Softening of the Patellar Articular Cartilage
- Chondromalacia patellae literally means softening (Greek malakia) of the cartilage (chondros) of the patella - specifically the articular cartilage on the posterior surface of the patella - and it may progress through FIBRILLATION, FISSURING and EROSION; it is one of the most frequently encountered causes of knee pain in young people, classically young adults and often women.
- It is a DESCRIPTIVE term for a cartilage finding rather than a single pathophysiological diagnosis, and it overlaps with but is not synonymous with PATELLOFEMORAL PAIN syndrome - many patients with anterior knee pain have normal cartilage, and conversely chondromalacic change can be found without symptoms - so the diagnosis should not be assumed from pain alone, and 'idiopathic' chondromalacia is that arising without a clear anatomical cause.
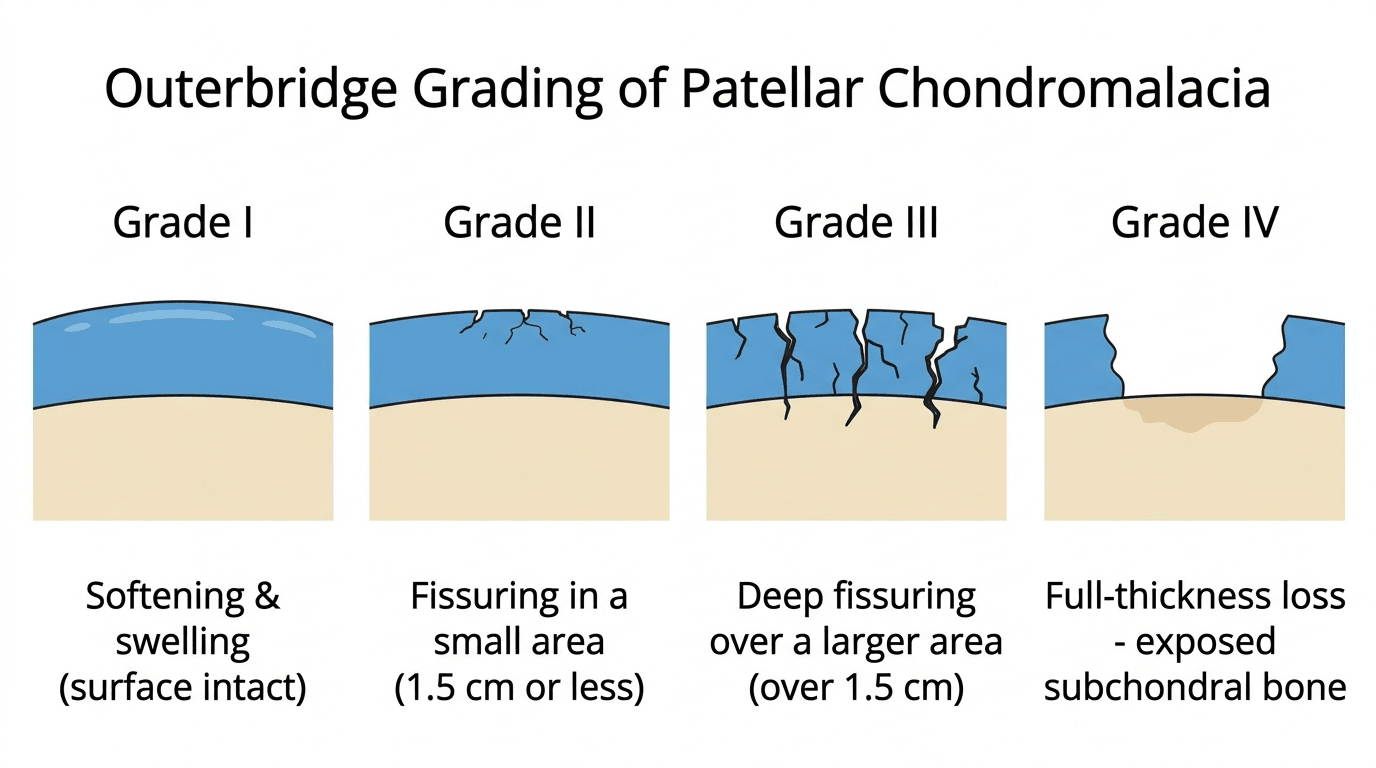
- The ARTHROSCOPIC grading is the OUTERBRIDGE classification: grade I, softening and swelling of the cartilage; grade II, fragmentation and fissuring in an area of 1.3 cm or less; grade III, fragmentation and fissuring in an area larger than 1.3 cm; and grade IV, cartilage erosion down to exposed subchondral bone.
