Ipsilateral Fractures Above & Below the Elbow
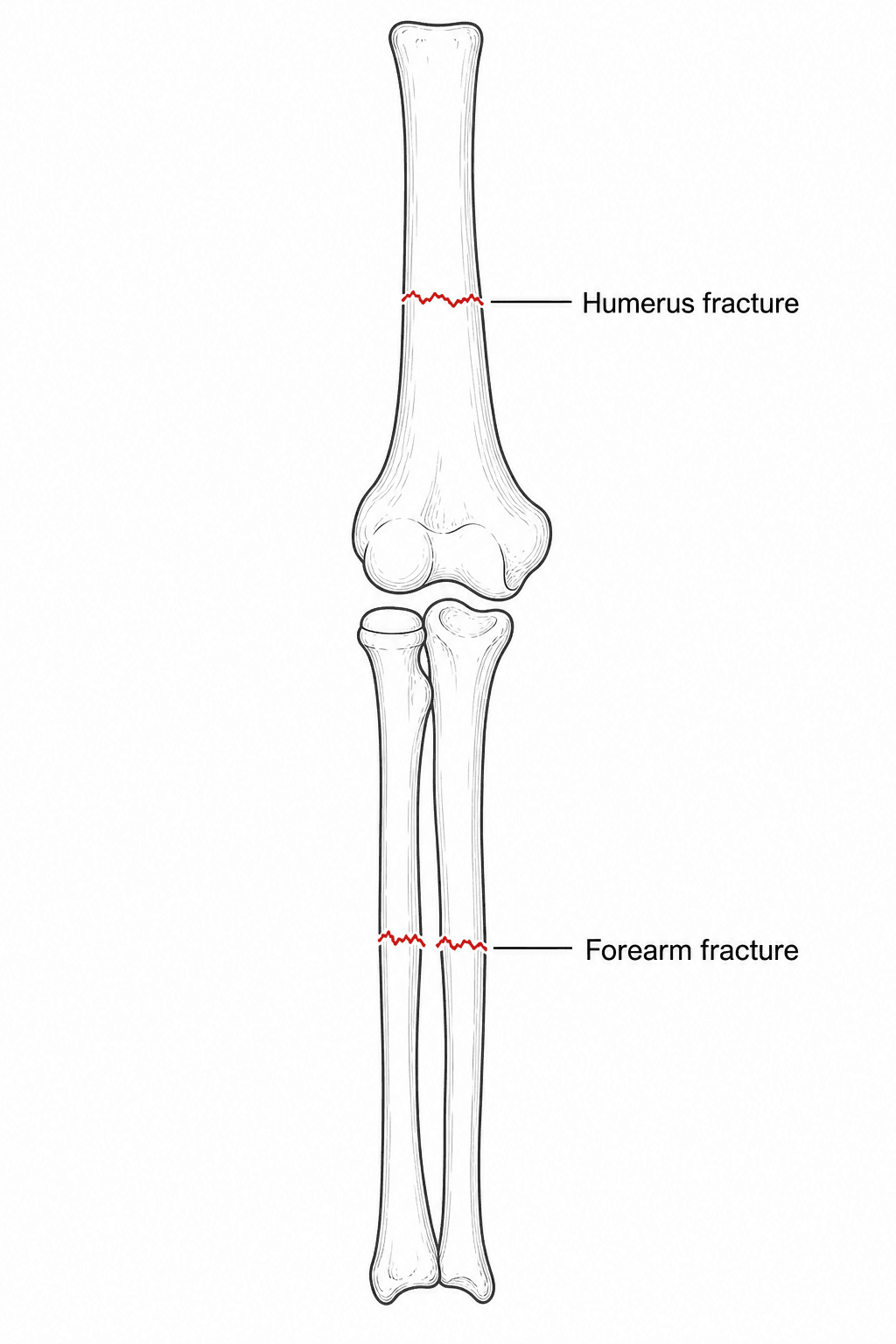
- A 'floating elbow' is the combination of IPSILATERAL fractures ABOVE and BELOW the elbow on the same limb, so the elbow joint is left flail/'floating' between them - classically a displaced SUPRACONDYLAR humerus fracture with an ipsilateral FOREARM fracture in CHILDREN, or a humeral (shaft/distal) plus forearm fracture in ADULTS.
- It is an indicator of HIGH-ENERGY trauma and carries a HIGHER incidence of OPEN fractures, NEUROVASCULAR injury (e.g. with supracondylar fractures - brachial artery, median/anterior interosseous and radial nerves) and the NEED for open reduction than isolated fractures.
- COMPARTMENT SYNDROME is a key risk - the high-energy mechanism, swelling, and combined fractures (and potential vascular injury) put the forearm at risk - so maintain a high index of suspicion and monitor closely.
