When Soft Tissue Turns to Bone
- Fibrodysplasia ossificans progressiva (FOP) is an ULTRA-RARE, AUTOSOMAL DOMINANT genetic disorder caused by a GAIN-OF-FUNCTION mutation in ACVR1 (ALK2) - the canonical R206H variant - which dysregulates BMP-type-I-receptor and ACTIVIN A signalling, causing progressive HETEROTOPIC OSSIFICATION (HO) that turns muscle, tendon, ligament and fascia into bone.
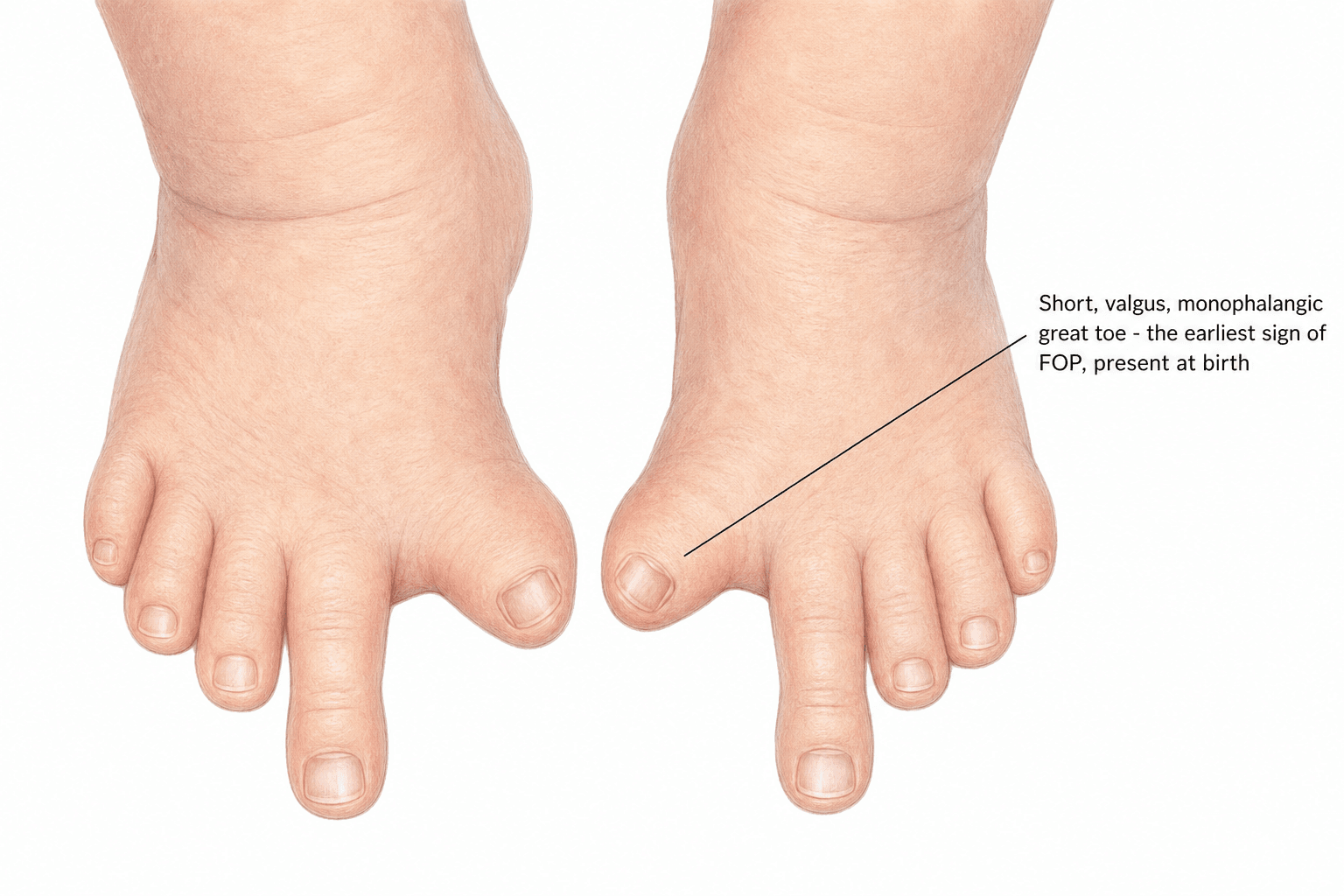
- There are TWO clinical hallmarks: (1) a congenital MALFORMATION OF THE GREAT TOES (short/valgus/monophalangic), present at BIRTH and the most penetrant feature - the diagnostic CLUE often visible before any HO; and (2) progressive HETEROTOPIC OSSIFICATION, which usually begins in early childhood as soft-tissue swellings ('flare-ups') that mature into bone.
