S100-Positive Schwann-Cell Tumour
- The GRANULAR CELL TUMOUR is an UNCOMMON, usually BENIGN soft-tissue tumour of SCHWANN-CELL (neural) origin - which is why it is S100-POSITIVE (and SOX10-positive) - composed of cells with characteristic abundant GRANULAR EOSINOPHILIC (lysosome-rich) cytoplasm.
- It typically presents as a SMALL, FIRM, often solitary DERMAL or SUBCUTANEOUS NODULE; the classic site is the TONGUE (and head/neck), but it also arises in the SKIN and SOFT TISSUE of the trunk and limbs, the breast, and (uncommonly) the gastrointestinal tract and other viscera. THE DEMOGRAPHICS ARE WORTH KNOWING: across 42 cases with a systematic review of 1,499, the mean age at diagnosis was 45.8 YEARS (range 6 to 69) and 60 PERCENT were FEMALE.
- PUT A NUMBER ON 'RARE MALIGNANT VARIANT' - AND NOTE THAT THE HISTOLOGICAL CRITERIA OVER-CALL IT. Applying the Fanburg-Smith criteria to that pooled literature classified 72 percent benign, 17 PERCENT ATYPICAL and 11 PERCENT MALIGNANT. But TRUE malignancy, defined by actual METASTASIS, occurred in only about 2.5 PERCENT - so the histological grading labels roughly FOUR TIMES as many tumours malignant as ever behave that way. Of the six criteria, NECROSIS and MITOTIC ACTIVITY were the most effective at identifying genuinely aggressive tumours.
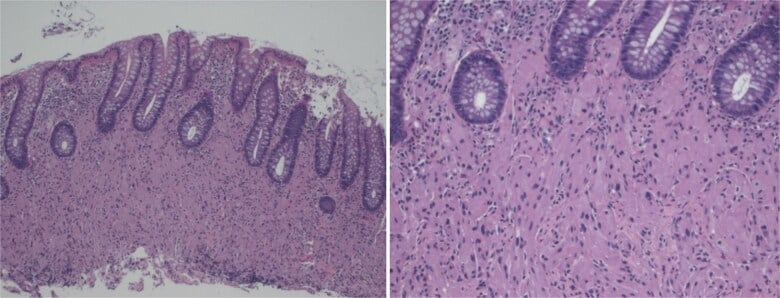
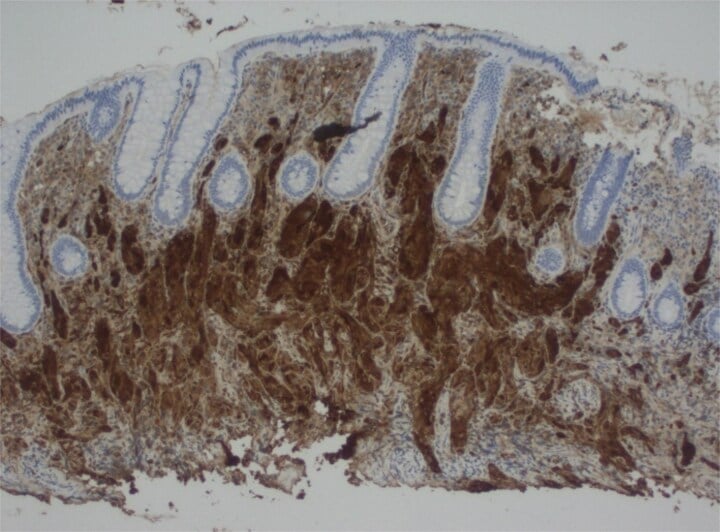
- HISTOLOGY shows nests or sheets of polygonal cells with abundant granular eosinophilic cytoplasm; immunohistochemistry confirms the neural (Schwann-cell) origin with S100/SOX10 positivity, and the overlying epithelium may show PSEUDOEPITHELIOMATOUS HYPERPLASIA, which can be mistaken for squamous cell carcinoma on a superficial biopsy.
- The vast majority are BENIGN, but a RARE MALIGNANT variant exists and is the dangerous one: features that raise concern include LARGE size (often over about 4-5 cm), RAPID growth, necrosis, increased mitotic activity/pleomorphism and infiltrative margins - malignant granular cell tumours carry a HIGH risk of local recurrence and METASTASIS and significant mortality.
- The DIFFERENTIAL includes other granular/eosinophilic lesions and, because of the pseudoepitheliomatous hyperplasia, squamous cell carcinoma on a small/superficial biopsy - so adequate sampling and S100/SOX10 staining are important to confirm the diagnosis and avoid over-diagnosis of carcinoma.