- Management requires OPERATIVE STABILISATION of BOTH fractures: a flail elbow cannot be managed in a cast, and rigid fixation of both fractures allows early motion and protects against the complications. In children this is emergency reduction and percutaneous K-wire stabilisation of the supracondylar fracture plus reduction/fixation of the forearm; in adults, plate or nail fixation of the humerus and (usually plate) fixation of the forearm.
- Thorough NEUROVASCULAR assessment (before and after reduction) and treatment of any OPEN wounds (debridement, antibiotics) are essential; outcomes are good with prompt aggressive operative management, though they are worse than for isolated fractures because of the associated injuries.
- The take-home: a floating elbow is a high-energy, complication-prone injury that mandates aggressive operative treatment of both fractures and vigilance for neurovascular injury and compartment syndrome.
- “Floating elbow = ipsilateral fractures above AND below the elbow - a marker of HIGH-ENERGY trauma.
- “Expect (and look for) open fractures, neurovascular injury and COMPARTMENT SYNDROME - higher than isolated fractures.
- “Treat by stabilising BOTH fractures operatively (you cannot cast a flail elbow); early motion follows rigid fixation.
Fractures above and below the same elbow signal a high-energy injury, with higher rates of open fractures, neurovascular injury (brachial artery, median/AIN, radial, ulnar nerves) and the need for open reduction than isolated fractures.
The combination of high energy, swelling, two fractures and possible vascular injury makes forearm compartment syndrome a real risk - monitor closely, have a low threshold for pressure measurement, and beware the obtunded/young child who cannot report symptoms.
Definition & Patterns
The term 'floating elbow' describes ipsilateral fractures on both sides of the elbow - one above (humerus) and one below (forearm) - so the elbow joint is rendered flail / 'floating' between the two fractures. The classic paediatric pattern is a completely displaced supracondylar humerus fracture combined with an ipsilateral forearm fracture (distal radius or both-bone). In adults, the analogous injury is an ipsilateral humeral (shaft or distal) fracture with a forearm fracture. Whatever the exact bones, the injury reflects substantial energy transmitted through the limb.
Associated Injuries & Assessment
- Open fractures (higher incidence than isolated injuries)
- Neurovascular injury - brachial artery, median/anterior interosseous, radial and ulnar nerves (especially with displaced supracondylar fractures)
- Forearm compartment syndrome
- Other high-energy injuries (this is often a polytrauma limb)
- Full neurovascular examination before and after any reduction (pulses, perfusion, all nerves)
- Inspect for open wounds; assess soft-tissue swelling and compartments
- Radiographs of the whole limb (humerus, elbow, forearm, wrist) - do not miss the second fracture
- Treat as a high-energy / potential polytrauma patient (ATLS principles where relevant)
Maintain a high index of suspicion for forearm compartment syndrome - increasing analgesia requirement, pain on passive stretch and a tense forearm are key signs; in a child or obtunded patient, clinical signs are unreliable, so monitor closely and measure compartment pressures if in doubt. With a displaced supracondylar component, also assess the vascular status carefully - a pulseless hand (whether pale or the 'pink pulseless hand') after a high-energy elbow injury demands urgent reduction and reassessment, and vascular exploration if perfusion does not return.
Compartment syndrome: what "a high index of suspicion" actually means
Telling a candidate to be vigilant is not an answer. The examinable content is how you make the diagnosis and what you do about it.
In the child, the classic five Ps are useless. Pain, pallor, paraesthesia, paralysis and pulselessness are late signs, and pulselessness is often absent altogether - compartment pressure rises well above capillary filling pressure long before it occludes a major artery, so a palpable pulse never excludes the diagnosis. The early signs in a child are the three A's: increasing Analgesia requirement (the most useful single sign - a child needing escalating opioid after fixation is declaring itself), Anxiety and Agitation. Add to those pain on passive extension of the fingers, a tense, swollen forearm, and pain disproportionate to the injury.
Measure when the clinical picture is unreliable - the obtunded, intubated, very young or regionally blocked patient. The threshold is a delta P of less than 30 mmHg, that is, the diastolic blood pressure minus the measured compartment pressure. An absolute pressure alone is misleading in a hypotensive patient, which is why the differential is used. Measure in the compartment nearest the fracture and in the deep volar compartment, which is where the pressure is highest and where flexor digitorum profundus dies.
Fasciotomy is the treatment and it is time-critical. For the forearm this means a volar release through an extended Henry-type or curved ulnar-based incision, decompressing the superficial and - crucially - the deep flexor compartment, combined with a carpal tunnel release, and a separate dorsal incision for the extensor and mobile wad compartments if they remain tight after volar release. Leave the wounds open, re-look at 48 hours, and close or graft when swelling permits. Note that a regional block can mask the developing syndrome, which is a real argument against dense regional anaesthesia in exactly this injury.
