When the Intracapsular Neck Fails to Unite
- Nonunion complicates roughly 10-30% of femoral neck fractures despite modern fixation, and is much more common after DISPLACED (Garden III-IV) and VERTICAL (high Pauwels angle / Pauwels III) fractures, with POOR REDUCTION and posterior comminution as major risk factors.
- The femoral neck is prone to nonunion because it is INTRACAPSULAR: it has a precarious, retrograde retinacular blood supply, is bathed in synovial fluid with essentially NO PERIOSTEAL CALLUS (healing is by direct/intramembranous union), and a VERTICAL fracture experiences high SHEAR force that displaces rather than compresses the fragments.
- It presents months after fixation with persistent groin/hip pain, shortening and painful weight-bearing; radiographs show a persistent fracture line, hardware loosening/back-out or cut-out, and possibly femoral-head changes - assess for coexisting AVASCULAR NECROSIS (AVN), which frequently accompanies or follows nonunion.
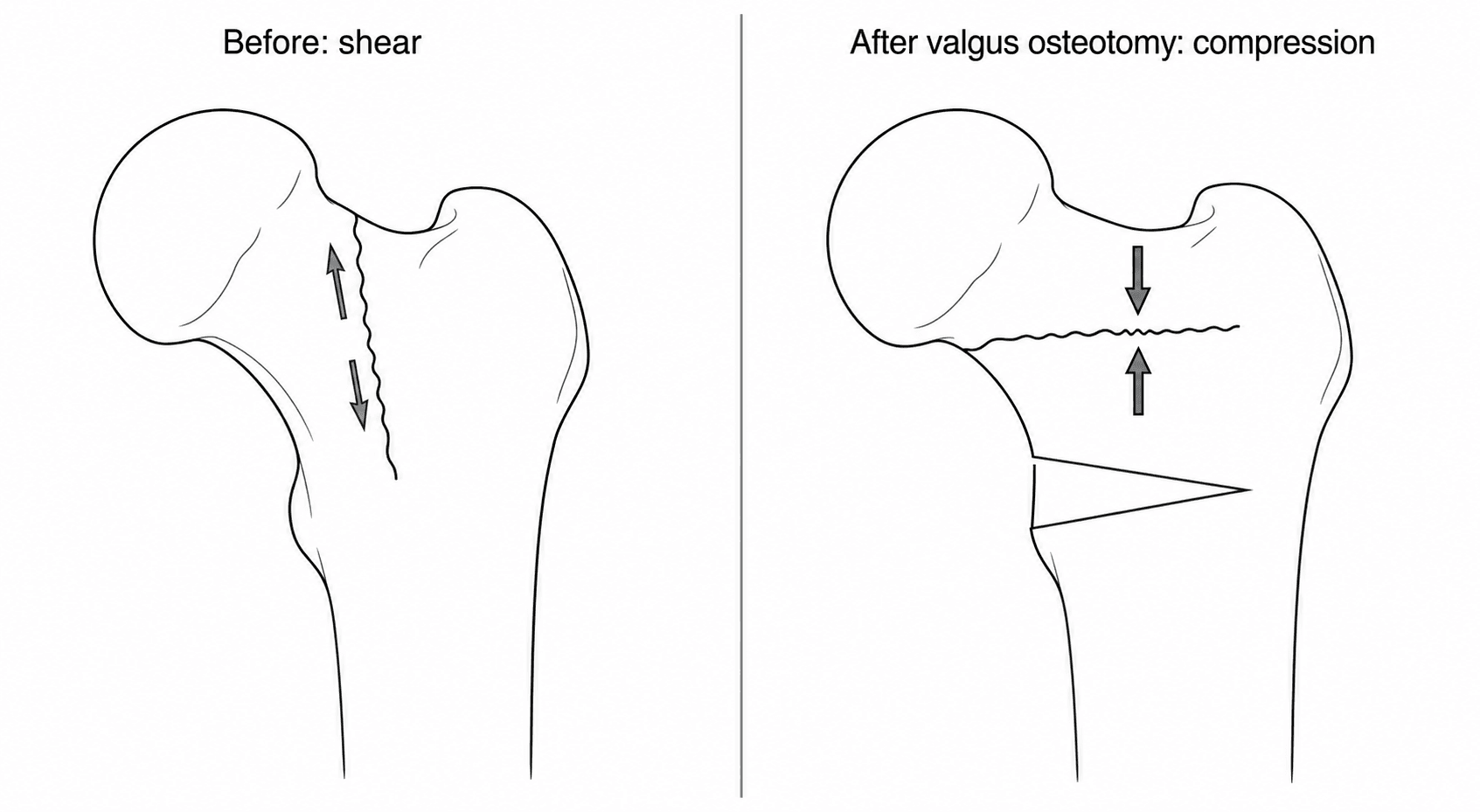
- The treatment decision is driven by PATIENT AGE and FEMORAL-HEAD VIABILITY: in a YOUNG patient with a VIABLE head, perform HEAD-PRESERVING surgery - a VALGUS INTERTROCHANTERIC OSTEOTOMY, which reorients the fracture so that the previously vertical (shear) fracture line becomes more HORIZONTAL and is loaded in COMPRESSION (the Pauwels principle), promoting union - often supplemented by bone grafting.
