Prevention, Recognition & Management
- Iatrogenic peripheral nerve injuries result from one (or several) of a small set of MECHANISMS: DIRECT LACERATION (by scalpel, drill, saw, K-wire, screw or retractor), TRACTION/STRETCH (limb lengthening, fracture/joint reduction, vigorous retraction), COMPRESSION (a retractor, haematoma, tight cast/dressing or positioning), THERMAL injury (bone cement, diathermy), ISCHAEMIA (tourniquet, vascular injury) and PATIENT-POSITIONING injury - and recognising the mechanism guides both prevention and treatment.
- Each PROCEDURE/region has nerves AT RISK that the surgeon must know: in HIP surgery the SCIATIC nerve (especially its peroneal division - from the posterior approach, lengthening, retractors and dislocation), the FEMORAL nerve (anterior retractors), the SUPERIOR GLUTEAL nerve (abductor-splitting approaches) and the LATERAL FEMORAL CUTANEOUS nerve (anterior approach/positioning) - in total hip arthroplasty the nerves most frequently involved are, in order, the sciatic, femoral, obturator, superior gluteal and lateral femoral cutaneous nerves.
- Other classic at-risk nerves are the ULNAR nerve at the cubital tunnel (elbow surgery and positioning), the COMMON PERONEAL nerve at the FIBULAR NECK (lateral position, leg holders, knee surgery), the RADIAL nerve in humeral shaft fracture/plating, the AXILLARY nerve in shoulder surgery, the SPINAL ACCESSORY nerve in posterior-triangle procedures, and the BRACHIAL PLEXUS from arm abduction/extension during positioning.
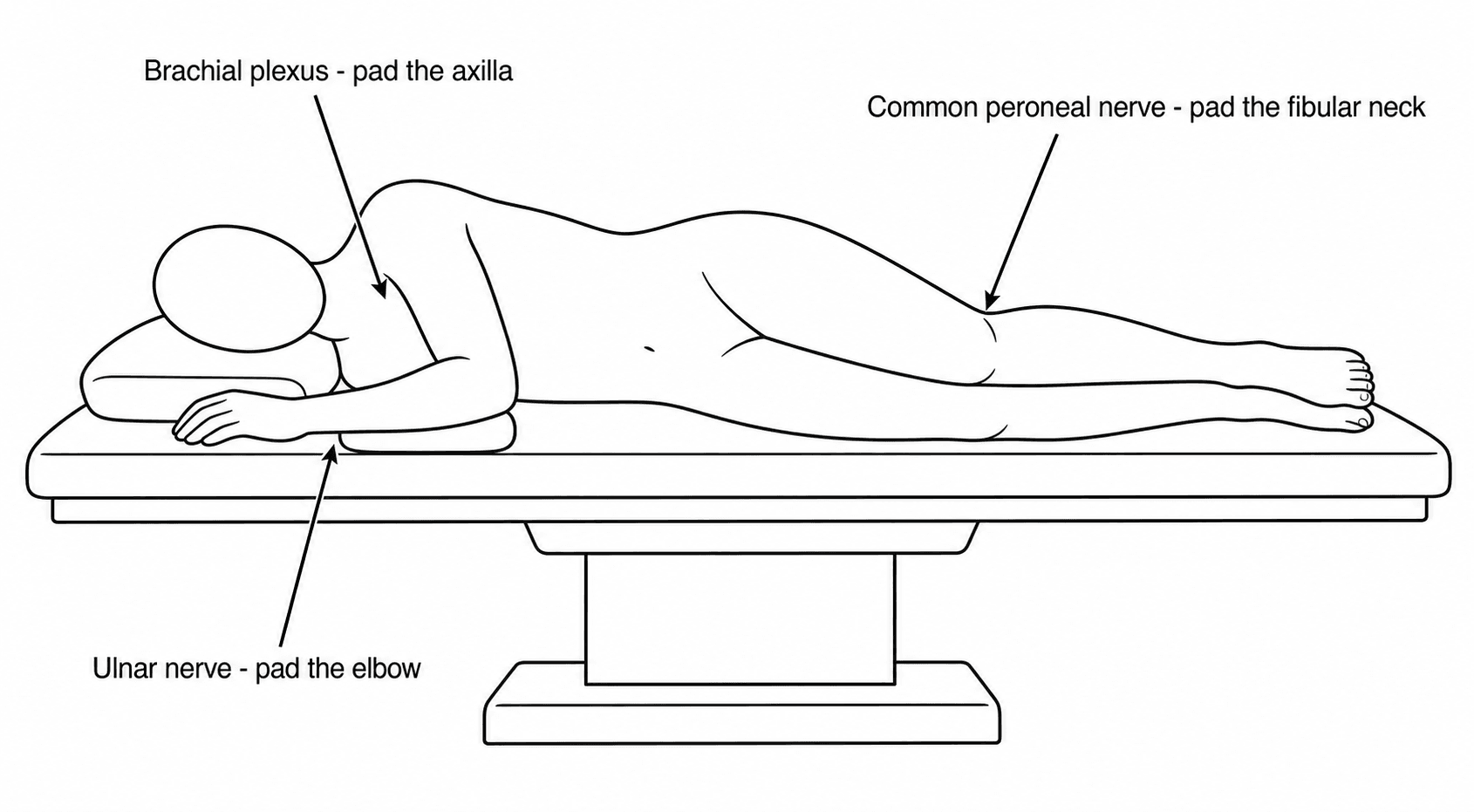
- POSITIONING injuries occur because an anaesthetised, paralysed patient cannot protect their nerves from stretch or sustained compression: classic patterns include brachial-plexus and common-peroneal (dependent leg) injury in lateral decubitus, common-peroneal/sciatic/femoral injury in lithotomy, ulnar/brachial-plexus/eye injury when prone, and PUDENDAL nerve injury from the traction-table perineal post - so correct positioning and PADDING of bony prominences are essential.
- PREVENTION is the priority and rests on knowing the ANATOMY, careful POSITIONING with PADDING of vulnerable nerves/bony prominences, RETRACTOR DISCIPLINE (placement, tension, intermittent release), awareness of LIMB-LENGTH change (excessive lengthening stretches the sciatic nerve), judicious tourniquet use, and protecting nerves during dissection, drilling and implant placement - documenting these precautions is itself important.