- A POSITIVE MARGIN IS NOT AUTOMATICALLY A RE-EXCISION. In the pooled follow-up, about 20 PERCENT of excisions had positive margins, and of those only about 20 PERCENT recurred locally - and in the authors' own 42 cases, 32 were INCOMPLETELY excised yet none recurred or progressed, with the single exception of the one malignant tumour. So an incompletely excised benign granular cell tumour can reasonably be observed rather than re-operated, and the decision should turn on the histological grade rather than the margin alone.
- MANAGEMENT is COMPLETE surgical EXCISION with CLEAR MARGINS, which is usually curative for benign lesions; SMALL lesions (under about 1 cm) may be monitored in selected cases, but LARGER lesions and any with worrying features warrant WIDE excision, and a MALIGNANT granular cell tumour requires wide resection and surveillance (with consideration of adjuvant therapy) given its high recurrence/mortality.
- “Granular cell tumour = uncommon, usually BENIGN soft-tissue tumour of SCHWANN-CELL (neural) origin -> S100/SOX10 POSITIVE; cells with abundant GRANULAR eosinophilic cytoplasm. Classic site = TONGUE (also skin/soft tissue/limbs, rarely GI).
- “Overlying pseudoepitheliomatous hyperplasia can MIMIC squamous cell carcinoma on a superficial biopsy - confirm with S100/SOX10 and adequate sampling.
- “RARE MALIGNANT variant = the dangerous one: large (often over ~4-5 cm), rapid growth, necrosis/mitoses -> high recurrence/metastasis/mortality. Treatment = complete excision with clear margins (wide resection + surveillance for large/malignant).
- “Quote the proportions: mean age 45.8, 60% female. Fanburg-Smith grades 72% benign / 17% atypical / 11% malignant, but only ~2.5% METASTASISE - a fourfold over-call, and necrosis + mitoses are the most useful features. Nasser criteria are more conservative (93% benign). ~20% of excisions have positive margins and only ~20% of those recur, so a positive margin alone is not an indication to re-operate.
Small, firm dermal/subcutaneous nodule (classically tongue), S100/SOX10-positive (Schwann-cell origin), with granular eosinophilic cytoplasm - usually benign.
Malignant granular cell tumour - large (often over ~4-5 cm), rapid growth, necrosis/mitoses - high recurrence/metastasis. Adequate sampling (pseudoepitheliomatous hyperplasia mimics SCC).
Features, Histology & The Malignant Variant
The granular cell tumour is an uncommon, usually benign soft-tissue tumour of Schwann-cell (neural) origin - hence S100/SOX10-positive - made of cells with abundant granular eosinophilic (lysosome-rich) cytoplasm. It is typically a small, firm dermal/subcutaneous nodule, classically of the tongue but also the skin/soft tissue of the trunk and limbs and (uncommonly) the viscera. Overlying pseudoepitheliomatous hyperplasia can mimic squamous cell carcinoma on a superficial biopsy. A rare malignant variant - large (often over ~4-5 cm), rapidly growing, with necrosis, increased mitoses/pleomorphism - carries a high risk of recurrence, metastasis and mortality and is the one to identify.
- Benign (the majority)
- Usually small (often under 2 cm)
- Malignant (rare)
- Often large (over ~4-5 cm)
- Benign (the majority)
- Slow
- Malignant (rare)
- Rapid
- Benign (the majority)
- Bland granular cells
- Malignant (rare)
- Necrosis, increased mitoses, pleomorphism, infiltration
- Benign (the majority)
- Cured by complete excision
- Malignant (rare)
- High recurrence/metastasis; significant mortality
- Benign (the majority)
- Complete excision (clear margins)
- Malignant (rare)
- Wide resection + surveillance (+/- adjuvant)
The Granular/Eosinophilic Differential and the Immunoprofile
- The granular/eosinophilic mimics.
- Alveolar soft part sarcoma - crystalline PAS-positive (diastase-resistant) cytoplasmic crystals, TFE3-positive (a caution: GCT can also be TFE3-positive, so use morphology and the wider panel).
- Rhabdomyoma / rhabdomyosarcoma - desmin/myogenin-positive, S100-negative.
- Granular-cell variants of leiomyoma/leiomyosarcoma - SMA/desmin-positive.
- Melanoma - S100/SOX10-positive too (overlap), so distinguish with HMB45/Melan-A and the clinical picture.
- Histiocytic lesions (e.g. reticulohistiocytoma) - CD68-positive but S100-negative.
- The confirming immunoprofile. Conventional GCT is S100-positive, SOX10-positive, CD68-positive (lysosomes), inhibin and calretinin-positive, with PAS-positive diastase-resistant granules, and negative for keratins, desmin, SMA and HMB45/Melan-A - the panel that separates it from the epithelial and muscle mimics.