- In the ELDERLY, or when the head is NON-VIABLE (AVN/collapse), or after a FAILED osteotomy, ARTHROPLASTY (usually total hip replacement) is the treatment of choice - a reliable single operation allowing immediate weight-bearing.
- Valgus osteotomy achieves union in the large majority (small series report most or all united at around 12-13 weeks, though the published cohorts number only tens of patients and there are no comparative trials), but AVASCULAR NECROSIS remains a recognised complication that can necessitate later arthroplasty; modern variants (e.g. subtrochanteric valgus osteotomies) also restore the abductor lever arm and leg length while keeping later conversion to arthroplasty straightforward.
- “The femoral neck fails to unite because it is intracapsular (poor blood supply, no periosteal callus) and a vertical (Pauwels III) fracture is loaded in SHEAR.
- “Valgus intertrochanteric osteotomy works by making the fracture line more HORIZONTAL so it is loaded in COMPRESSION not shear (Pauwels principle) - for the YOUNG patient with a VIABLE head.
- “Elderly, AVN/non-viable head, or failed osteotomy -> arthroplasty (usually THR).
In a young patient whose femoral head is still viable, the goal is to keep the native head: a valgus intertrochanteric osteotomy converts the shear across the vertical nonunion into compression, reliably uniting it - avoid arthroplasty in the young if the head can be saved.
In the elderly, or when the head is non-viable (AVN/collapse) or an osteotomy has failed, arthroplasty (usually total hip replacement) is the reliable choice - a single operation with immediate weight-bearing.
Presentation & Assessment
- Persistent groin/hip pain and painful weight-bearing months after fixation
- Shortening and external rotation of the limb; limp
- Radiographic persistent fracture line, hardware back-out/cut-out or loosening, varus collapse
- Radiographs (+/- CT) to confirm nonunion and assess hardware/alignment
- Assess femoral-head VIABILITY - look for AVN (sclerosis, collapse) on X-ray; MRI to evaluate head vascularity, which is central to the treatment decision
- Consider patient age, demand and comorbidities
Avascular necrosis of the femoral head commonly coexists with, or develops after, femoral neck nonunion (the same vascular insult underlies both). Establishing whether the head is viable is the pivotal step: a viable head can be salvaged with osteotomy, whereas a dead or collapsing head mandates arthroplasty. AVN is also the main reason a valgus osteotomy may ultimately fail and require later replacement.
Management
The head-preserving operation of choice in the young. A closing-wedge valgus osteotomy at the intertrochanteric level tilts the head into valgus so that the previously vertical (shear) fracture line becomes more horizontal and is loaded in COMPRESSION (the Pauwels principle), fixed with an angled blade plate or equivalent; bone grafting (e.g. non-vascularised or vascularised fibular graft, or a muscle-pedicle graft) is often added for biology. Published series report union in most or all cases at around 12-13 weeks with good function - but read those numbers against their cohorts: the two series cited below contain 11 and 21 patients, there are no comparative trials, and "all united" out of eleven hips is a promising signal rather than a dependable rate. AVN remains a risk regardless.
Confirming the nonunion, and excluding the things that change the plan
When to call it. A femoral neck fracture that has not united by six months is a nonunion, but the decision rarely waits that long: progressive varus collapse, screw back-out or cut-out, and a fracture line that is widening rather than fading at three to four months are declaring failure early, and in a young patient there is nothing to gain by waiting for the calendar. Conversely, radiographs alone over-call it - the screws obscure the line and an apparently persistent lucency may be healing. CT is the test that settles whether the neck has united, and it also shows the bone stock, the position of the hardware and any posterior comminution that will matter for planning.
