A Common Injury with an Uncommon but Serious Tail of Infection
- Plantar puncture wounds are common and the GREAT MAJORITY heal uneventfully; only a small proportion - on the order of about 1.5-2% in published series - develop a deep infection that progresses to osteomyelitis or septic arthritis.
- The CLASSIC deep pathogen is PSEUDOMONAS AERUGINOSA, characteristically after a puncture THROUGH A RUBBER-SOLED SHOE (the warm, moist foam of a trainer/sneaker harbours Pseudomonas which is inoculated into the deep tissues); by contrast, early superficial CELLULITIS is usually due to Staphylococcus aureus or streptococci.
- A RETAINED FOREIGN BODY (nail fragment, wood, glass, sock/shoe debris) is a key driver of persistent infection and must be actively EXCLUDED - radio-opaque bodies (metal, glass, gravel) show on plain radiographs, while radiolucent material (wood, plastic) needs ULTRASOUND or MRI.
- TETANUS status must be checked and updated (puncture wounds are tetanus-prone); a full neurovascular and soft-tissue examination is needed, and the DEPTH and LOCATION matter - deep FOREFOOT punctures over the metatarsal heads/MTP joints carry the highest risk of bone and joint involvement.
- DIABETES (and peripheral neuropathy/vascular disease) markedly worsens the picture: infections are more often POLYMICROBIAL, may present late because of insensate feet, and carry a higher risk of chronic ulceration and AMPUTATION - the puncture can be the initiating injury of a diabetic foot infection.
- Management of a SIMPLE puncture is wound cleaning/irrigation, removal of any foreign body, tetanus prophylaxis and CLOSE follow-up; routine prophylactic antibiotics for clean simple punctures are NOT clearly beneficial (selective use only). Established DEEP infection or OSTEOMYELITIS requires SURGICAL DEBRIDEMENT with deep cultures and CULTURE-DIRECTED antibiotics (empirically covering Pseudomonas if deep/late), typically for several weeks.
- “Deep/late infection after a puncture through a trainer = Pseudomonas aeruginosa until proven otherwise; early cellulitis = S. aureus/Strep.
- “Always exclude a retained foreign body: plain film for radio-opaque, US/MRI for wood/plastic. Check tetanus.
- “Simple puncture: clean + foreign-body exclusion + tetanus + follow-up (no routine prophylactic antibiotics). Osteomyelitis: debride + culture-directed (anti-pseudomonal) antibiotics.
Superficial, within days - usually Staphylococcus aureus or streptococci. Treat with appropriate oral/IV antibiotics and review.
Abscess, septic arthritis or osteomyelitis - classically Pseudomonas aeruginosa, especially after a puncture through a rubber-soled shoe. Needs debridement + anti-pseudomonal, culture-directed antibiotics.