- CLINICALLY there is anterior or retropatellar knee pain that is typically worse with stair climbing/descending, squatting, kneeling and prolonged sitting (the 'theatre sign'), sometimes with crepitus; examination may show a positive CLARKE'S sign (pain on patellar compression during quadriceps contraction - the patellar grind test) and patellofemoral tenderness, and contributing factors such as maltracking should be sought.
- IMAGING is usually for exclusion and grading: radiographs (including a skyline/Merchant view) assess patellofemoral alignment and exclude other causes, while MRI can show cartilage signal change and grade the lesion; arthroscopy provides the definitive (Outerbridge) grading but is not required to make the clinical diagnosis.
- MANAGEMENT is predominantly CONSERVATIVE: activity modification, analgesia/NSAIDs, and a structured rehabilitation programme emphasising QUADRICEPS (especially VMO) and HIP/core strengthening, stretching and patellar taping/bracing; intra-articular options (e.g. hyaluronic acid, and platelet-rich plasma, which has shown benefit over physiotherapy alone in some studies, especially in younger patients) and arthroscopic chondroplasty or cartilage procedures are reserved for refractory cases.
- “Chondromalacia patellae = SOFTENING of patellar articular cartilage (-> fibrillation -> fissuring -> erosion); common anterior knee pain in young adults (often women).
- “DESCRIPTIVE term (a cartilage finding), overlaps with but is not the same as patellofemoral pain; graded arthroscopically by OUTERBRIDGE (I-IV; IV = exposed bone).
- “Anterior knee pain worse on stairs/squatting/prolonged sitting; positive Clarke's sign. Management CONSERVATIVE-first (VMO/hip rehab; injections/chondroplasty if refractory).
Softening of the patellar articular cartilage (progressing to fibrillation/fissuring/erosion); common anterior knee pain in young adults. Graded by Outerbridge (I-IV).
A descriptive term - overlaps with but is not the same as patellofemoral pain (which can occur with normal cartilage). Manage conservatively first.
Definition, Grading & Assessment
Chondromalacia patellae is softening of the articular cartilage on the posterior surface of the patella (Greek: chondros = cartilage, malakia = softening), which may progress to fibrillation, fissuring and erosion, and it is a common cause of anterior knee pain in young adults (often women). It is a descriptive cartilage finding rather than a single disease, overlapping with but not identical to patellofemoral pain (which can occur with normal cartilage). Cartilage change is graded arthroscopically by the Outerbridge classification (I softening/swelling; II fissuring in an area 1.3 cm or less; III fissuring in a larger area; IV exposed subchondral bone). Clinically there is anterior/retropatellar pain worse on stairs, squatting and prolonged sitting, with a positive Clarke's (patellar grind) sign; radiographs (with a skyline view) and MRI assess alignment and grade, but arthroscopy gives the definitive grading.
- Cartilage appearance
- Softening and swelling of the cartilage
- Cartilage appearance
- Fragmentation/fissuring in an area 1.3 cm or less
- Cartilage appearance
- Fragmentation/fissuring in an area larger than 1.3 cm
- Cartilage appearance
- Erosion of cartilage down to exposed subchondral bone
Why the Cartilage Softens: Aetiology and Idiopathic vs Secondary
Be ready to give the mechanism of softening and to separate idiopathic from secondary chondromalacia, because a correctable driver changes management.
Softening is the morphological expression of cartilage that is mechanically overloaded or intrinsically vulnerable: early matrix breakdown (proteoglycan loss, collagen-network disruption, increased water content) that progresses to fibrillation -> fissuring -> erosion - the same early-degeneration cascade detailed in Articular Cartilage Structure.
- Idiopathic: softening without a clear anatomical cause (the body's term), typically young adults/women, attributed to subtle overload/patellofemoral mechanics.
- Secondary (a definable driver): patellar maltracking / lateral overload, patellar instability (recurrent subluxation/dislocation shearing the cartilage), direct trauma (dashboard injury, fall on the flexed knee), prolonged immobilisation, and malalignment (Q-angle, weak hip abductors).
Chondromalacia is overloaded/vulnerable cartilage undergoing early matrix breakdown; always separate idiopathic from secondary (maltracking, instability, trauma, immobilisation) - because a correctable driver (especially maltracking/instability) is what changes management beyond rehab.
