neuropathic joint occurs at the elbow or shoulder, and why the loss of protective pain sensation there allows the joint to be destroyed unnoticed.
- Associated neurology to examine. Look for lower-motor-neuron signs in the hands (wasting/weakness from anterior-horn-cell involvement) and lost upper-limb reflexes; with expansion, long-tract (spastic lower-limb) signs, scoliosis and Horner syndrome; and the common association with a Chiari I malformation.
Q: Explain the dissociated sensory loss in the syringomyelic Charcot elbow.
A: The syrinx expands the central canal and first interrupts the decussating spinothalamic fibres (pain/temperature) in the anterior commissure while sparing the dorsal columns - giving loss of pain and temperature with preserved light touch ("dissociated"/"suspended" loss) in a cape distribution. A cervical syrinx affects the upper limbs, so the insensate elbow/shoulder is destroyed unnoticed. Also examine for hand wasting/lost reflexes (anterior-horn cells), long-tract signs, scoliosis, Horner syndrome and an associated Chiari I malformation.
Does Treating the Syrinx Change the Joint?
Telling a patient to have neurosurgery for the sake of the elbow needs more than plausibility behind it. A neurosurgical cohort followed exactly this question.
Twelve patients with neuropathic arthropathy from syringomyelia were followed a mean of 39 months. Five underwent neurosurgery (four posterior fossa decompression, one syringo-subarachnoid shunt); none of those five deteriorated, and all reported improved neurological function. Of the seven who did not, five had aggravation of the arthropathy, four of them with worsening neurological symptoms, and only two remained stable. No patient had joint surgery. That is 12 patients, retrospective and unrandomised, and the ones offered neurosurgery were selected - but it is the closest available answer, and it supports treating the syrinx as disease-modifying for the joint rather than merely for the neurology.
In that series the elbow was the commonest joint - 10 of 16 involved joints, ahead of the shoulder (three), interphalangeal joints (two) and wrist (one), which puts a number to the usual claim. More useful at the bedside: the side of the syrinx on axial cervical MRI matched the side of the affected limb in every patient. A syrinx that sits contralateral to the destroyed elbow should prompt a rethink rather than reassurance. Chiari malformation was present in 11 of the 12 and a tethered cord in the twelfth - so the MRI should cover the craniocervical junction, not the cervical cord alone.
Quote the cohort: elbow in 10 of 16 joints, Chiari in 11 of 12, syrinx side concordant with the affected limb in every patient, and after neurosurgical treatment none of five progressed against five of seven untreated. Small and retrospective, but it is why decompressing the syrinx is offered for the joint and not only for the cord.
Features, Work-up & Management
A Charcot (neuropathic) joint is a progressive, destructive arthropathy of an insensate joint - lost protective sensation/proprioception causes repeated unperceived microtrauma and destruction with fragmentation and debris. At the elbow (and shoulder), the classic cause is syringomyelia, so a neuropathic elbow mandates MRI of the cervical spine for a syrinx (look for dissociated pain/temperature sensory loss). The presentation is paradoxical - a strikingly swollen, unstable elbow with marked destruction that is relatively painless (destruction out of proportion to symptoms). The crucial differential is infection and tumour (the destructive/expansile appearance can mimic malignancy), which must be excluded. Management is largely supportive (protect/brace) plus treating the underlying cause (e.g. syrinx decompression); joint surgery (arthrodesis/arthroplasty) is limited and high-risk.
The Charcot elbow presents a double trap. First, the gross destruction is paradoxically associated with little pain, so the severity can be under-appreciated, and the markedly destructive, sometimes expansile and 'mass-like' radiographic appearance can be mistaken for a tumour or for infection - so infection (septic arthritis/ osteomyelitis) and malignancy must be excluded with appropriate investigations, and biopsy obtained where there is genuine uncertainty, before destruction is attributed to neuropathic arthropathy. Second, having recognised the neuropathic picture, the clinician must find the underlying cause: at the elbow (and shoulder) this is classically syringomyelia, so MRI of the cervical spine to detect a syrinx is essential, with examination for the dissociated (pain/temperature) sensory loss. Management is largely supportive - protecting the joint with bracing/activity modification - together with treatment of the underlying cause, such as neurosurgical decompression of a syrinx; surgery on the joint itself (arthrodesis or arthroplasty) is limited and is generally held to carry high failure and complication rates in the neuropathic, insensate joint, and is reserved for selected severe cases within a multidisciplinary (including neurosurgical) approach.