- HO progresses in a characteristic ANATOMIC PATTERN - generally AXIAL to appendicular, CRANIAL to caudal, PROXIMAL to distal and DORSAL to ventral - and the flares are frequently TRIGGERED BY TRAUMA, including intramuscular INJECTIONS, BIOPSIES, SURGERY, dental/mandibular blocks, falls and viral illness.
- Because trauma triggers catastrophic HO, BIOPSY of a suspicious soft-tissue swelling is CONTRAINDICATED (the swelling is an FOP flare, NOT a tumour, and biopsy accelerates ossification), and INTRAMUSCULAR INJECTIONS and elective SURGERY (including excision of the heterotopic bone) must be AVOIDED - surgical excision of HO simply provokes more HO.
- DIAGNOSIS is CLINICAL - the combination of the malformed great toes and progressive soft-tissue ossification - and is confirmed by ACVR1 GENETIC testing; FOP is repeatedly MISDIAGNOSED as cancer or aggressive fibromatosis, leading to harmful biopsy, so recognising the great-toe clue is critical. Progressive joint ANKYLOSIS and costovertebral/thoracic ossification cause cumulative immobility and RESTRICTIVE LUNG disease (the main cause of death).
- There is NO cure: management is SUPPORTIVE and preventive - AVOID trauma/IM injections/surgery/biopsy, fall prevention, manage acute flares (high-dose corticosteroids for flares near major joints/the jaw, NSAIDs), dental care avoiding mandibular blocks, and respiratory monitoring; PALOVAROTENE (a retinoic-acid-receptor-gamma agonist) is approved to reduce HO, and Activin A-targeting and other agents are in development.
- “FOP = AD ACVR1 (ALK2) gain-of-function (R206H) -> Activin A-driven progressive heterotopic ossification (soft tissue -> bone).
- “Two hallmarks: congenital MALFORMED GREAT TOES (clue at birth) + progressive HO (axial->appendicular, proximal->distal).
- “TRAUMA triggers flares -> NO biopsy, NO IM injections, NO surgical excision of HO. Diagnose clinically + ACVR1; supportive care + palovarotene; restrictive lung disease = main cause of death.
A child with malformed great toes and soft-tissue swellings that turn to bone has FOP. The great- toe malformation is present at birth, before the heterotopic ossification.
Trauma triggers catastrophic HO - biopsy of the swelling, intramuscular injections and surgical excision of heterotopic bone all provoke more ossification. Diagnose clinically and avoid them.