The Differential of Anterior Knee Pain in the Young Adult
The cartilage is only one possible source of anterior knee pain in a young adult, so the wider differential matters and the pain should be localised before it is attributed to the patellar cartilage.
- Discriminating clue
- Retropatellar pain, worse on stairs, squatting and prolonged sitting
- What it means for management
- Structured rehabilitation - hip abductor and quadriceps strengthening - not arthroscopy
- Discriminating clue
- Inferior-pole tenderness, pain on loading and jumping
- What it means for management
- Progressive tendon loading, not rest - the tendon needs a stimulus to remodel
- Discriminating clue
- Superficial fluctuant ANTERIOR swelling over the patella - the problem is in front of the bone, not behind it
- What it means for management
- Rest, compression and kneeling avoidance; exclude infection before injecting anything
- Discriminating clue
- Apprehension, a history of subluxation or dislocation, J-sign on active extension
- What it means for management
- Assess trochlear dysplasia, patella alta and TT-TG distance - this group may genuinely need surgery, unlike the rest of the table
- Discriminating clue
- Medial snapping band, or infrapatellar pain on hyperextension
- What it means for management
- Rehabilitation and activity modification first; excision or fat-pad debridement only for genuinely refractory, well-localised cases
- Discriminating clue
- Superolateral tenderness; hip examination and age; tibial-tubercle or inferior-pole apophyseal pain
- What it means for management
- Do not miss the hip: ALWAYS examine it in an adolescent with knee pain, because a SUFE presents with referred knee pain and a normal-looking knee
Management
- Do not lean on Clarke's sign. The patellar grind test is quoted throughout as the examination finding, but it is poorly specific: pressing the patella into the trochlea and asking a patient to contract the quadriceps is uncomfortable in a substantial proportion of normal knees, so a positive test in isolation confirms very little and a negative one does not exclude the diagnosis. Use it as one part of a pattern - with the site of tenderness, the loading history and the assessment of tracking and proximal control - rather than as the diagnostic test.
- Conservative first: activity modification, analgesia/NSAIDs, and a structured rehabilitation programme emphasising quadriceps (VMO) and hip/core strengthening, stretching, and patellar taping/bracing.
- Address contributors: patellar maltracking, weak hip abductors/external rotators, tight lateral structures and biomechanical factors.
- Injections: intra-articular hyaluronic acid and platelet-rich plasma (which has shown benefit over physiotherapy alone in some studies, particularly in younger patients) for selected refractory cases.
- Surgery: arthroscopic chondroplasty/debridement or cartilage-restoration procedures are reserved for refractory, high-grade lesions, with realignment only for a demonstrated maltracking cause - because the pain often does not correlate well with the cartilage grade.
The key judgement in chondromalacia patellae is to remember that it is a descriptive cartilage finding, not a one-to-one explanation for a patient's pain: anterior knee pain frequently occurs with normal cartilage (patellofemoral pain), and chondromalacic change is sometimes found incidentally without symptoms, so the clinical picture and contributing biomechanical factors must be assessed rather than attributing all pain to the cartilage and rushing to surgery. Management is conservative first - quadriceps (VMO) and hip strengthening, activity modification and load management - with injections and arthroscopic chondroplasty or cartilage procedures reserved for genuinely refractory cases, and realignment surgery only for a demonstrated maltracking cause. Over-treating the radiological or arthroscopic grade rather than the patient is the pitfall to avoid.
Why the Pain Does Not Match the Cartilage
Pain correlates poorly with the cartilage grade, and the reason is a basic-science answer worth having ready.
Articular cartilage is aneural. It contains no nerve endings, so a fibrillated or fissured cartilage surface cannot itself generate pain. Whatever hurts in this condition is not the lesion the arthroscope is looking at. The actual nociceptive sources around the patellofemoral joint are:
- Subchondral bone, richly innervated, loaded increasingly as the overlying cartilage thins and loses its load-distributing function - the likeliest source in high-grade disease, and the reason bone marrow oedema on MRI tracks symptoms better than the cartilage signal does.
- The lateral retinaculum, which contains free nerve endings and shows neural changes in chronic anterior knee pain, particularly where it is tight.
- The synovium and the infrapatellar (Hoffa) fat pad, both densely innervated and readily irritated.
- The subchondral plate and peripatellar soft tissues more generally, plus central sensitisation in long-standing cases.
Three consequences follow, and they are the practical payoff:
- A patient can have Outerbridge III change and no pain, because the cartilage lesion is silent until it changes the loading of something innervated.