- The S100-negative variant. A distinct "primitive (non-neural) granular cell tumour" is S100-negative (often ALK-rearranged/ALK-positive) and is NOT of Schwann-cell origin - so do not assume every granular-cell lesion is the S100-positive neural tumour.
Q: What is the differential of a granular-cell lesion and the confirming immunoprofile?
A: Conventional GCT is S100+, SOX10+, CD68+, inhibin/calretinin+, PAS+ (diastase-resistant), and keratin/desmin/SMA/HMB45-negative. Mimics: alveolar soft part sarcoma (PAS crystals, TFE3+ - caution, GCT can be TFE3+ too), rhabdomyoma/RMS (desmin/myogenin+), granular leiomyosarcoma (SMA/desmin+), melanoma (also S100/SOX10+ - use HMB45/Melan-A), and histiocytic lesions (CD68+ but S100-negative). Note the distinct S100-negative "primitive/non-neural granular cell tumour" (often ALK+), not of Schwann-cell origin.
Management
- Diagnosis: adequate biopsy with S100/SOX10 staining (confirm neural origin; avoid over-diagnosing squamous cell carcinoma from pseudoepitheliomatous hyperplasia).
- Treatment (benign): complete surgical excision with clear margins - usually curative; very small lesions may be monitored in selected cases.
- Large/worrying or malignant lesions: wide resection with clear margins; surveillance (and consideration of adjuvant therapy) given the high recurrence/metastasis risk of the malignant variant.
- A positive margin on a benign lesion: not an automatic re-excision. Positive margins occurred in about 20 percent of excisions and only about 20 percent of those recurred; in one series 32 of 42 were incompletely excised without any recurrence. Let the grade, not the margin alone, drive the decision.
- Setting: larger/malignant lesions managed at a specialist sarcoma centre.
The mimics that matter each have a page. The crystalline, TFE3-positive sarcoma to exclude is alveolar soft part sarcoma; the other S100 and SOX10-positive lesion is melanoma, which in the hand and foot presents as subungual melanoma; and the granular-cell variant of a smooth-muscle tumour belongs with leiomyosarcoma. The neural tumours it sits alongside are schwannoma and neurofibroma, and any large or deep lesion should travel the pathway in soft-tissue masses and sarcoma referral.
Although most granular cell tumours are benign, S100-positive Schwann-cell tumours cured by complete excision, two cautions matter. First, the rare malignant variant is genuinely dangerous, carrying a high risk of local recurrence, metastasis and death; the features that should raise concern are a large size (often over about four to five centimetres), rapid growth, necrosis, increased mitotic activity and pleomorphism, and infiltrative margins - so size and growth rate are practical red flags that change the lesion from a simple local excision to a wide resection with surveillance. Second, the epithelium overlying a cutaneous or mucosal granular cell tumour frequently shows pseudoepitheliomatous hyperplasia, which can be mistaken for squamous cell carcinoma on a small or superficial biopsy and lead to over-treatment; adequate sampling and S100/SOX10 confirmation of the neural granular cell tumour prevent this error. Management is therefore complete excision with clear margins, with wide resection and specialist (sarcoma-centre) care for large or malignant lesions.
Grading Malignancy: The Fanburg-Smith Criteria
- The six Fanburg-Smith criteria. Malignancy is graded histologically on six features: (1) necrosis, (2) spindling of the tumour cells, (3) vesicular nuclei with large nucleoli, (4) increased mitotic activity (more than 2 mitoses per 10 high-power fields), (5) a high nuclear-to-cytoplasmic ratio, and (6) pleomorphism.
- The scoring. Meeting none of the six = benign; one or two = atypical; three or more = histologically malignant.
- The caveat, quantified. Histology does not merely predict behaviour imperfectly - it over-calls malignancy by roughly fourfold. Applied to a pooled literature of about 1,500 cases, the Fanburg-Smith criteria classified 72 percent benign, 17 percent atypical and 11 percent malignant, yet true malignancy defined by metastasis occurred in only about 2.5 percent. The alternative Nasser criteria are more conservative, calling 93 percent benign and 7 percent of uncertain malignant potential. Of the six Fanburg-Smith features, necrosis and mitotic activity were the most effective at identifying genuinely aggressive tumours, and the definitive proof of malignancy remains metastasis (regional nodes, lung, bone). Large size (over 4-5 cm) and rapid growth remain the clinical red flags.
Q: How is malignancy in a granular cell tumour graded?
