Fracture Between a Hip and a Knee Implant
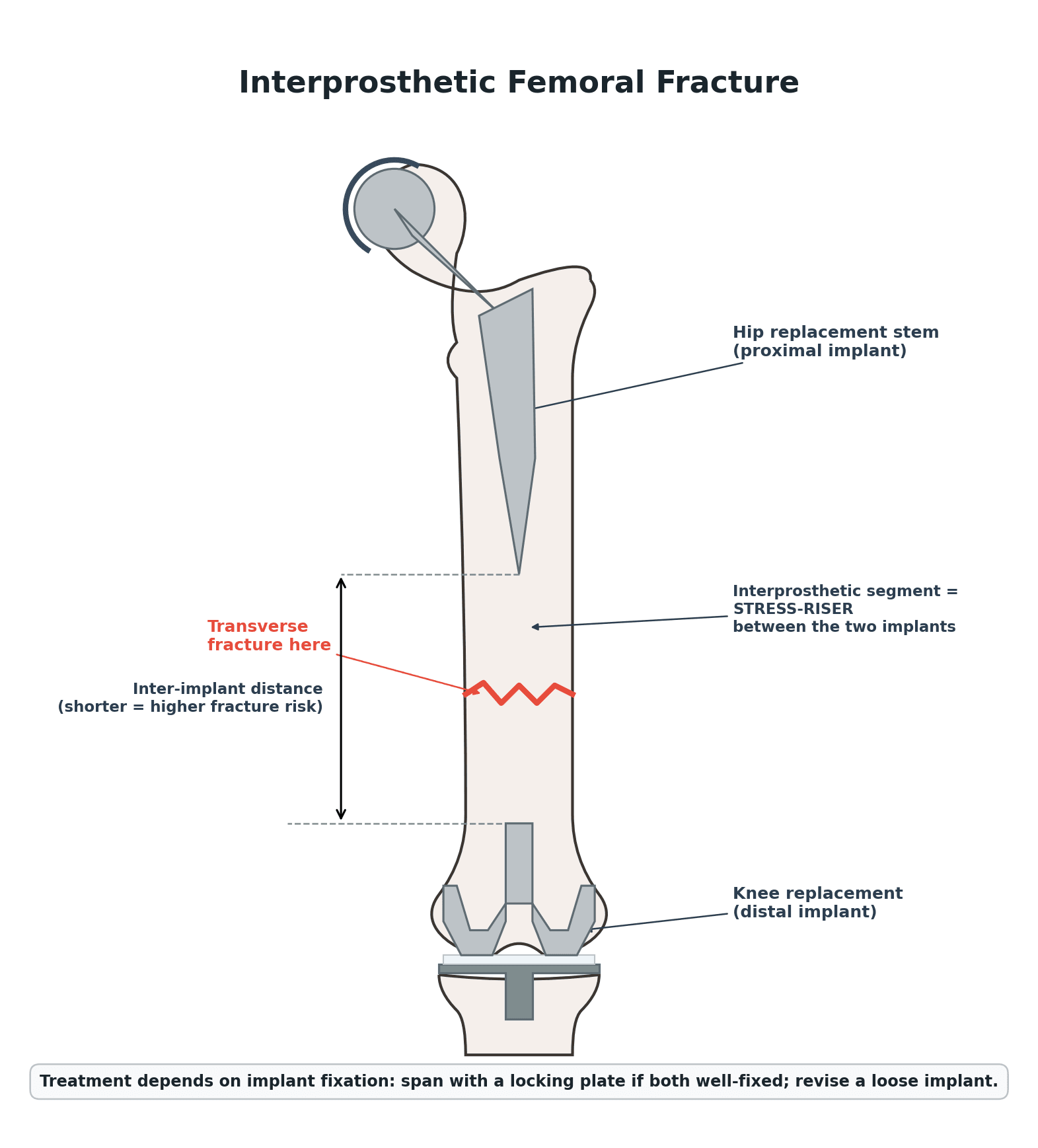
- An interprosthetic femoral fracture is a fracture of the femoral shaft occurring BETWEEN an ipsilateral HIP implant (a total hip or hemiarthroplasty stem) and a KNEE implant (a total knee femoral component); it is rare but devastating, with incidence rising as more patients have both a hip and a knee replacement and live longer.