- A patient can have severe pain with pristine cartilage - which is patellofemoral pain, and is why arthroscopy for anterior knee pain alone so often finds nothing to explain the symptoms.
- Chondroplasty treats the lesion, not the pain generator, which is precisely why debriding a chondromalacic patella for pain gives such unreliable results. Modifying load - the loading of the subchondral bone and the tension in the retinaculum - is what actually changes symptoms, and that is a rehabilitation problem far more often than a surgical one.
The loads involved, and why the symptoms take the shape they do
The patella carries the thickest articular cartilage in the body, which is a clue to the forces it handles. The patellofemoral joint reaction force rises steeply with knee flexion under load - modest in level walking, several times body weight on stairs, and higher still in a deep squat - because the quadriceps tension and the angle of the extensor mechanism both increase.
That single fact explains the whole symptom pattern the page describes: pain descending stairs (eccentric quadriceps loading at flexion) rather than on the flat, pain squatting and kneeling, and the theatre sign - discomfort after prolonged sitting with the knee flexed, where the patella is held loaded against the trochlea without the relief of movement. It also explains why rehabilitation is prescribed in a pain-free arc and why closed-chain exercise near extension is tolerated when deep flexion loading is not.
Mnemonics & Memory Aids
SOFTEN
Hook:SOFTEN: Softening, Outerbridge grades, Fibrillation/fissuring, Theatre-sign pain (Clarke's), Exercise rehab, Not equal to patellofemoral pain.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is chondromalacia patellae and how is it graded?”
“How would you manage a young adult with chondromalacia patellae?”
Definition
- Softening of the patellar articular cartilage (chondros + malakia)
- Progresses: softening -> fibrillation -> fissuring -> erosion
- Common anterior knee pain in young adults (often women); a descriptive term
Grading & assessment
- Outerbridge: I softening, II fissuring 1.3 cm or less, III fissuring over 1.3 cm, IV exposed bone
- Pain worse on stairs/squatting/prolonged sitting (theatre sign); positive Clarke's sign
- Radiographs (skyline view) + MRI for alignment/grade; arthroscopy = definitive grade
Key concept
- Overlaps with but is not the same as patellofemoral pain (can occur with normal cartilage)
- Pain does not correlate well with cartilage grade
- Can be an incidental finding
Management
- Conservative first: activity modification, analgesia, VMO/hip/core rehab, taping/bracing
- Injections (HA, PRP) for refractory cases
- Chondroplasty/cartilage procedures for refractory/high-grade; realignment only for maltracking
Evidence & Key Studies
Chondromalacia patellae (definition and natural history)
- Chondromalacia patellae is softening of the articular cartilage on the posterior surface of the patella (chondros = cartilage, malakia = softening).
- It may eventually lead to fibrillation, fissuring and erosion of the cartilage.
- It is one of the most frequently encountered causes of knee pain in young people.
PRP and hyaluronic acid for anterior knee pain due to chondromalacia patellae
- Chondromalacia patellae describes softening of patellar articular cartilage and remains a general descriptive term not tied to a single pathophysiological mechanism; it commonly causes anterior knee pain in young adults (often women).
- In patients with anterior knee pain and a positive Clarke's sign without altered patellofemoral anatomy, platelet-rich plasma (with hyaluronic acid) improved VAS and Kujala scores significantly more than physiotherapy alone at 3 and 6 months.
- Younger patients benefited more from the injection treatment.
The definition (softening of patellar articular cartilage progressing to fibrillation, fissuring and erosion) and its frequency as a cause of knee pain in young people come from the cited Gordon article; the characterisation of chondromalacia as a general descriptive term, the association with anterior knee pain and a positive Clarke's sign, and the benefit of PRP/hyaluronic acid over physiotherapy alone (particularly in younger patients) from the cited Ostojic study. The Outerbridge arthroscopic grading, the overlap with patellofemoral pain, and the conservative-first rehabilitation pathway are standard, well-established teaching. The Outerbridge grade II/III cutoff is the ORIGINAL half an inch (about 1.3 cm), not 1.5 cm - see Articular Cartilage Injuries. The aneural nature of cartilage and the peripatellar pain sources, and the patellofemoral loading that shapes the symptom pattern, are standard basic-science teaching. (See also Patellofemoral Instability, Lateral Patellar Compression Syndrome, Articular Cartilage Injuries and Cartilage Healing & Repair.)