Excessive Lateral Pressure Syndrome (ELPS)
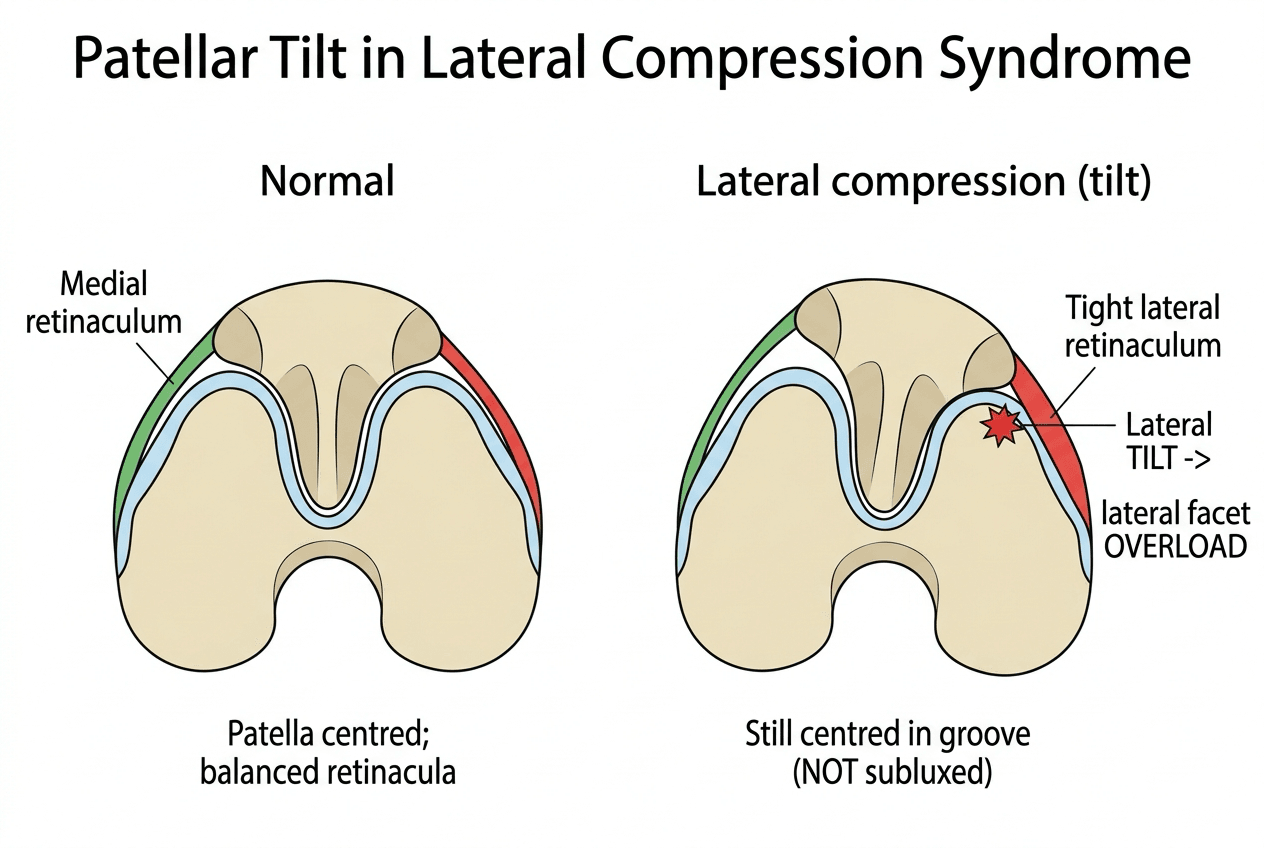
- Lateral patellar compression syndrome, also called excessive lateral pressure syndrome (ELPS), is caused by a TIGHT LATERAL RETINACULUM that TILTS the patella laterally and concentrates load on the LATERAL patellofemoral facet, producing excessive lateral pressure, anterior knee pain and, over time, lateral facet cartilage degeneration - and the defining point is that the patella is TILTED, not subluxing or dislocating, so this is a problem of PRESSURE/tilt, NOT of instability.