- The fundamental biomechanical concept is that the bone TRAPPED between two implants is a STRESS RISER: a SHORT inter-implant (inter-stem) distance concentrates stress, and osteoporosis, osteolysis, cortical defects (including old screw holes), loose implants and a fall all increase the risk - so prevention includes avoiding leaving a short, unsupported inter-implant segment.
- Assessment must determine the FRACTURE LOCATION and, critically, the FIXATION STATUS of BOTH implants (is the hip stem well-fixed or loose? is the knee femoral component well-fixed?), because implant stability - more than the fracture pattern alone - drives the treatment decision; the hip side is often classified with Vancouver-type thinking (B1 well-fixed, B2/B3 loose stem) and the distal/knee side by remaining bone stock and component fixation.
- When BOTH implants are WELL-FIXED, treatment is OPEN REDUCTION AND INTERNAL FIXATION, and the key principle is to use a SPANNING construct - a long locked plate that bridges essentially the WHOLE femur (overlapping or engaging both implants) - so that the fixation does NOT create a new short, unsupported segment (a new stress riser) between the plate end and an implant.
- When an implant is LOOSE or the bone is deficient, REVISION/REPLACEMENT is required: a loose hip stem is treated with revision to a long stem (that may bypass the fracture), and a loose knee component or deficient distal femoral bone is treated with a distal femoral replacement (megaprosthesis), with total femoral replacement reserved for the worst combined bone loss.
- Outcomes are POOR with HIGH REOPERATION rates: a large series reported only around 71% two-year survivorship free of reoperation, with periprosthetic joint INFECTION the commonest reason for reoperation (also nonunion, refracture, hardware failure), and fractures occurring between TWO STEMMED components carried the highest reoperation and infection risk - so these are high-risk reconstructions requiring careful planning, robust fixation and infection vigilance.
- “Interprosthetic femoral fracture = femoral shaft fracture BETWEEN an ipsilateral hip and knee implant; the inter-implant bone is a STRESS RISER (short inter-stem distance, osteoporosis).
- “Assess BOTH implants' fixation - implant stability drives treatment. Well-fixed both -> ORIF with a SPANNING plate bridging the WHOLE femur (don't create a new stress riser); loose hip stem -> revision long stem; deficient distal bone -> distal/total femoral replacement.
- “High reoperation rate (~71% 2-yr survivorship free of reop); PJI the commonest cause; fractures between two STEMMED components are highest risk.
Femoral shaft fracture between a hip and a knee implant - the inter-implant bone is a stress riser (worse with a short inter-stem distance and osteoporosis).
Assess both implants' fixation. Well-fixed -> ORIF with a spanning plate bridging the whole femur (no new stress riser); loose/deficient -> revision / distal-femoral replacement.
The Stress Riser, Assessment & Treatment Principle
An interprosthetic femoral fracture occurs in the femoral shaft between an ipsilateral hip implant and a knee implant, and the bone trapped between them is a stress riser - a short inter-implant distance, osteoporosis and cortical defects all increase the risk. Assessment must define the fracture location and the fixation status of BOTH implants, because implant stability drives treatment (hip side: Vancouver-type B1 well-fixed vs B2/B3 loose; distal side: bone stock and knee-component fixation). With both implants well-fixed, treat by ORIF using a spanning locked plate that bridges essentially the whole femur so the construct does NOT create a new short unsupported segment. With a loose implant or deficient bone, revise/replace: a loose hip stem -> long revision stem; deficient distal bone/loose knee -> distal femoral replacement. These are high-risk reconstructions with high reoperation and infection rates.
Operative Strategy
- Assess both implants' fixation (and bone stock) on imaging - this, not the fracture pattern alone, determines treatment.
- Both implants well-fixed -> ORIF with a spanning construct: a long locked plate bridging essentially the whole femur, overlapping/engaging both implants, so no new short unsupported segment (stress riser) is created; use locking screws around stems and cables where needed.
- Loose hip stem -> revision to a long stem (bypassing the fracture by adequate cortical diameters).
- Loose knee component or deficient distal bone -> distal femoral replacement (megaprosthesis); total femoral replacement for the worst combined bone loss.