The pulseless hand: pink is not the same as white
A pulseless hand comes in two forms, and they are managed differently.
- The white (or dusky), pulseless hand is an unperfused hand - cool, pale, sluggish or absent capillary refill. This is limb-threatening ischaemia. Reduce and stabilise the fracture immediately, and if perfusion does not return at once, explore the brachial artery with vascular surgical support. Do not observe it.
- The pink, pulseless hand is perfused but without a palpable radial pulse - warm, pink, with capillary refill, presumably supported by collateral flow. This is the genuinely contested one. After reduction and fixation the reasonable position is admission and close serial observation by an experienced team, with documented perfusion checks; but persistent pulselessness, any deterioration, or an inability to observe reliably should prompt vascular assessment and exploration rather than indefinite watching. The concern is not the missing pulse itself but the occult ischaemia and the developing compartment syndrome behind it, and there is a well-recognised subgroup whose collateral flow proves inadequate. A pink pulseless hand with rising analgesia requirement or a tense forearm is a compartment syndrome until proven otherwise, not a reassuring sign.
Management
A floating elbow requires operative stabilisation of BOTH fractures - a flail elbow between two fractures cannot be controlled in a cast, and rigid fixation of both allows early motion and reduces complications.
- Children: emergency closed (or open) reduction and percutaneous K-wire stabilisation of the supracondylar fracture, plus reduction and fixation (K-wires/plating as appropriate) of the forearm fracture. Higher rates of open reduction and nerve injury than isolated supracondylar fractures are expected.
- Adults: plate or nail fixation of the humeral fracture and (usually) plate fixation of the forearm fracture, restoring length, alignment and rotation to allow early rehabilitation.
- Always: treat open wounds (debridement, antibiotics, tetanus), monitor compartments, and perform/repeat neurovascular assessment; have a plan for fasciotomy and vascular repair if needed.
With prompt, aggressive operative management, outcomes are generally good - in the paediatric series cited below, 10 of 12 children achieved good or excellent results after emergency reduction and K-wire stabilisation of both fractures. Read that as a small single-centre series rather than a reliable rate: the injury is rare enough that the literature is case series and reports, with no comparative trials. Because of the associated injuries (open fractures, nerve injury, compartment syndrome), results are less predictable than for isolated fractures, and early recognition and treatment of those complications drives the outcome. Children generally do better than adults, whose stiffness, articular involvement and higher rate of open injury make a full functional recovery less likely.
Fixation Strategy: Which Fracture First, and Damage Control
- The goal. Rigid fixation of BOTH fractures converts the flail elbow into a stable segment and allows early motion, which is the single best protection against the elbow stiffness this injury otherwise causes.
- Which first. There is no absolute rule, but a common strategy is to stabilise the more proximal (humeral/supracondylar) fracture first - this restores a stable proximal segment/lever against which the forearm can then be reduced and fixed; some surgeons instead fix whichever fracture is simpler or more unstable first. In children: emergency CRPP of the supracondylar fracture to restore the elbow, then reduce/fix the forearm (K-wires/flexible nails or plate depending on level/age).
- Damage control when needed. In a grossly contaminated open injury or a physiologically unstable polytrauma patient, temporary spanning external fixation or K-wires (damage-control orthopaedics - developed in Damage Control Orthopaedics) buy time, with definitive fixation once the soft tissues and patient allow.
- Then move it. Once both are fixed, begin early supervised motion to protect against stiffness and forearm rotation loss.
Choosing the implants, and one position that must be avoided
In the child. The supracondylar fracture is stabilised with percutaneous K-wires - two or three lateral entry wires, or crossed wires accepting the ulnar nerve risk of the medial pin. The point specific to the floating elbow is that the forearm fracture must also be stabilised rather than treated in a cast as it might be in isolation: leaving it to a cast both fails to abolish the flail segment and requires a circumferential dressing over a maximally swelling limb. Fix it by flexible intramedullary nails, K-wires or a plate depending on level and age.
Do not immobilise the elbow in hyperflexion. Flexion beyond about 90 degrees markedly raises compartment pressure and reduces brachial artery flow, and in a limb already at high risk this is how an avoidable Volkmann's contracture is produced. This is precisely why the supracondylar fracture is pinned rather than held reduced by hyperflexion in a cast, and why the post-operative splint sits in less than 90 degrees with the dressing loose and split.
In the adult. Both fractures are usually plated. For the humerus, plate fixation is generally preferred to intramedullary nailing in this setting: it gives rotational control, permits direct reduction and, where the fracture is distal or intra-articular, is the only option - while an antegrade nail adds shoulder morbidity and controls rotation less well in a limb where the forearm is also unstable. Nailing remains reasonable for a segmental or pathological midshaft fracture, or in the polytrauma patient where speed and soft-tissue preservation dominate. The radial nerve must be identified or deliberately protected with a distal-third humeral fracture and again at plate removal. For the forearm, restore radial bow and length with plate fixation of both bones - malunion here costs pronation and supination, which is the function the patient will actually notice.