- When a postoperative deficit occurs, RECOGNISE and EXAMINE it early (motor/sensory map, distinguish complete from incomplete), exclude REVERSIBLE causes (a tight cast/dressing, a haematoma, a malpositioned limb), and investigate with NERVE CONDUCTION studies/EMG (baseline at around 3 weeks; serial to detect recovery) and imaging (ultrasound/MRI); MANAGEMENT is usually OBSERVATION with rehabilitation for a neurapraxia/incomplete lesion expected to recover, but EXPLORATION/repair is indicated for a suspected transection, a deteriorating or complete lesion with no recovery, or a correctable compressive cause - and, importantly, a nerve injury after a properly performed, documented operation is NOT automatically negligence (it can be an unavoidable adverse event), which is the basis of its medico-legal assessment.
- “Mechanisms of iatrogenic nerve injury: laceration, traction/stretch, compression, thermal, ischaemic, positioning. Know the at-risk nerve for each PROCEDURE.
- “Hip (THA) nerves at risk (in order): sciatic (esp. peroneal division) > femoral > obturator > superior gluteal > LFCN. Also ulnar (elbow), common peroneal (fibular neck), radial (humerus), brachial plexus + pudendal (positioning/traction table).
- “PREVENT (anatomy, positioning + padding, retractor discipline, limb-length awareness, tourniquet care). For a deficit: examine early, exclude reversible causes (cast/haematoma), NCS/EMG; observe most (neurapraxia), explore transection/no-recovery/correctable cause. Not automatically negligence if precautions followed + documented.
Know the at-risk nerve for each procedure; position and pad carefully; retractor discipline; be aware of limb-length change (sciatic stretch); judicious tourniquet. Document the precautions.
Examine early; exclude reversible causes (tight cast/dressing, haematoma, malpositioned limb); NCS/EMG and imaging; observe neurapraxia, explore transection / no-recovery / correctable cause.
Mechanisms & At-Risk Nerves
Iatrogenic nerve injury follows a small set of mechanisms - laceration, traction/stretch, compression, thermal, ischaemic, and positioning - and each procedure has nerves at risk the surgeon must know. In hip surgery: the sciatic (especially its peroneal division), femoral, superior gluteal, obturator and lateral femoral cutaneous nerves. Elsewhere: the ulnar at the cubital tunnel, the common peroneal at the fibular neck, the radial in humeral fracture/plating, the axillary in shoulder surgery, and the brachial plexus (and pudendal on a traction table) from positioning. An anaesthetised patient cannot protect their nerves, so positioning and padding are critical.