Mechanism & Why Some Get Infected
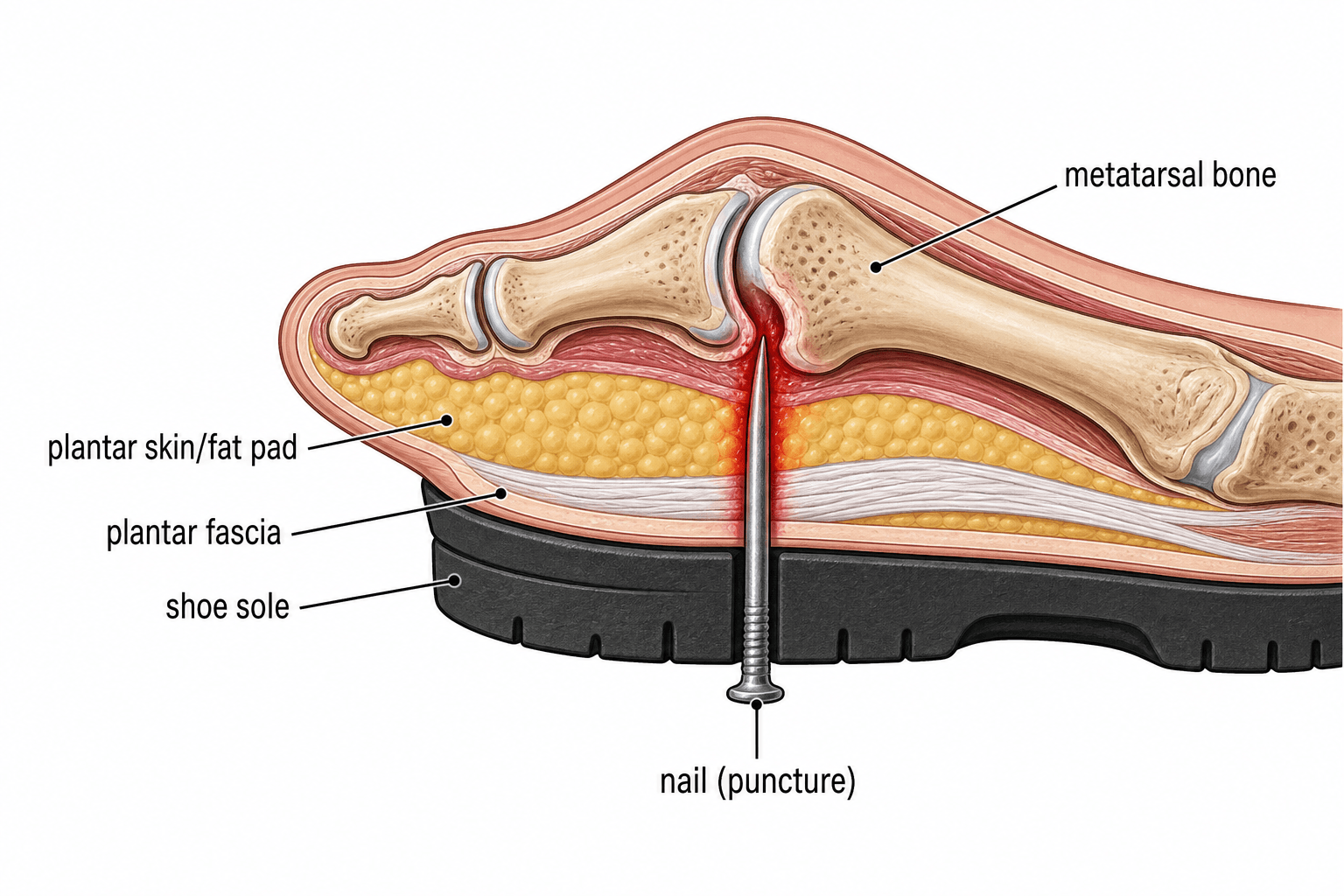
The typical injury is stepping on a nail. Most punctures are trivial, but several factors push a wound toward deep infection: a puncture through a rubber-soled shoe inoculates Pseudomonas aeruginosa from the warm, moist sole foam; a retained foreign body (nail fragment, wood splinter, glass, or a fragment of sock/shoe carried in) acts as a nidus; a deep puncture, and especially one over the forefoot (metatarsal heads / MTP joints), reaches bone and joint; delayed presentation, contamination, and host factors (diabetes, neuropathy, vascular disease, immunosuppression) all increase risk. Recognising these lets you stratify the wound that needs more than simple cleaning.
Where the Nail Went In Changes the Injury
The plantar surface is not uniform, and the site of entry predicts what is at risk - which is why the history should establish where as precisely as what.
- The forefoot, over the metatarsal heads and MTP joints, is the dangerous zone and the one that generates the classic cases. The soft-tissue envelope here is thin, so a nail that passes the skin and the plantar fat pad is immediately at the plantar plate, joint capsule and articular cartilage. Depth of only a couple of centimetres reaches bone. This is where pseudomonal septic arthritis and metatarsal osteomyelitis arise.