Exclude infection before you reconstruct anything. A nonunion around retained metal is a septic nonunion until shown otherwise, and this is the single omission that turns a valgus osteotomy into a disaster. Check CRP and ESR, ask specifically about wound problems or prolonged discharge after the index operation, and if there is any doubt aspirate the hip or take intra-operative samples for culture (multiple, off separate instruments) and histology before committing to a reconstruction. Infection changes the plan completely - towards debridement, hardware removal and staged treatment - and it is far better found before a blade plate is inserted than after.
Screen the patient's biology. An atrophic nonunion deserves the standard metabolic work-up: vitamin D, calcium, phosphate, parathyroid hormone and thyroid function, with smoking cessation, nutritional assessment and a review of medications (NSAIDs, steroids) - the same principles set out in Nonunion Management. It is unusual for a metabolic abnormality alone to explain a femoral neck nonunion, where mechanics and vascularity dominate, but correcting one is cheap and failing to look is indefensible in a nonunion that has already defeated one operation.
Arthroplasty After Failed Fixation: Not a Primary Hip Replacement
Arthroplasty is the commoner operation in this situation, and it is consistently underestimated: a total hip replacement after failed femoral neck fixation is a reconstructive procedure with higher complication rates than a primary, and the exam question is usually about exactly why.
- The hardware has to come out, and it may be broken, buried or stripped - have extraction sets available, and accept that removal can take longer than the arthroplasty.
- Screw holes are stress risers. Empty tracks in the lateral cortex and neck concentrate stress, and a fracture through one during broaching or in early weight-bearing is a recognised event. Consider a stem that bypasses the most distal hole by two cortical diameters, and be deliberate about it rather than hoping.
- Exposure is harder: scarring from the previous approach, capsular contracture, heterotopic bone and a shortened, adducted limb with contracted abductors all make dislocating the hip and restoring length more difficult than in a primary.
- Restoring leg length and offset is a genuine challenge when the neck has resorbed or collapsed into varus, and getting it wrong leaves the abductors weak and the patient with a limp and a Trendelenburg gait.
- Dislocation and infection rates are higher than primary arthroplasty - previous surgery, altered soft tissues and longer operative time all contribute - so implant choice should account for stability, and the patient should be counselled with these figures rather than primary-hip figures.
- Total hip replacement is generally preferred to hemiarthroplasty here: these patients are usually younger and more active than the typical acute hip-fracture patient, and the acetabular cartilage has often already been damaged by the collapsed head or protruding metal.
Assessing Head Viability: The Decision That Drives Everything
- Plain radiographs (established AVN): subchondral sclerosis, the crescent sign (a subchondral lucency) and head collapse/flattening all mark a failing/non-viable head.
- MRI - the most sensitive for marrow viability and pre-collapse AVN (the marrow-signal and double-line changes) - but beware metal artefact from the retained fixation, which may need metal-artefact-reduction sequences (or removing the hardware first) to read the head (the disease itself is in Avascular Necrosis of the Hip).
- Bone scan / SPECT: assesses head perfusion (reduced uptake = avascular) - useful where MRI is degraded by metal (technique in Bone Scan Interpretation).
- The intra-operative test: the real-time check is to drill the femoral head and look for punctate bleeding - a bleeding head is viable and can be salvaged by osteotomy; a dry, non-bleeding head is avascular and should be replaced. Confirm viability before committing to a head-preserving osteotomy.
Head viability decides osteotomy vs arthroplasty. Radiographs show established AVN (sclerosis, crescent sign, collapse); MRI is most sensitive pre-collapse but is degraded by retained metal (use MARS or a bone scan); and the intra-operative drill test - punctate bleeding = viable (salvage), dry head = avascular (replace) - is the real-time confirmation before an osteotomy.
Planning the Valgus Osteotomy: How Much, and the Trade-offs
- The goal sets the correction: reduce the steep (high-Pauwels) fracture line to a more horizontal orientation so load becomes compressive - broadly bringing the fracture line into the compression range (roughly below 30 degrees from horizontal); the amount of valgus is the wedge angle needed to achieve that, templated pre-operatively (the classification itself is in Neck of Femur Fracture).
- The technique: a laterally-based, medial closing wedge at the intertrochanteric level, held by a fixed-angle device (an angled blade plate or equivalent) that sets and maintains the correction; bone graft is added for biology.
- The trade-offs to counsel: a medial closing-wedge valgus osteotomy shortens the limb and shifts the proximal femur, which can medialise the shaft / shorten the abductor lever arm and cause a leg-length discrepancy and a Trendelenburg-type gait. The SALVA (subtrochanteric angulation + lateral translation) variant is designed to restore the abductor lever arm and limb length and to keep the proximal femur favourable for an easy later conversion to arthroplasty.