- Nerve(s) at risk
- Sciatic (peroneal division) > femoral > obturator > superior gluteal > LFCN
- Mechanism
- Retraction, lengthening, dislocation, positioning
- Nerve(s) at risk
- Ulnar (cubital tunnel)
- Mechanism
- Compression/traction
- Nerve(s) at risk
- Common peroneal (fibular neck)
- Mechanism
- Compression/stretch
- Nerve(s) at risk
- Radial nerve
- Mechanism
- Laceration/traction
- Nerve(s) at risk
- Axillary nerve
- Mechanism
- Traction/laceration
- Nerve(s) at risk
- Brachial plexus, common peroneal, LFCN, ulnar
- Mechanism
- Positioning (stretch/compression)
- Nerve(s) at risk
- Pudendal nerve
- Mechanism
- Compression
Recognition & Management
- Recognise/examine early: map the motor and sensory deficit; distinguish complete from incomplete; note the time of onset (immediate vs delayed).
- Exclude reversible causes immediately: a tight cast/dressing, a compressive haematoma, or a malpositioned limb - release/evacuate/reposition as needed.
- Investigate: nerve conduction studies/EMG (a baseline around 3 weeks; serial studies to detect recovery) and imaging (ultrasound/MRI) where structural injury is suspected.
- Manage: OBSERVE with rehabilitation (splinting, physiotherapy) for a neurapraxia/incomplete lesion expected to recover; EXPLORE/repair for a suspected transection, a complete lesion with no recovery, a deteriorating deficit, or a correctable compressive cause.
- Communicate honestly with the patient and document.
What the timing of onset actually tells you
Whether the deficit was immediate or delayed is not book-keeping - it changes the differential and the urgency.
- What it suggests
- Direct injury during surgery - laceration, suture or screw entrapment, sustained retraction, or a stretch from limb lengthening
- What to do
- The most urgent group. Review the operative detail, image if an implant may be the cause, and consider early return to theatre - a nerve caught under a screw or suture does not improve with waiting
- What it suggests
- Neurapraxia from retraction or positioning; ischaemic from tourniquet
- What to do
- Exclude a correctable cause, then observe with serial examination - most recover
- What it suggests
- An evolving compressive cause - expanding haematoma, swelling under a tight cast or dressing, a limb left in a damaging position on the ward
- What to do
- Treat as reversible until proven otherwise: split the cast, examine for haematoma, reposition. This is the group where delay costs recovery
- What it suggests
- Classic positioning neuropathy, especially ulnar - and the pattern in 62% of ulnar claims
- What to do
- Examine, document, reassure and observe; most are neurapraxias, but exclude a late haematoma
Why the electrodiagnostic study is timed the way it is
"Baseline at around three weeks" has a reason, and a second use that is easy to miss.
Why three weeks: after axonal injury, Wallerian degeneration takes days to develop and fibrillation potentials do not appear on EMG until roughly two to three weeks. A study done in the first few days therefore cannot distinguish a neurapraxia from an axonotmesis, because neither will yet show denervation. Waiting until three weeks lets the study grade the lesion, and a repeat at around three months looks for reinnervation potentials, which appear before clinical recovery is visible.
The second use is medico-legal, and argues for an early study rather than a late one. Precisely because acute denervation takes weeks to appear, abnormalities found in the first few days must pre-date the operation. An early study that shows chronic neurogenic change - or an abnormality in the contralateral limb - documents a pre-existing, often subclinical, neuropathy rather than a surgical injury. That is frequently the single most useful piece of evidence in a claim, and it is unobtainable once three weeks have passed. Where a deficit is significant and the question of pre-existing disease is live, request the study early and bilaterally, and accept that a second study will be needed later to grade the lesion.