- The midfoot overlies the plantar fascia and the deep plantar compartments, so a deep puncture here can seed a closed space and present as a deep abscess rather than a superficial infection - and, rarely, as a compartment problem.
- The heel has a thick, chambered fat pad which is relatively resistant, but a nail that traverses it reaches the calcaneus, and calcaneal osteomyelitis is difficult to eradicate because the bone is largely cancellous with a thin cortex and a poor soft-tissue cover for reconstruction. Heel punctures also present late because the fat pad masks early swelling.
The practical consequence: a superficial midfoot scratch and a deep forefoot puncture through a trainer are the same "puncture wound" in the triage note and completely different problems, so record the site, estimated depth, and the object and footwear at first presentation - that record is what makes the later decision to image or explore defensible.
Microbiology and Antibiotic Choice
- Why Pseudomonas specifically. It colonises the warm, moist foam/insole of rubber-soled footwear and is inoculated deep; it also has a recognised affinity for cartilage, so a forefoot puncture that drives it onto the relatively avascular cartilage of the metatarsal head/MTP joint predisposes to pseudomonal chondral and osteoarticular infection.
- Early cellulitis (S. aureus / streptococci). Cover with an anti-staphylococcal/streptococcal agent such as flucloxacillin or cefazolin (clindamycin if penicillin-allergic).
- Deep / late infection (anti-pseudomonal). Empirically cover Pseudomonas with oral ciprofloxacin, or IV ceftazidime/cefepime, piperacillin-tazobactam or a carbapenem, sometimes with an aminoglycoside - then de-escalate to deep-culture sensitivities.
- Duration. Cellulitis needs a short course; established osteomyelitis needs a prolonged course (several weeks - the cited series report a mean of around five weeks), guided by the organism and the response.
Name it and dose it: early cellulitis = anti-staph/strep (flucloxacillin/cefazolin); deep/late through a trainer = anti-pseudomonal (ciprofloxacin orally, or ceftazidime/cefepime/piperacillin-tazobactam/carbapenem +/- aminoglycoside), then de-escalate on deep cultures. Pseudomonas is favoured by the moist foam sole and its cartilage affinity. Osteomyelitis = a several-week course.
Diagnosing Puncture-Wound Osteomyelitis
Confirming osteomyelitis after a puncture wound follows a defined sequence, and the radiographic lag is the reason MRI matters early (general infection imaging is developed in our Imaging Infection and White-Cell Scan topics).
- When to suspect it. The wound fails to settle - pain, swelling or discharge that persists or worsens beyond the first few days - or there is a deep forefoot puncture over the metatarsal heads/MTP joints.
- Plain radiographs are normal early. Osteomyelitis is radiographically silent for about 10-14 days, so a normal early film does NOT exclude it; later there may be lysis or periosteal reaction - the film's main early value is finding a radio-opaque foreign body.
- MRI is the most sensitive early test (marrow oedema, abscess, joint involvement and radiolucent foreign bodies); a labelled-white-cell or bone scan is an alternative when MRI is unavailable.
- Deep bone biopsy/culture at debridement is the gold standard for the organism - superficial swabs are unreliable/misleading; a positive probe-to-bone supports osteomyelitis, and CRP/ESR are supportive but non-specific.
Suspect osteomyelitis when a puncture fails to settle. A normal X-ray does not exclude it (silent for about ten to fourteen days - the film mainly finds a radio-opaque foreign body); MRI is the sensitive early test, and the organism comes from a deep bone culture (not a superficial swab) - probe-to-bone and raised CRP/ESR support the diagnosis.
Assessment & Imaging
Take a focused history (object, footwear, time since injury, environment, immunisation and diabetic/vascular status) and examine the wound for depth, location, contamination and signs of infection, with a full neurovascular assessment. A retained foreign body must be actively excluded:
- Plain radiographs detect radio-opaque bodies (metal, glass, gravel) and any bony changes (though osteomyelitis is radiographically silent for ~10-14 days).