- Anticipate complications: high reoperation rate, with periprosthetic joint infection the commonest cause (also nonunion, refracture, hardware failure) - meticulous technique, biology and infection prophylaxis.
The defining technical error in fixing an interprosthetic femoral fracture is to use a construct that leaves a new short, unsupported segment of bone between the end of the plate and an implant - this simply creates a fresh stress riser and predisposes to a refracture. The principle is therefore to SPAN the whole femur, bridging or engaging both implants with a long locked plate (and cables/locking screws around the stems), rather than using a short plate confined to the fracture. Equally, the decision between fixation and revision/replacement hinges on implant stability and bone stock, so both implants must be assessed: a loose hip stem needs revision and a deficient distal femur needs a distal femoral replacement, not ORIF. Finally, because reoperation - most often for infection - is common, these reconstructions demand careful planning, robust biology-respecting fixation and infection vigilance.
The Inter-Implant Distance: Biomechanics and Prevention
- Where stress concentrates: bending load peaks at the junction between stiff (implant/cement) and compliant (bone) zones - i.e. at the tip of a stem and the end of any rigid construct. A femur with two implants therefore has two such zones, and the bone between them carries the load.
- Why a short distance is dangerous: a short inter-implant (stem-tip-to-stem-tip) distance leaves little compliant bone to dissipate the load, so bending stress is concentrated over a small segment - in one case report the inter-stem distance was around 50 mm before the fracture. Osteoporosis, osteolysis and old screw holes lower the threshold further.
- Prevention (the planning rule): when placing a second arthroplasty or a long stem in a femur that already has one, either preserve an adequate inter-implant bone distance or plan to overlap/bridge the constructs so no short unsupported gap remains; avoid a stem tip adjacent to a cortical defect.
- Prophylactic plating must cover the stress zone, not relocate it: a reinforcing plate has to extend past and overlap the stem-tip stress-concentration region, because a plate that ends at the stem tip (e.g. subtrochanterically beneath a hip stem) simply moves the stress riser to the plate end and can still fracture - exactly the failure described in the cited case.
Stress peaks at stem tips / construct ends; a short inter-stem distance concentrates it over a small bone segment. Prevent it by keeping the implants an adequate distance apart or overlapping them, and ensure any prophylactic plate extends past the stem tip - a plate that ends at the stem tip just relocates the stress riser.
Building the Spanning Construct Around Well-Fixed Implants
A spanning locked plate overlapping and engaging both implants, with locking screws around stems and cables where needed, raises the practical "how" - because you cannot drill a bicortical screw through a well-fixed stem or the box of a knee component:
- Around the hip stem: cerclage cables/wires, unicortical or variable-angle locking screws angled around the stem, and a locking attachment plate (LAP) that clamps to the plate and grips the bone beside the implant.
- At the fracture and screw-free bone: standard bicortical locking/cortical screws where there is no implant - this is where the construct gets its strongest hold.
- Around the knee component: a distal-femoral periarticular locking plate with multiple divergent/variable-angle locking screws into the distal fragment around the component.
- Get fixation in all three zones (proximal around the hip stem, the central fracture, and distal around the knee component) and overlap both implants so there is no unsupported gap; where a single plate cannot span safely, use overlapping constructs (e.g. plate plus retrograde nail, or two overlapping plates), and add an anterior strut allograft in poor bone.
- If an implant is loose, this does not apply - revise the loose hip stem (long stem bypassing the fracture) or use a distal femoral replacement for a loose knee/deficient distal bone (see Revision THA, Revision TKA and Periprosthetic Knee Fracture).
You can't screw through a well-fixed stem, so the spanning plate uses cerclage cables, unicortical/variable- angle locking screws and a locking attachment plate around the stem, bicortical screws in screw-free bone, and a periarticular distal-femoral plate around the knee component - with fixation in all three zones and no unsupported gap. Use overlapping plate-plus-nail/two-plate constructs when one plate won't span.
How Bad Is It? Interprosthetic Versus Ordinary Periprosthetic Fracture
A direct comparison against ordinary periprosthetic femoral fractures at the same centre puts figures on how rare and how devastating these are, and the pattern is consistent: the interprosthetic patient is frailer to start with and does worse afterwards.