A: By the Fanburg-Smith criteria - six features: necrosis, spindling, vesicular nuclei with large nucleoli, mitoses over 2 per 10 HPF, high N:C ratio, and pleomorphism. None = benign; one or two = atypical; three or more = histologically malignant. The point to add is that this over-calls malignancy: in a pooled series of about 1,500 cases it labelled 11 percent malignant while only 2.5 percent actually metastasised - roughly a fourfold excess. The more conservative Nasser criteria gave 93 percent benign and 7 percent uncertain. Necrosis and mitoses were the most useful individual features, metastasis is the definitive proof, and size over 4-5 cm plus rapid growth are the clinical red flags.
Mnemonics & Memory Aids
GRANULAR
Hook:GRANULAR: Granular cytoplasm, S100 (neuRal), Anywhere (tongue), Nodule, Usually benign (PEH mimics SCC), Large=maLignant, Adequate margins (but grade decides re-excision), Really malignant = metastasis (~2.5%).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A firm subcutaneous nodule is reported as a granular cell tumour. What is its origin, and how do you decide management?”
What it is
- Uncommon, usually benign soft-tissue tumour of Schwann-cell (neural) origin
- S100/SOX10-positive; granular eosinophilic cytoplasm
- Classic site: tongue (also skin/soft tissue/limbs; rarely GI tract)
Diagnostic pitfall
- Overlying pseudoepitheliomatous hyperplasia mimics squamous cell carcinoma
- Confirm with S100/SOX10 and adequate sampling
- Avoid over-treatment as carcinoma
Malignant variant (rare)
- Large (often over ~4-5 cm), rapid growth
- Necrosis and increased mitoses are the most useful features; also pleomorphism, infiltration
- Fanburg-Smith calls 11 percent malignant but only ~2.5 percent metastasise - a fourfold over-call
- Metastasis is the definitive criterion; malignant tumours carry high recurrence and mortality
Management
- Complete surgical excision with clear margins (curative for benign)
- Very small lesions may be monitored; a positive margin on a benign lesion is not an automatic re-excision (~20 percent of those recur)
- Large/malignant: wide resection + surveillance; specialist centre
Evidence & Key Studies
Malignant granular cell tumour - a rare case and review of the literature
- Granular cell tumours are rare, mostly benign soft-tissue neoplasms; only a small proportion (about 8%) occur in the gastrointestinal tract, and the diagnosis is confirmed by S100-positive staining (reflecting the Schwann-cell/neural origin).
- Although rare in some sites, malignant granular cell tumours carry a high risk of mortality and recurrence.
- Small lesions (under about 1 cm) can be monitored, but larger or malignant ones require surgical resection - the case underscores early detection and intervention to prevent severe outcomes.
Granular cell tumor: a study of 42 cases and systematic review of the literature
- 42 institutional cases plus 1,499 cases reviewed to PRISMA guidelines. Mean age at diagnosis 45.8 years (range 6 to 69), 60 percent female; sites in descending frequency were skin and subcutaneous tissue, bronchus, oesophagus, breast, tongue, larynx, pharynx, gingiva, trachea, colon, vulva and hypopharynx.
- By Fanburg-Smith criteria the pooled cases were 72 percent benign, 17 percent atypical and 11 percent malignant; by the more conservative Nasser criteria, 93 percent benign and 7 percent of uncertain malignant potential. True malignancy defined by metastasis occurred in only about 2.5 percent, so the histological criteria over-call malignancy roughly fourfold. Necrosis and mitotic activity were the most effective individual features.
- About 20 percent of excisions had positive margins and about 20 percent of those recurred locally. In the authors' own series, 32 of 42 were incompletely excised yet none recurred or progressed apart from the single clinically malignant tumour, whose patient died 2 years after diagnosis. The follow-up is retrospective and of unstated duration for many pooled cases.
The nature of granular cell tumours (rare, mostly benign soft-tissue neoplasms confirmed by S100 positivity, with only a small proportion in the gastrointestinal tract), the high recurrence/mortality risk of the malignant variant, and the management principle (monitor small lesions, resect larger/malignant ones) come from the cited Usman report. The Schwann-cell (neural) origin with S100/SOX10 positivity, the granular eosinophilic cytology, the classic tongue/skin/soft-tissue sites, the pseudoepitheliomatous-hyperplasia mimic of squamous cell carcinoma, and the malignancy criteria (large size, rapid growth, necrosis, mitoses) with complete/wide excision are standard, well-established teaching. The demographics, the Fanburg-Smith and Nasser classification proportions, the 2.5 percent metastasis figure, the margin and recurrence data and the finding that necrosis and mitoses are the most useful individual criteria come from the Mobarki study, whose follow-up is retrospective and of unstated duration for many of the pooled cases. No randomised trial addresses margin width, re-excision for a positive margin, surveillance interval or adjuvant therapy in this tumour, and no cohort establishes a size threshold at which excision becomes mandatory - so none is quoted here as though settled.