Mnemonics & Memory Aids
CHARCOT
Hook:CHARCOT: Cervical syrinx (MRI), Hugely swollen, (relatively) Asymptomatic, Radiographic destruction, exClude infection/tumour, Offload/protect, arThrodesis high-risk.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a grossly swollen, unstable, but relatively painless elbow with marked destruction on radiographs. What is the diagnosis, what must you investigate, and how do you manage it?”
What it is
- Progressive destructive arthropathy of an insensate joint
- Repeated unperceived microtrauma -> fragmentation/debris
- Destruction out of proportion to (relatively painless) symptoms
Cause & work-up
- Classic cause at elbow/upper limb = syringomyelia (also other sensory neuropathies)
- MRI the cervical spine for a syrinx; examine for dissociated sensory loss
- Exclude infection (septic arthritis/osteomyelitis) and tumour (can mimic malignancy)
Management
- Largely supportive: protect/brace, activity modification
- Treat the underlying cause: after decompression 0 of 5 progressed, against 5 of 7 untreated (n=12, confounded)
- MRI must cover the craniocervical junction (Chiari in 11 of 12) and the syrinx side should match the affected limb
- Joint surgery limited and held high-risk - no elbow-specific outcome series exists; multidisciplinary care
Evidence & Key Studies
Neuropathic arthropathy from a chronic syrinx (Charcot joint of the upper limb)
- Syringomyelia is a prevalent cause of Charcot arthropathy, notably affecting the elbow and (less frequently) the shoulder; neuropathic arthropathy can present as an expansile destructive mass on imaging, raising suspicion of malignancy.
- Diagnosis relies on a comprehensive assessment - clinical signs/symptoms, radiological imaging and tests to exclude other causes including soft-tissue tumours - and laboratory tests/biopsy were used to exclude malignancy.
- Management strategies range from conservative approaches to surgical interventions such as neurosurgical decompression (for the syrinx) and arthroplasty, with a multidisciplinary approach important for optimal outcomes.
Neuropathic arthropathy caused by syringomyelia: 12 patients, and what neurosurgery did to the joints
- Retrospective single-department review of 12 patients referred to neurosurgery between 2003 and 2012, with 16 involved joints and a mean follow-up of 39 months.
- The ELBOW was the commonest joint (10 of 16), followed by shoulder (3), interphalangeal (2) and wrist (1).
- MRI showed a syrinx in all 12, with Chiari malformation in 11 and a tethered cord in 1 - so imaging must cover the craniocervical junction.
- The side of the syrinx on axial cervical MRI was concordant with the side of the affected limb in EVERY patient.
- Five patients had neurosurgery (4 posterior fossa decompression, 1 syringo-subarachnoid shunt): all reported neurological improvement and NONE deteriorated with respect to the arthropathy. Of the 7 without neurosurgery, 5 had aggravation of the arthropathy and 2 were stable.
- No patient underwent surgery on the neuropathic joint itself.
- Twelve patients, retrospective, unrandomised and referred to a neurosurgical department - those offered decompression were selected, so the comparison is confounded by indication and cannot establish a treatment effect.
Syringomyelia as a prevalent cause of Charcot arthropathy notably affecting the elbow, the presentation as an expansile destructive 'mass' that can mimic malignancy, the need for a comprehensive assessment to exclude tumour/other causes (including biopsy where uncertain), and the management spectrum (conservative to neurosurgical decompression of the syrinx and arthroplasty, with a multidisciplinary approach) come from the cited Edara report. The general nature of neuropathic arthropathy (destruction of an insensate joint out of proportion to pain), the need to image the cervical spine for a syrinx, and the high-risk/limited role of joint surgery in neuropathic joints are standard, well-established teaching. The joint distribution, the Chiari and side-concordance findings and the outcomes with and without neurosurgical decompression come from the cited Deng series - 12 patients referred to a single neurosurgical department, retrospective and unrandomised, in which the patients offered decompression were selected, so it is confounded by indication and shows an association rather than a treatment effect. No series reporting the outcome of arthroplasty or arthrodesis specifically in the NEUROPATHIC ELBOW was retrieved; the statement that joint surgery carries high failure and complication rates is therefore an extrapolation from neuropathic joints at other sites and from general principle, and is labelled as such rather than given a rate. For contrast, a 10-patient shoulder series found reverse arthroplasty gave good or excellent results in the two patients who had it while conservative treatment relieved symptoms without restoring motion - shoulder data, not elbow. See also Charcot neuroarthropathy, neuropathic arthropathy of the shoulder, syringomyelia, Chiari malformation, total elbow arthroplasty and septic arthritis pathophysiology.