When a nerve deficit appears after orthopaedic surgery, the first priority is to examine it promptly and to exclude the immediately reversible causes - a tight cast or dressing, a compartment problem, a compressive haematoma, or a limb left in a damaging position - because these are correctable at the bedside or with prompt return to theatre. Beyond that, the management depends on the likely mechanism and the lesion: most positioning and retraction injuries are neurapraxias that recover with observation, splinting and physiotherapy, and serial nerve conduction studies and EMG (baseline around three weeks) document recovery; but a suspected transection (for example after a sharp instrument near a known nerve), a complete lesion that shows no recovery, a deteriorating deficit, or a clearly correctable compressive cause warrants exploration and repair. Finally, the medico-legal framing matters: a nerve injury after a properly performed and documented operation, with standard preventive measures taken, is not automatically negligence - many such injuries are unavoidable adverse events arising from the interaction of the patient's anatomy and the procedure - so honest communication, careful documentation of the precautions taken, and appropriate management are the basis of good practice.
Grading the Lesion: Seddon, Sunderland & Prognosis
The management section turns on "neurapraxia versus transection" and "observe versus explore" without ever giving the grading framework that underpins it - the Seddon and Sunderland classifications:
- Seddon: neurapraxia → axonotmesis → neurotmesis. Neurapraxia is a conduction block with intact axons (no Wallerian degeneration) - the typical positioning/retraction injury, recovering fully in weeks to a few months. Axonotmesis is axonal disruption with intact connective-tissue sheaths - the axons regrow distally at roughly 1 millimetre per day with variable recovery. Neurotmesis is complete division (axons and sheaths) - no recovery without surgical repair.
- Sunderland I-V refines this: I = neurapraxia; II = axon divided, endoneurium intact (good recovery); III = endoneurium also divided (incomplete recovery, often needs help); IV = only epineurium intact (a neuroma-in-continuity that usually needs resection/grafting); V = complete transection (needs repair). A mixed (VI) pattern can coexist.
- How it drives the decision. A likely Seddon neurapraxia / Sunderland I-II lesion is observed with rehabilitation and serial studies expecting recovery; a Sunderland IV-V / neurotmesis (or a known sharp transection) needs exploration and repair. NCS/EMG help grade it - the absence of denervation and preserved distal conduction points to neurapraxia, while fibrillations/denervation indicate axonal loss. (The cellular pathophysiology - Wallerian degeneration, regeneration - is developed in Nerve Injury & Regeneration.)
Grade it: neurapraxia (Sunderland I - conduction block, recovers in weeks–months) → axonotmesis (Sunderland II-IV - regrows about 1 mm/day) → neurotmesis (Sunderland V - needs repair). Most iatrogenic positioning/retraction lesions are neurapraxias to observe; a Sunderland IV-V / known transection is the one to explore. NCS/EMG distinguishes them (preserved distal conduction = neurapraxia; fibrillations = axonal loss).
Intra-operative Neuromonitoring to Prevent Injury
Limb-lengthening and deformity correction carry a traction risk, and beyond prevention there is a real-time tool for detecting an impending nerve injury during these high-risk cases - intra-operative neuromonitoring (IONM):
- The modalities. Somatosensory evoked potentials (SSEPs) monitor the dorsal-column sensory pathway; transcranial motor evoked potentials (MEPs) monitor the motor tracts/muscles; free-running and triggered EMG detect nerve irritation and (for pedicle screws) breach. The historical Stagnara wake-up test intentionally lightens anaesthesia to confirm voluntary movement.
- Alert criteria. A significant change - classically a 50% fall in SSEP amplitude or a 10% increase in latency, or a marked loss of MEP response - is the alarm that prompts immediate action.
- The corrective response. On an alert: relax the deforming force (reduce the distraction/lengthening or back off a correction), check limb positioning and retractors, restore blood pressure and limb perfusion (raise the mean arterial pressure, release the tourniquet), warm the patient and re-check - the aim is to reverse the insult before it becomes a fixed deficit.
- Where it is used. Spinal deformity correction (the classic indication), complex acetabular/ peri-acetabular and pelvic surgery, limb-lengthening/deformity correction, and some revision or high-risk arthroplasty - it does not replace good anatomy/positioning/retractor discipline but adds a real-time safety net. (Nerve repair techniques for an established transection are covered in Nerve Repairs and Nerve Transfers.)
For high-risk traction cases (spinal deformity, complex pelvic/acetabular, limb-lengthening) use IONM - SSEPs (sensory), transcranial MEPs (motor), free-run/triggered EMG, ± the wake-up test. The classic SSEP alarm is a 50% amplitude drop or 10% latency rise; respond by relaxing the correction, checking position/retractors and raising the blood pressure/perfusion before the change becomes permanent.