Plan the valgus by the wedge angle needed to horizontalise the fracture into compression (roughly below 30 degrees from horizontal), held by a fixed-angle blade plate with bone graft. Counsel that a medial closing wedge shortens and medialises the limb (LLD, weakened abductor lever arm) - the SALVA variant restores the abductor lever arm/limb length and eases a later arthroplasty.
Why the Femoral Neck Fails to Unite
The femoral neck is uniquely prone to nonunion for biological and mechanical reasons:
- Biology: it is intracapsular, with a precarious, largely retrograde retinacular blood supply (from the medial femoral circumflex artery) that the fracture itself can disrupt; it is bathed in synovial fluid; and there is essentially no periosteal callus - healing must occur by direct (intramembranous) union, which is unforgiving of any instability or gap.
- Mechanics: a vertical fracture line (a high Pauwels angle, Pauwels III) is loaded in SHEAR, which displaces the fragments rather than compressing them, defeating fixation. Risk factors are therefore displacement (Garden III-IV), a vertical/Pauwels III pattern, poor reduction, posterior comminution, and patient factors (smoking, etc.).
Mnemonics & Memory Aids
NECK
Hook:The NECK fails (no callus, end-artery supply); restore Compression and Know the head - then choose osteotomy or arthroplasty.
VALGUS
Hook:VALGUS osteotomy: drop the Pauwels angle to turn shear into compression in the young viable hip.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old develops a femoral neck nonunion 9 months after fixation of a displaced vertical fracture. Why did it fail to unite, and how would you decide on treatment?”
“When would you choose arthroplasty over osteotomy for a femoral neck nonunion, and what are the limitations of the osteotomy?”
Why it happens
- Nonunion in 10-30%; worse with displaced (Garden III-IV), vertical/Pauwels III, poor reduction
- Intracapsular: precarious retrograde blood supply, synovial fluid, NO periosteal callus (direct union)
- Vertical fracture loaded in SHEAR -> displacement
Assessment
- Persistent pain/painful weight-bearing months post-fixation; hardware back-out/cut-out, varus collapse
- Radiographs +/- CT; assess femoral-head VIABILITY (AVN) with MRI
- AVN frequently coexists - it drives the decision
Treatment
- Young + viable head: valgus intertrochanteric osteotomy (shear->compression, Pauwels) +/- bone graft
- Modern variant (SALVA) restores abductor lever arm/LLD; keeps later arthroplasty easy
- Elderly / non-viable head / failed osteotomy: arthroplasty (usually THR)
Outcomes & caveats
- Valgus osteotomy unites the large majority (~12-13 weeks)
- AVN is the main complication (may need later arthroplasty)
- Optimise biology/patient; exclude infection before reconstruction
Evidence & Key Studies
Valgus intertrochanteric osteotomy for non-union of femoral neck fracture
- Nonunion occurs in 10-30% of femoral neck fractures; valgus intertrochanteric osteotomy is a head-preserving option.
- In 11 cases, all nonunions healed (average 12.5 weeks); functional outcome was excellent in 9 and poor in 2, who underwent total hip arthroplasty for avascular necrosis.
- Valgus intertrochanteric osteotomy is effective for femoral neck nonunion, but AVN of the femoral head is a possible complication.
Treatment of non-united femoral neck fracture by a novel subtrochanteric angulation lateral translation valgus osteotomy (SALVA osteotomy)
- In 21 young adults (19-50 y) with non-united/neglected femoral neck fractures, the SALVA valgus osteotomy achieved consolidation in all, with improved functional and radiological outcomes.
- It restored the abductor lever arm and improved leg-length discrepancy; 3 developed AVN and 2 had mechanical failure (in marked osteopenia).
- A later, technically less demanding conversion to arthroplasty remains possible - valgus osteotomy is a reliable head-preserving option in the young.
The 10-30% nonunion rate and the effectiveness (and AVN risk) of valgus intertrochanteric osteotomy come from the cited Min series, and the young-adult head-preserving SALVA osteotomy outcomes from the cited Hegazy series. The intracapsular biology, the Pauwels shear-to-compression principle, and the age/head-viability treatment algorithm are standard, well-established teaching, as are the infection and metabolic work-up and the technical difficulties of arthroplasty after failed fixation. (See also Neck of Femur Fracture, Nonunion Management and Avascular Necrosis of the Hip.)