Genetics & Pathophysiology
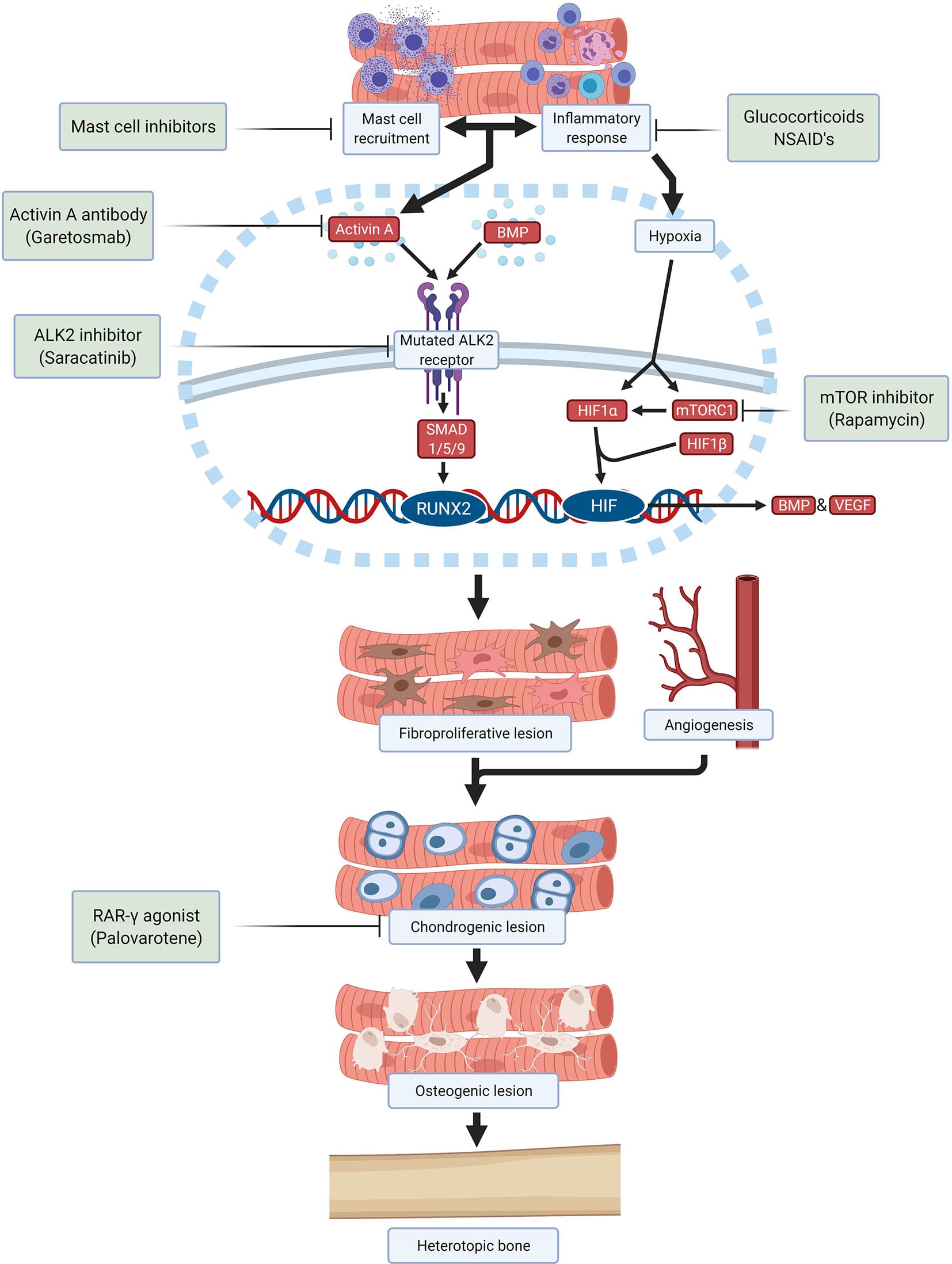
FOP is caused by an autosomal dominant gain-of-function mutation in ACVR1 (ALK2), a BMP type I receptor; the canonical mutation is R206H. The mutant receptor responds aberrantly to ACTIVIN A (which normally would not activate this pathway) and dysregulates BMP/SMAD signalling, so that, following an inflammatory/traumatic trigger, connective-tissue progenitor cells undergo a fibroproliferative -> chondrogenic -> osteogenic sequence that ends in mature heterotopic bone - effectively turning soft tissue into a second skeleton. This molecular understanding underlies the emerging therapies (Activin A antibodies, ALK2 inhibitors, the retinoic-acid-receptor-gamma agonist palovarotene).
Clinical Course & Diagnosis
The malformed great toes are present at birth and are the key early clue. HO typically begins in early childhood as painful soft-tissue swellings ('flare-ups') - often after trauma or illness - that mature into bone, progressing in a characteristic axial-to-appendicular, cranial-to-caudal, proximal-to-distal pattern. Over time, bridging HO across joints causes cumulative ANKYLOSIS and immobility, and costovertebral/thoracic ossification produces restrictive lung disease, which is the main cause of death. FOP is frequently MISDIAGNOSED as a tumour or aggressive fibromatosis - leading to a harmful biopsy
- so the diagnosis should be made CLINICALLY from the great-toe malformation plus progressive ossification and confirmed by ACVR1 genetic testing, NOT by biopsy.