- The hallmark clinical sign is a positive PATELLAR TILT TEST: with the knee extended and quadriceps relaxed, the examiner tries to lift (evert) the lateral edge of the patella, and in ELPS the tight lateral retinaculum prevents the lateral patella being everted past the horizontal/neutral; there is also lateral patellofemoral tenderness and anterior knee pain worse with activity and prolonged sitting.
- AXIAL (skyline / Merchant) radiographs are the key imaging, showing an abnormal PATELLAR TILT ANGLE and a reduced/negative LATERAL PATELLOFEMORAL ANGLE (the patella tilted laterally), and CT or MRI confirm lateral tilt WITHOUT subluxation and assess the lateral facet cartilage (and exclude maltracking from trochlear dysplasia or a high TT-TG that would change management).
- MANAGEMENT is CONSERVATIVE first: activity modification and analgesia, plus a rehabilitation programme that STRETCHES the tight lateral structures (lateral retinaculum, iliotibial band) and STRENGTHENS the vastus medialis obliquus and the hip abductors/external rotators, with patellar taping/bracing to medialise/de-rotate the patella.
- For REFRACTORY, genuine ELPS (a tight lateral retinaculum with tilt and no instability), an ARTHROSCOPIC LATERAL RETINACULAR RELEASE - sometimes combined with a lateral patelloplasty - is an effective minimally invasive option that corrects the tilt, relieves pain and improves function (with outcomes worse when the lateral facet already has high-grade cartilage damage).
- A CRITICAL caveat is that lateral retinacular release is for TILT/compression, NOT for patellar INSTABILITY: a randomised trial found NO benefit from adding a routine lateral release to MPFL reconstruction in recurrent patellar dislocation, and an inappropriate or over-aggressive lateral release can actually WORSEN instability (medial patellar subluxation/iatrogenic instability) - so the indication must be a tight lateral retinaculum with tilt, not a loose, unstable patella.
- “ELPS = tight LATERAL RETINACULUM -> patellar TILT + excessive lateral pressure -> anterior knee pain (TILT, not instability).
- “Positive PATELLAR TILT TEST (can't evert the lateral patella past neutral); skyline radiographs show abnormal patellar tilt angle / lateral patellofemoral angle.
- “Conservative first (stretch lateral structures, VMO/hip). Lateral retinacular release for refractory TILT/ELPS - NOT for instability (no benefit added to MPFL recon; can worsen instability).
A tight lateral retinaculum tilts the patella laterally - excessive lateral pressure and anterior knee pain - with the patella tilted, not subluxing (NOT instability).
Lateral retinacular release is for tilt/ELPS, NOT for instability - it adds no benefit to MPFL reconstruction and can worsen instability if misapplied.
Mechanism, Diagnosis & Imaging
Lateral patellar compression syndrome (excessive lateral pressure syndrome, ELPS) is caused by a tight lateral retinaculum that tilts the patella laterally and concentrates load on the lateral facet - excessive lateral pressure - causing anterior knee pain and, over time, lateral facet cartilage wear; crucially the patella is tilted, not subluxing (this is not instability). The hallmark sign is a positive patellar tilt test (the tight lateral retinaculum prevents everting the lateral patella past neutral), with lateral patellofemoral tenderness. Axial (skyline/Merchant) radiographs show an abnormal patellar tilt angle and lateral patellofemoral angle, and CT/MRI confirm tilt without subluxation and assess the lateral facet cartilage (and exclude trochlear dysplasia or a high TT-TG that would change management).
Proving It Is Tight and Not Loose at the Bedside
Treatment turns entirely on separating a tight patella from an unstable one, and the tilt test alone does not do it - a patella can be both tilted and lax. Two further examinations settle it, and they take seconds.
The patellar glide test quantifies the restraints in quadrants. With the knee flexed to about 20 to 30 degrees and the quadriceps relaxed, divide the patella into four longitudinal quadrants and translate it medially, then laterally, recording how many quadrants of its own width it moves:
- Medial glide of less than one quadrant means the lateral structures are tight - the finding that supports excessive lateral pressure, and the one a release or lengthening is designed to correct. (Normal is around two quadrants.)
- Lateral glide of three quadrants or more means the medial restraints are incompetent, and four quadrants is a frank dislocation. This is instability, and it is the finding that makes a lateral release the wrong operation.