Fix both to abolish the flail segment and permit early motion. A workable sequence is to stabilise the proximal (supracondylar/humeral) fracture first to create a stable lever, then reduce and fix the forearm. In the contaminated-open or unstable-polytrauma limb, use temporary external fixation/K-wires (damage control) and convert to definitive fixation later.
Complications of the Floating Elbow
- Volkmann's ischaemic contracture. The devastating end-stage of an unrecognised forearm compartment syndrome (fixed flexion contracture of the wrist and fingers, intrinsic loss) - the reason for the relentless compartment vigilance (compartment syndrome detail in Forearm Compartment Syndrome).
- Elbow stiffness / loss of motion. The flail joint, extensive surgery and any immobilisation predispose to stiffness and lost forearm rotation; rigid fixation of both fractures with early motion is the main preventive (developed in Elbow Stiffness & Contracture).
- Nerve injury and recovery. A higher rate of median/anterior-interosseous, radial and ulnar nerve injury; most are traction neurapraxias that recover over weeks to months, but a nerve that is interposed in the fracture or lacerated (especially in an open injury) needs exploration - document and follow.
- Malunion / nonunion. Paediatric supracondylar malunion can give cubitus varus; forearm malunion reduces pronation/supination; adults risk nonunion of the humeral or forearm fracture.
- Other. Heterotopic ossification around the high-energy elbow, re-displacement/loss of fixation, and vascular sequelae.
The feared complication is Volkmann's ischaemic contracture from a missed compartment syndrome - hence the vigilance. The commonest functional problem is elbow stiffness / lost forearm rotation, prevented by rigid dual fixation and early motion. Expect nerve injuries (mostly recovering neurapraxias) and watch for malunion (cubitus varus in children; lost rotation from forearm malunion) and adult nonunion.
Mnemonics & Memory Aids
FLOAT
Hook:A FLOATing elbow: fractures both sides, look for nerve/vessel injury, fix both, watch compartments, high-energy.
BOTH
Hook:Fix BOTH, beware Open injury, the Tense forearm, and the Hand's perfusion.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A child falls from a height and has a displaced supracondylar humerus fracture and an ipsilateral distal forearm fracture. What is this injury, why does it concern you, and how would you manage it?”
“How does the floating elbow differ in adults, and what general principles guide its treatment?”
Definition
- Ipsilateral fractures above AND below the elbow (elbow flail/'floating')
- Children: displaced supracondylar + forearm fracture (classic)
- Adults: humeral (shaft/distal) + forearm fracture
Why it matters
- Marker of high-energy trauma
- Higher rates of open fractures, neurovascular injury, need for open reduction
- Forearm compartment syndrome risk
Assessment
- Neurovascular exam before/after reduction; inspect for open wounds
- Radiograph the whole limb (don't miss the 2nd fracture)
- Assess compartments; treat as high-energy/polytrauma
Management
- Operative stabilisation of BOTH fractures (can't cast a flail elbow)
- Children: CRPP supracondylar + forearm reduction/fixation; Adults: plate/nail humerus + plate forearm
- Treat open wounds; monitor compartments (low threshold for fasciotomy); repair vascular injury; early motion
Evidence & Key Studies
Management of the floating elbow injury in children: simultaneous ipsilateral fractures of the elbow and forearm
- In 12 children with a completely displaced supracondylar humerus fracture plus an ipsilateral forearm fracture, all underwent emergency operative reduction and percutaneous K-wire stabilisation; 10 had good/excellent and 2 fair results.
- The incidence of open fractures, nerve injury and the need for open reduction was higher than for isolated supracondylar fractures.
- The floating elbow is an indicator of a high-energy injury and requires aggressive operative management.
Paediatric bilateral 'floating elbow'
- Reports a rare bilateral floating elbow (ipsilateral supracondylar + distal forearm fractures bilaterally) managed by closed reduction and pinning, with uneventful union and no functional limitation.
- Emphasises vigilance for compartment syndrome in floating-elbow injuries.
- Concludes that early surgical fixation may give better results.
The high-energy nature, the higher rates of open fractures/nerve injury/open reduction, and the good results of emergency operative stabilisation come from the cited Harrington paediatric series, and the compartment-syndrome vigilance and early-fixation message from the cited Rangasamy report. The adult patterns and fixation principles are standard, well-established trauma teaching. The compartment-syndrome thresholds and fasciotomy technique, the pink-versus-white pulseless hand, the hyperflexion caution and the implant choices are standard, well-established trauma teaching. (See also Supracondylar Humerus Fracture, Both-Bone Forearm Fractures and Forearm Compartment Syndrome.)