Prevention
- Know the anatomy and the at-risk nerve for the approach; protect it during dissection, drilling and implant placement.
- Position and pad: protect the brachial plexus (avoid excessive arm abduction/extension), the ulnar nerve at the elbow, the common peroneal at the fibular neck, and the LFCN; pad bony prominences; check the perineal post on traction tables.
- Retractor discipline: correct placement (e.g. avoid the sciatic posteriorly and femoral anteriorly in hip surgery), minimal tension, intermittent release.
- Limb-length awareness: avoid excessive lengthening (sciatic-nerve stretch) in arthroplasty/deformity correction.
- Tourniquet care: appropriate pressure/time; document positioning and protective measures.
What the Claims Data Actually Show - and Why the Ulnar Nerve Is Different
The evidence that a nerve injury after a properly performed operation is not automatically negligence is stronger, and stranger, than the assertion alone.
In the definitive closed-claims analysis, 670 of 4,183 anaesthesia claims (16%) were for nerve injury, and the distribution was: ulnar nerve 28%, brachial plexus 20%, lumbosacral nerve root 16%, spinal cord 13%. The ulnar nerve is therefore the single commonest perioperative nerve injury, and it behaves unlike the others:
- It occurred predominantly in men (75%).
- Its onset was delayed in 62% of cases - symptoms appearing after the immediate postoperative period, rather than being present on waking.
- It arose overwhelmingly with general anaesthesia (85%), whereas lumbosacral root and spinal cord injuries clustered with regional techniques.
The authors' conclusion is the part that matters and is routinely omitted: they could not recommend new prevention strategies, because the mechanism of most injuries - the ulnar nerve especially - is not apparent. This is the substance behind the medico-legal framing. Ulnar neuropathies occur despite documented padding and correct positioning, the delayed onset is hard to reconcile with simple intra-operative compression, and the male predominance suggests an anatomical predisposition (a thinner or absent protective fat pad and a larger coronoid tubercle) rather than a lapse in care. Padding remains right and must be documented - but it is not a guarantee, and the honest position is that some of these injuries are currently unpreventable.
Positioning: The Specific Rules, With Numbers
"Position and pad" is the instruction everywhere; these are the actual rules an examiner expects, and most of them have a number or a named landmark attached.
- Nerve at risk
- Ulnar nerve at the cubital tunnel
- The rule
- Abduct the arm LESS THAN 90 degrees; keep the forearm SUPINATED or neutral, never pronated - pronation rolls the cubital tunnel onto the board and raises intraneural pressure; pad the elbow
- Nerve at risk
- Brachial plexus (stretch)
- The rule
- Abduction under 90 degrees, avoid external rotation and posterior shoulder sag, and keep the head NEUTRAL - rotating it away stretches the contralateral plexus
- Nerve at risk
- Dependent brachial plexus; dependent common peroneal; dependent ulnar
- The rule
- Place the axillary roll CAUDAL to the axilla, under the chest wall - not in the axilla, where it does the compressing it was meant to prevent; pad the dependent fibular neck and elbow
- Nerve at risk
- Common peroneal at the fibular neck (commonest); sciatic; femoral
- The rule
- Pad the fibular head away from the stirrup; avoid excessive hip flexion, abduction and external rotation; limit duration - and remember well-leg compartment syndrome in prolonged cases
- Nerve at risk
- Lateral femoral cutaneous nerve; ulnar; brachial plexus; eyes
- The rule
- Place bolsters on the chest wall and iliac crests without compressing the ASIS; keep shoulders abducted and elbows flexed under 90 degrees; check the eyes are free
- Nerve at risk
- Pudendal nerve
- The rule
- A well-padded, adequately sized perineal post, minimum effective traction, and limit traction time
- Nerve at risk
- Brachial plexus (compression)
- The rule
- Braces over the acromioclavicular joints, not medially over the plexus - or avoid braces altogether in favour of a non-slip mattress
Two habits matter as much as the initial set-up: re-check the position after every change - draping, table tilt, repositioning for imaging - because a limb that was safe at the start may not be at hour three, and record what was padded, since documentation is the only evidence that the standard was met.
The patient factors that raise risk are worth knowing too, because they identify who to be most careful with: diabetes and pre-existing subclinical neuropathy (a "double crush" susceptibility), extremes of body habitus at either end, male sex for the ulnar nerve, prolonged operative time, and intra-operative hypotension and hypothermia.