The two can coexist, which is exactly the trap: a tight lateral retinaculum in a patient who also has a deficient MPFL. Releasing that patella removes what little lateral checkrein remained.
Apprehension should be absent. Pushing the patella laterally with the knee near extension provokes a protective, alarmed response in a patient whose patella has dislocated - and produces nothing in excessive lateral pressure, where the complaint is pain from compression rather than fear of the patella leaving the groove. A positive apprehension sign points away from this diagnosis and towards instability, and is the fastest single discriminator available. Where it is positive, or lateral glide is excessive, reach for the instability work-up - trochlear dysplasia, TT-TG distance, patellar height and MPFL competence - covered in Patellofemoral Instability and MPFL Injury.
Management
- Conservative first: activity modification and analgesia, plus rehabilitation that STRETCHES the tight lateral structures (lateral retinaculum, iliotibial band) and STRENGTHENS the VMO and hip abductors/external rotators; patellar taping/bracing to medialise the patella.
- Confirm true ELPS: a tight lateral retinaculum with tilt and NO instability, with abnormal tilt angles on skyline imaging.
- Lateral retinacular release (arthroscopic, sometimes with lateral patelloplasty) for refractory true ELPS - it corrects the tilt, relieves pain and improves function; outcomes are poorer with high-grade lateral facet cartilage damage.
- Do NOT release for instability: lateral release adds no benefit to MPFL reconstruction in recurrent dislocation and can WORSEN instability (medial subluxation) if misapplied.
The single most important judgement in lateral patellar compression syndrome is to confirm that the problem is TILT from a tight lateral retinaculum and NOT instability, because lateral retinacular release is the right operation for the former and the wrong one for the latter. A randomised trial showed no benefit from adding a routine lateral release to MPFL reconstruction in recurrent patellar dislocation, and an inappropriate or over-aggressive lateral release in an unstable or already-lax patella can worsen instability and even cause medial patellar subluxation. So reserve lateral release for the patient with a genuinely tight lateral retinaculum, a positive tilt test and abnormal tilt angles on skyline imaging, after failed conservative management - and treat instability with the appropriate medial-sided and bony procedures instead.
The Axial Radiographic Angles (Defining Tilt vs Subluxation)
The diagnosis leans on the "patellar tilt angle" and "lateral patellofemoral angle" - the examinable detail is knowing what each measures, on an axial (Merchant/Laurin skyline or axial CT/MRI) view with the knee in early flexion:
- Lateral patellofemoral angle (Laurin). The angle between a line across the anterior aspects of the two femoral condyles and a line along the lateral patellar facet. Normally this angle opens laterally; in excessive lateral pressure the lateral tilt makes the lines become parallel or the angle open medially - the classic Laurin sign of patellar tilt.
- Patellar tilt angle. The angle between the transverse (equatorial) axis of the patella and the posterior femoral condylar line; it increases as the patella tilts laterally and is commonly cited as abnormal beyond about twenty degrees - a direct measure of how tilted the patella sits in the trochlea.
- Separating tilt from subluxation. Tilt is a rotational malposition (the above angles), whereas subluxation is translational - measured by the congruence angle (Merchant), which locates the patellar apex relative to the bisector of the sulcus angle. ELPS shows tilt with a normal congruence angle (no subluxation); an abnormal congruence angle points to instability/maltracking instead.
Tilt = rotation (lateral patellofemoral angle opening medially/parallel; raised patellar tilt angle); subluxation = translation (abnormal congruence angle on the Merchant view). ELPS is tilt with a normal congruence angle. If the congruence angle is abnormal you are dealing with instability/maltracking - and the patellar height (Insall-Salvati/Caton-Deschamps) and trochlear depth (sulcus angle) are checked alongside, and are developed in Patellar Height Abnormalities and Patellofemoral Instability.
Lateral Release vs Lengthening: Technique and Complications
The operative detail behind the release, and the reason many surgeons now lengthen instead:
- Lateral retinacular release. Division of the tight lateral retinaculum (the superficial oblique and deep transverse fibres) from around the superior pole down toward the inferior pole/tibial-tubercle level - done arthroscopically (inside-out) or open - so the tilted patella can be everted and re-centred. Lateral patelloplasty (as in the cited Wang series) adds contouring/chondral management of the worn lateral facet at the same sitting.