The course, and what accumulates along the way
The disease advances in steps rather than smoothly - long quiet periods punctuated by flares, each of which may resolve or may leave permanent bone. Ossification typically starts in the neck, back and shoulders in the first decade, reaching the hips and knees later, and by the third decade most patients need a wheelchair. Reported median survival is around the fourth to sixth decade, with thoracic insufficiency syndrome the usual terminal pathway: costovertebral and chest-wall ossification with spinal deformity produces progressive restriction, and death commonly follows a pneumonia the patient cannot clear or right heart failure.
The problems that accumulate short of that are the ones easily overlooked:
- Temporomandibular ankylosis, which restricts mouth opening and causes real nutritional compromise and weight loss as well as making the airway hazardous. Dental care must avoid mandibular blocks and forced opening.
- Conductive hearing loss, present in a substantial minority and often middle-ear in origin, worth screening for in children so it does not impair speech and schooling.
- Falls and fractures: a rigid, unbalanced patient with a fused spine falls badly, and fractures in FOP generally heal normally - but the trauma of a fall or of aggressive handling can itself set off a flare.
- Pressure sores and contractures from immobility and the inability to reposition.
- Ankylosis in a poor position, which is unfixable - unlike acquired heterotopic ossification, the bone cannot be excised, so posture and seating are managed by adapting the environment to the patient.
The Differential - and Why FOP Is Misdiagnosed
- Progressive osseous heteroplasia (POH): a GNAS-inactivating disorder with dermal/superficial ossification that progresses from the skin into deeper tissue, with normal great toes and no inflammatory flares - the closest genetic mimic, separated by the absent toe malformation and the top-down (skin-first) pattern (versus FOP's deep, flare-driven ossification).
- Acquired/localised heterotopic ossification - post-traumatic myositis ossificans, neurogenic HO and post-surgical HO: localised, follow a defined event, normal toes, and - critically - can be excised once mature, the opposite of FOP.
- Osteosarcoma / extraskeletal osteosarcoma and aggressive fibromatosis (desmoid): the malignant or aggressive soft-tissue mimics that prompt the catastrophic biopsy, because an early FOP flare can look like a soft-tissue mass.
The take-home: the congenital great-toe malformation plus soft-tissue-to-bone progression makes the diagnosis clinically (confirmed by ACVR1 testing) - so recognise it and do not biopsy a presumed tumour. (The individual mimics are covered in Myositis Ossificans, Osteosarcoma and Desmoid Tumor; note POH is GNAS-inactivating, distinct from the GNAS-activating McCune-Albright syndrome.)
The great-toe malformation discriminates FOP: POH (GNAS, dermal/top-down ossification, normal toes, no flares), acquired/myositis ossificans and neurogenic HO (localised, post-event, excisable), and osteosarcoma/desmoid (the malignant mimics that prompt biopsy) are the differentials. Diagnose clinically plus ACVR1 - never biopsy.
Management
- Avoid triggers: NO biopsy, NO intramuscular injections, NO elective surgery (including excision of heterotopic bone, which provokes more HO); avoid mandibular dental blocks; prevent falls; use intravenous/subcutaneous rather than IM medication routes.
- Acute flares: high-dose corticosteroids for flares involving major joints, the jaw or other critical areas, plus NSAIDs/symptom control.
- Disease-modifying: PALOVAROTENE (a retinoic-acid-receptor-gamma agonist) is approved to reduce new HO; Activin A-targeting antibodies and ALK2 inhibitors are in development.
- Supportive/MDT: respiratory monitoring and care (restrictive disease), dental care without IM blocks, occupational therapy/mobility aids, fall prevention, and anaesthetic precautions (difficult airway from cervical/jaw ankylosis - avoid IM injections and forced neck manipulation).
- Counselling: autosomal dominant inheritance and genetic counselling.
Treating a flare: the specifics
"High-dose corticosteroids" needs numbers and, more importantly, limits. The widely used regimen is prednisone around 2 mg/kg/day (to a ceiling of about 100 mg) for four days, started within 24 hours of the flare beginning - later than that and the window has largely passed. It is a short burst, not a taper and not a maintenance drug.