- Ultrasound or MRI is needed for radiolucent material (wood, plastic, thorn) and to define deep abscess, septic arthritis or early osteomyelitis. Tetanus: puncture wounds are tetanus-prone - check status and give a booster +/- immunoglobulin as indicated.
"As indicated" - the tetanus rule in full
A puncture wound is by definition tetanus-prone, which is what lowers the threshold, so the decision turns on the patient's vaccination history rather than on how dirty the wound looks:
- Vaccine
- None needed
- Immunoglobulin
- No
- Vaccine
- Booster
- Immunoglobulin
- No
- Vaccine
- Vaccine + complete the primary course
- Immunoglobulin
- YES
Two points the table cannot carry. The 5-year threshold applies because a puncture is tetanus-prone - for a genuinely clean minor wound it would be 10 years, and a puncture is never that wound. And "unknown" belongs in the bottom row, not the top: an uncertain history is treated as incomplete rather than as probably fine, which is the decision that most often goes wrong.
Heavy contamination with soil or faeces, devitalised tissue, or presentation beyond about six hours all reinforce the tetanus-prone classification. The full schedule, immunoglobulin dosing and the special cases are in Tetanus Prophylaxis in Orthopaedics.
Wound care: what to do, and what not to do
"Clean and irrigate" needs qualifying, because a puncture tract is not a laceration.
- Clean the surrounding skin and the entry point, and irrigate the surface. Do not blindly probe or syringe fluid down the tract under pressure - it drives surface contaminant and shoe debris deeper into tissue planes that are hard to reach later.
- Do not soak the foot, which macerates the entry point without decontaminating the tract, and do not close the puncture.
- If the wound is deep, heavily contaminated, or a foreign body is suspected, explore it properly under anaesthesia with adequate light and extension of the entry wound rather than attempting it in the emergency department. Coring or excision of a contaminated tract is reasonable in that setting.
- Remove footwear debris deliberately: a fragment of insole foam or sock carried in is a classic retained nidus and is radiolucent, so it will not be on the radiograph.
Safety-netting that means something
Most of these patients go home, so the discharge advice is the intervention. Tell them explicitly to return if:
- Pain increases after an initial improvement - the single most useful warning, because it is the pattern of a deep infection declaring itself at 5 to 14 days rather than the steady settling of a simple wound.
- Fever, spreading redness, swelling or discharge appears.
- They cannot bear weight, or the toe or forefoot becomes painful to move passively - which suggests joint involvement rather than skin.
Arrange review at 48 to 72 hours for any deep forefoot puncture, any puncture through footwear, and every diabetic, neuropathic or immunocompromised patient, rather than relying on the patient to re-present.
Management
- Simple, clean puncture (no infection, no foreign body): thorough cleaning/irrigation, removal of any superficial foreign material, tetanus prophylaxis, dressing, analgesia and clear safety-netting with follow-up. Routine prophylactic antibiotics are not clearly beneficial for clean simple punctures and are used selectively (e.g. heavily contaminated wounds, deep forefoot punctures, immunocompromised/diabetic hosts).
- Cellulitis: antibiotics covering S. aureus/streptococci, with review to ensure resolution.
- Deep infection / abscess / septic arthritis / osteomyelitis: surgical debridement with removal of any foreign body and deep tissue/bone cultures, followed by culture-directed antibiotics - started empirically to cover Pseudomonas when the infection is deep or late - typically for several weeks (published series report a mean of around five weeks for osteomyelitis). Recurrent or extensive bone destruction may need repeat debridement.
In a patient with diabetes or peripheral neuropathy, a puncture wound may present late (insensate foot), is more likely to be polymicrobial, and can be the initiating injury of a limb-threatening diabetic foot infection with a higher risk of amputation. Have a low threshold for imaging, deep cultures, surgical debridement and multidisciplinary (vascular/diabetic-foot) involvement. (See Diabetic Foot and Charcot Neuroarthropathy.)