- The shift to lateral retinacular LENGTHENING. Because a complete release sacrifices the lateral restraint, many now prefer a controlled z-/step-cut lengthening of the retinaculum: it relieves the tight lateral tether and corrects tilt while preserving a lateral checkrein, reducing the risk of iatrogenic medial instability - particularly when there is any doubt about laxity.
- Complications. Haemarthrosis is the commonest (bleeding from the lateral superior genicular vessels); the feared specific complication is iatrogenic MEDIAL patellar instability/subluxation from over-release (exactly why release is wrong for an unstable patella); also quadriceps inhibition/weakness and persistent pain when the lateral facet cartilage is already high-grade (poorer outcomes, per Wang).
Release divides the lateral retinaculum; lengthening (z-plasty) achieves the same de-tilting while keeping a lateral restraint and is increasingly preferred to avoid the classic complication - iatrogenic medial subluxation from over-release. Commonest complication overall is haemarthrosis; outcomes are worse with established lateral-facet chondral damage. Reserve either for a genuinely tight, tilted, stable patella.
Mnemonics & Memory Aids
TILT
Hook:TILT: Tight lateral retinaculum, Increased lateral pressure, Lateral tilt (not instability), Tilt test positive (release only for refractory tilt).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is excessive lateral pressure syndrome and how do you diagnose it?”
“How would you manage ELPS, and what is the role of lateral retinacular release?”
Mechanism
- Tight lateral retinaculum tilts the patella laterally
- Excessive lateral facet pressure -> anterior knee pain + lateral facet wear
- Patella TILTED, not subluxing (NOT instability)
Diagnosis
- Positive patellar tilt test (can't evert lateral patella past neutral)
- Lateral patellofemoral tenderness; pain with activity/prolonged sitting
- Skyline radiographs: abnormal patellar tilt angle / lateral patellofemoral angle; CT/MRI confirm tilt without subluxation
Conservative management
- Activity modification, analgesia
- Stretch lateral structures (retinaculum, IT band); strengthen VMO/hip
- Patellar taping/bracing to medialise
Surgery
- Lateral retinacular release (+/- patelloplasty) for refractory true ELPS
- Worse outcomes with high-grade lateral facet cartilage damage
- NOT for instability (no benefit with MPFL recon; can worsen instability)
Evidence & Key Studies
Arthroscopic lateral retinacular release with lateral patelloplasty for excessive lateral pressure syndrome
- In 73 patients (88 knees) with ELPS, arthroscopic lateral retinacular release combined with lateral patelloplasty significantly reduced pain (VAS) and improved Kujala and Lysholm scores, patella medial pushing distance, patellar tilt angle and lateral patellofemoral angle.
- Outcomes were worse with a higher lateral patella Outerbridge cartilage grade at follow-up.
- The technique effectively corrects the patellar force-line/tilt abnormality with few complications, supporting lateral release for true ELPS.
Lateral retinacular release is not recommended routinely with MPFL reconstruction for instability
- In a randomised trial of recurrent patellar dislocation, adding an arthroscopic lateral retinacular release to MPFL reconstruction produced no significant difference in subjective IKDC score or patellar tilt versus isolated MPFL reconstruction.
- There is no indication for a systematic lateral retinacular release in association with MPFL reconstruction for recurrent dislocation.
- This underlines that lateral release addresses tilt/compression, not instability.
The efficacy of arthroscopic lateral retinacular release (with lateral patelloplasty) for true ELPS - improving pain, function and the patellar tilt/lateral patellofemoral angles, with worse outcomes at higher lateral-facet cartilage grades - comes from the cited Wang study; the evidence that a routine lateral release adds no benefit to MPFL reconstruction for recurrent dislocation (underlining that release is for tilt, not instability) from the cited Malatray randomised trial. The tight-lateral-retinaculum mechanism, the patellar tilt test, the glide-test quadrants, the absent apprehension sign, the skyline radiographic angles and the conservative-first rehabilitation are standard, well-established teaching. (See also Patellofemoral Instability, MPFL Injury, Chondromalacia Patellae for the wider anterior knee pain differential, and Patellar Height Abnormalities.)