The limitation matters as much as the dose. Steroid bursts are reserved for flares affecting major joints, the jaw, or the submandibular region - the sites where a single flare can cost a joint or an airway. They are not used for flares of the back, neck and trunk, which are frequent and recurrent, because repeated courses would deliver a substantial cumulative steroid burden for a flare that is not threatening a critical structure. Those are managed with NSAIDs or COX-2 inhibitors and symptom control.
A submandibular flare is an emergency. Swelling in the floor of the mouth threatens the airway and swallowing in a patient who may already have limited mouth opening and a fused cervical spine, and it warrants urgent assessment rather than reassurance.
Palovarotene: approved, but not a benign drug
Palovarotene reduces new heterotopic ossification, and the pivotal open-label phase 3 trial is worth knowing in full, because what it cost is exactly what an orthopaedic surgeon needs to weigh:
- Efficacy was real but hard-won. The twelve-month interim analysis met futility criteria and dosing was paused; the trial continued on the recommendation of its data monitoring committee, and the benefit - roughly a 60% lower mean annualised new HO volume than natural-history controls - rests substantially on post hoc analyses rather than the prespecified one.
- Premature physeal closure occurred in 21 of 57 patients under 14 years - about 37%. In a growing child this is a drug that trades heterotopic bone for growth plates, which is precisely the trade an orthopaedic surgeon should be able to discuss. It is the reason for weight-adjusted dosing in the skeletally immature and for skeletal monitoring during treatment.
- Retinoid toxicity is near-universal (mucocutaneous effects in almost every patient), and post hoc imaging analysis suggested reduced vertebral bone mineral density and strength with increased vertebral fracture risk.
None of that means the drug should not be used - FOP is a devastating disease and the alternative has been nothing - but it is a genuine risk-benefit conversation in a skeletally immature patient, not a straightforward win. Garetosmab, an anti-activin A antibody, and ALK2 inhibitors are the agents in development behind it.
The single most important and exam-critical message is that in FOP, TRAUMA causes catastrophic heterotopic ossification, so a soft-tissue swelling must NOT be biopsied (it is a flare, not a tumour), intramuscular injections must be avoided, and the heterotopic bone must NOT be surgically excised because excision provokes even more ossification. The diagnosis is made clinically from the pathognomonic malformed great toes and progressive ossification and confirmed by ACVR1 genetic testing. Anaesthesia is hazardous because of cervical- spine and jaw ankylosis and restrictive lung disease, so any unavoidable procedure needs careful planning with avoidance of intramuscular injections, intubation trauma and forced manipulation.
The Radiographic Signature
- Great toe: a short, often valgus great toe that on radiograph shows monophalangism (a single, malformed phalanx) with a short/abnormal first metatarsal - the most penetrant and earliest radiographic clue, present before any heterotopic ossification (the thumbs may also be short).
- The heterotopic bone: early flares are radiographically occult soft-tissue swellings; ossification then appears and bridges across joints and along fascial planes and muscle as ribbons, sheets and plates of mature bone - a "second skeleton" - characteristically sparing the heart, smooth muscle, diaphragm, tongue and extraocular muscles.
- Other skeletal signatures: the cervical spine shows tall, narrow vertebral bodies with large posterior elements and early facet (posterior-element) fusion (which helps distinguish FOP from juvenile idiopathic arthritis); broad, short femoral necks; and proximal-medial-tibial osteochondroma-like exostoses.
Plain radiographs and CT define the great-toe malformation and the mature heterotopic bone and let you plan around it (airway/anaesthesia), and CT/bone scan can show an active flare - but the disease is characterised by imaging, not biopsy. (General heterotopic-ossification imaging is covered in Heterotopic Ossification; the point here is the FOP signature.)
Radiographic signature: a monophalangic short great toe (earliest clue, before HO), sheets/ribbons of HO sparing the diaphragm/heart/smooth muscle, tall narrow cervical vertebrae with facet fusion, broad femoral necks and proximal-tibial exostoses. Characterise on imaging - never biopsy.
How Rare, and Why the Family History Is Usually Silent
FOP affects roughly one person in one and a half to two million, with no ethnic, geographic or sex predilection - so most clinicians will meet at most one case, which is a large part of why it is misdiagnosed.