The complications to recognise
- Cellulitis and abscess - the common early problems, the abscess needing drainage rather than more antibiotics.
- Septic arthritis of an MTP joint and osteomyelitis of a metatarsal or the calcaneus - the serious tail of the injury, needing debridement and prolonged culture-directed therapy.
- Retained foreign body with a chronic sinus or granuloma - the wound that repeatedly settles on antibiotics and recurs when they stop is a retained foreign body until imaging proves otherwise, and no antibiotic course will resolve it.
- Necrotising soft-tissue infection - rare but the one not to miss: pain grossly out of proportion, systemic toxicity, rapid progression, skin changes and crepitus mandate immediate surgical exploration (see Necrotizing Fasciitis).
- Tetanus, the reason the prophylaxis rule above is not a formality.
- Chronic plantar pain or a tender scar at the entry site, and in the diabetic or neuropathic foot, chronic ulceration and amputation.
Mnemonics & Memory Aids
PUNCTURE
Hook:Run through PUNCTURE for every foot puncture wound.
BUGS
Hook:BUGS reminds you which organism to expect and to culture deep.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A healthy adult stepped on a nail through their trainer 10 days ago and now has a painful, swollen, discharging forefoot. What is the likely diagnosis and organism, and how would you manage them?”
“How does a foot puncture wound differ in a patient with diabetes, and why does that change your management?”
Epidemiology
- Common injury (typically stepping on a nail); most heal uneventfully
- ~1.5-2% develop deep infection / osteomyelitis
- Highest risk: deep forefoot punctures over metatarsal heads/MTP joints
Microbiology
- Early cellulitis: S. aureus / streptococci
- Deep/late through rubber sole: Pseudomonas aeruginosa
- Diabetic: polymicrobial; higher amputation risk
Assessment
- Exclude foreign body: X-ray (radio-opaque), US/MRI (radiolucent - wood/plastic)
- Check tetanus status; full neurovascular exam
- Inflammatory markers/cultures if infected; MRI for abscess/osteomyelitis
Management
- Simple: clean/irrigate, remove FB, tetanus, follow-up (no routine prophylactic antibiotics)
- Cellulitis: anti-staph/strep antibiotics
- Deep/osteomyelitis: debride + deep cultures + culture-directed (anti-pseudomonal) antibiotics ~weeks
Evidence & Key Studies
Calcaneal osteomyelitis caused by nail puncture wounds
- A small proportion (around 1.8%) of plantar puncture wounds become infected and progress to osteomyelitis.
- In six patients with calcaneal osteomyelitis after a heel nail-puncture, healthy patients grew a single pathogen, whereas diabetic patients grew MULTIPLE pathogens.
- The only amputation occurred in a diabetic patient; with diabetic neuropathy, the puncture may initiate chronic ulceration and raise amputation risk.
Pyogenic osteomyelitis after a plantar puncture wound: analysis of a series of 8 cases
- Osteoarticular infection followed plantar puncture in 1.65% of cases presenting to the emergency department; the mechanism was stepping on a nail in all cases.
- Cultures were monomicrobial in 6 of 8 cases, with Pseudomonas aeruginosa isolated in five - and a retained foreign body was found in one.
- Combined surgical and antibiotic treatment (mean antibiotic duration about five weeks) was used; initial proper wound treatment, foreign-body detection and follow-up are emphasised to prevent late infection.
The infection/osteomyelitis rates (~1.65-1.8%), the predominance of Pseudomonas aeruginosa in deep infection, the polymicrobial pattern and amputation risk in diabetics, and the role of foreign-body detection and several-week antibiotic courses come from the cited Laughlin and Morales series. The Pseudomonas-through-a-rubber-sole association is long-established clinical teaching, as are the tetanus thresholds, the wound-care cautions, the site-specific anatomy and the complications. (See also Osteomyelitis Pathophysiology, Septic Arthritis, Diabetic Foot, Tetanus Prophylaxis in Orthopaedics and Necrotizing Fasciitis.)