Mnemonics & Memory Aids
PROTECT
Hook:PROTECT: Position/Pad, Retractor discipline, Overlengthening avoided, Tourniquet/Thermal + anatomy, Examine early, Correct reversible, Test + observe/explore.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient wakes from a total hip arthroplasty with a foot drop. How do you approach this?”
Mechanisms
- Laceration, traction/stretch, compression, thermal, ischaemic
- Patient-positioning (anaesthetised patient can't protect nerves)
- Recognising the mechanism guides prevention + treatment
At-risk nerves
- THA: sciatic (peroneal division) > femoral > obturator > superior gluteal > LFCN
- Ulnar (elbow/cubital tunnel), common peroneal (fibular neck), radial (humerus), axillary (shoulder)
- Positioning: brachial plexus, common peroneal, LFCN, ulnar; pudendal (traction post)
Prevention
- Know anatomy/at-risk nerve; position + pad; retractor discipline
- Avoid excessive limb lengthening (sciatic stretch); judicious tourniquet
- Document positioning and protective measures
Recognition & management
- Examine early (complete vs incomplete); exclude reversible (cast/dressing, haematoma, malposition)
- NCS/EMG (baseline ~3 weeks, serial); imaging if structural injury suspected
- Observe neurapraxia (rehab/AFO); explore transection/no-recovery/correctable cause; not automatically negligence if precautions documented
Evidence & Key Studies
Nerve injury after total hip arthroplasty: aetiology, prevention and medico-legal considerations
- Nerve injuries in total hip arthroplasty are rare but clinically and medico-legally significant, resulting from complex interactions between the patient's pathophysiology, the technical aspects of surgery and the individual response - often rendering them not entirely avoidable.
- The nerves most frequently involved across the surgical phases are, in order, the sciatic, femoral, obturator, superior gluteal and lateral femoral cutaneous nerves; risk factors include the approach, intra-operative positioning, retraction/ligation/dissection, limb-length change and local haematoma/infection.
- Adverse outcomes should not automatically be interpreted as surgical negligence when standard care and clinical risk-management protocols have been followed and documented - a risk-prevention and -management strategy is the first step in patient safety.
Perioperative peripheral nerve injury from a fixation device - the role of positioning
- A perioperative peripheral nerve injury (anterior cutaneous nerve entrapment) was caused by a fixation device during bipolar hip arthroplasty, illustrating positioning/device-related iatrogenic nerve injury.
- Maintaining patients in the appropriate position during the operation is important to prevent perioperative peripheral nerve injury.
- Recognition of the syndrome (e.g. a positive Carnett's sign for an abdominal-wall source) is needed to diagnose iatrogenic nerve injury postoperatively.
Nerve injury associated with anesthesia: a closed claims analysis
- 670 of 4,183 claims (16%) in the ASA Closed Claims Database were for anaesthesia-related nerve injury; the commonest sites were the ULNAR NERVE (28%), brachial plexus (20%), lumbosacral nerve root (16%) and spinal cord (13%).
- Ulnar injuries occurred predominantly in MEN (75%), overwhelmingly under general anaesthesia (85%), and had a DELAYED onset of symptoms in 62% - a pattern unlike the other nerve injuries.
- The authors could not recommend new prevention strategies, because the mechanism of most injuries - the ulnar nerve in particular - is not apparent.
The order of nerves most frequently injured in total hip arthroplasty (sciatic, femoral, obturator, superior gluteal, lateral femoral cutaneous), the risk factors (approach, positioning, retraction, limb-length change, haematoma), and the medico-legal principle that such injuries are not automatically negligence when standard precautions are followed and documented come from the cited Bianco Prevot review; the role of intra-operative positioning/device contact in perioperative nerve injury from the cited Miyamatsu report. The full list of mechanisms, the at-risk nerves for other procedures/positions, and the recognition-and-management pathway (exclude reversible causes, NCS/EMG, observe vs explore) are standard, well-established teaching. The closed-claims distribution, the male predominance and delayed onset of ulnar injury, and the finding that the mechanism is not apparent come from the cited Cheney analysis. (See also Tourniquet Use, Compartment Syndrome, Nerve Injury & Regeneration, Nerve Repairs, Ulnar Nerve Anatomy and Meralgia Paraesthetica.)