The inheritance point is the practically important one. FOP is autosomal dominant, but the overwhelming majority of cases arise from a spontaneous new mutation, so the family history is almost always negative and affected people rarely reproduce. A clinician who reasons "no family history, so it cannot be a dominant genetic condition" will reach the wrong conclusion and order the biopsy. Inherited cases do occur, and an affected parent transmits the mutation to half their children, which is what makes genetic counselling meaningful once a diagnosis is made.
Mnemonics & Memory Aids
FOP
Hook:FOP: malformed First toes, Ossifying soft tissue, Procedures forbidden.
NO TRAUMA
Hook:In FOP, avoid all TRAUMA - it triggers ossification.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child has malformed great toes and develops painful soft-tissue swellings that harden into bone. What is the diagnosis, the genetics, and the one thing you must NOT do?”
“How is FOP managed, and what causes death?”
Genetics & pathophysiology
- Autosomal dominant ACVR1 (ALK2) gain-of-function (R206H)
- Aberrant Activin A/BMP-SMAD signalling -> heterotopic ossification
- Soft tissue (muscle/tendon/ligament/fascia) -> bone
Two hallmarks
- Congenital MALFORMED GREAT TOES (at birth - the clue)
- Progressive heterotopic ossification (flares)
- Pattern: axial->appendicular, cranial->caudal, proximal->distal
Diagnosis & pitfalls
- CLINICAL (great toes + progressive HO) + ACVR1 genetics
- Trauma triggers HO: NO biopsy, NO IM injections, NO surgery/excision of HO
- Often misdiagnosed as cancer/fibromatosis (avoid harmful biopsy)
Management & prognosis
- Avoid triggers; high-dose steroids for flares; palovarotene reduces HO
- Respiratory care, dental care (no mandibular blocks), anaesthetic precautions
- Death usually from restrictive lung disease / thoracic insufficiency
Evidence & Key Studies
Molecular developmental biology of FOP: ACVR1, the great toe and skeletal patterning
- Heterotopic ossification is the most prominent feature of FOP, which is caused by missense mutations in ACVR1.
- The mutation affects skeletal development even before HO appears, producing the signature malformation of the great toes (the most penetrant phenotype).
- Other skeletal features include joint malformation and ankylosis (cervical spine, costovertebral joints) and characteristic facial features.
MMP-9 deficiency confers resilience in FOP (ACVR1 R206H, Activin A and trauma-triggered HO)
- FOP is driven by the canonical pathogenic ACVR1 R206H variant with the classic congenital great-toe malformation.
- Activin A is an obligate ligand for heterotopic ossification, and trauma/inflammation trigger HO - linking inflammation to ossification.
- Molecular dissection of an unusually resilient patient identified MMP-9 as a druggable node linking inflammation to HO, illustrating the trauma-inflammation-HO axis.
Reduction of new heterotopic ossification in the open-label phase 3 MOVE trial of palovarotene for FOP
- Single-arm open-label phase 3 trial (97 treated patients) compared with 101 natural-history controls: mean annualised new HO volume was 60% lower with palovarotene.
- The 12-month interim analysis MET FUTILITY CRITERIA and dosing was paused; the trial continued on the data monitoring committee's recommendation, and the efficacy signal rests substantially on post hoc analyses rather than the prespecified one.
- Premature physeal closure or epiphyseal disorder occurred in 21 of 57 patients aged under 14 (36.8%); 97.0% had a retinoid-associated adverse event and 29.3% a serious adverse event, and post hoc imaging showed reduced vertebral bone mineral density and strength with increased vertebral fracture risk.
The palovarotene efficacy estimate, the futility pause, the 36.8% rate of premature physeal closure in children under 14 and the vertebral bone findings come from the cited Pignolo MOVE trial. The ACVR1 basis, the signature great-toe malformation (most penetrant, present before HO) and the associated joint ankylosis come from the cited Towler review, and the R206H variant, the obligate role of Activin A and the trauma/inflammation trigger for HO from the cited Lounev study. The autosomal-dominant inheritance, the progressive ossification pattern, the contraindication to biopsy/IM injection/surgery, and the supportive management framework are standard, well-established teaching, as are the flare steroid regimen, the epidemiology and the accumulated complications. (See also Heterotopic Ossification, Myositis Ossificans and Skeletal Dysplasias.)