- Interprosthetic
- 74 years
- Periprosthetic
- 69 years
- Interprosthetic
- 33%
- Periprosthetic
- 11%
- Interprosthetic
- 40%
- Periprosthetic
- 21%
- Interprosthetic
- 15%
- Periprosthetic
- 4%
- Interprosthetic
- 23%
- Periprosthetic
- 7%
- Interprosthetic
- 15%
- Periprosthetic
- 4%
- Interprosthetic
- 811 mL
- Periprosthetic
- 513 mL
Two of those rows change practice rather than merely describing it. Forty per cent presented with a loose implant - double the periprosthetic rate - which is the hard evidence behind this page's insistence on assessing the fixation of both components rather than planning from the fracture line. And a 15% mortality places this alongside a hip fracture in an elderly patient: it is a life-threatening event in a frail person, not simply a difficult reconstruction, and the peri-operative medical care matters as much as the construct.
Afterwards: Weight-Bearing and the Functional Reality
Can they weight-bear?
This is the question that decides whether the operation helps, because a frail 80-year-old told to stay non-weight-bearing for six weeks frequently cannot comply and deconditions instead. The reassuring finding is that in a cohort of periprosthetic femoral fractures plated and split by weight-bearing protocol, immediate full weight-bearing made no difference to mechanical complications, to one-year mortality, or to walking level at one year compared with a delayed protocol of at least six weeks. Early weight-bearing is therefore achievable when the construct is genuinely stable, and the default of routine protection is not supported.
A newer option bears directly on this. Nail-plate hybrid constructs - a retrograde nail combined with a lateral plate, giving a load-sharing intramedullary implant alongside the plate - are increasingly used for these fractures precisely because they permit immediate loading. In the comparison above, 6 of 7 patients treated with a nail-plate construct were immediately weight-bearing as tolerated against 9 of 23 treated otherwise, and none of the nail-plate constructs failed against 30% of the others. The numbers are small and the comparison is not randomised, so this is a promising direction rather than a settled standard - but it belongs in the discussion of how to span a femur when the patient cannot protect it.
The functional outcome to counsel
Be honest about the ceiling. In the plated cohort, 91.8% united by six months, which sounds excellent - but at one year only about a third had resumed independent walking, a third were using a walker, and roughly one in twelve was a non-walker. Union is not the outcome the patient experiences. The realistic conversation is that the aim is to return them to their pre-injury mobility, which is often already limited, rather than to restore normal function - and reassuringly, pre- and post-operative walking levels did not differ significantly, so that aim is achievable.
Mnemonics & Memory Aids
SPAN
Hook:SPAN: Stress riser, Probe both implants, All the femur (span it), Not fixable if loose -> revise/replace (watch infection).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is an interprosthetic femoral fracture and what determines its treatment?”
“What are the technical principles and the expected complications of fixing one?”
Concept
- Femoral shaft fracture between an ipsilateral hip and knee implant
- Inter-implant bone is a stress riser (short inter-stem distance, osteoporosis, cortical defects)
- Rising incidence (ageing, multiply-replaced patients)
Assessment
- Fracture location + fixation status of BOTH implants (and bone stock)
- Hip side: Vancouver-type (B1 well-fixed, B2/B3 loose)
- Implant stability drives treatment (not fracture pattern alone)
Treatment
- Both well-fixed -> ORIF with a spanning plate bridging the WHOLE femur (no new stress riser)
- Loose hip stem -> revision long stem (bypass fracture)
- Loose knee/deficient distal bone -> distal (or total) femoral replacement
Outcomes
- High reoperation rate (~71% 2-yr survivorship free of reoperation)
- Periprosthetic joint infection the commonest cause; also nonunion/refracture/hardware failure
- Highest risk between two stemmed components
Evidence & Key Studies
High rate of unplanned reoperation for interprosthetic femur fractures
- In 76 surgically managed interprosthetic femur fractures, treatment followed implant stability: well-fixed (Vancouver B1/C) fractures had ORIF, loose stems (B2/B3) had revision, and deficient distal bone was treated with distal femoral replacement.
- The 2-year survivorship free of reoperation was only 71%, with periprosthetic joint infection the commonest reason for reoperation (also refracture, nonunion, hardware failure, instability).
- Fractures involving a stemmed femoral knee component (i.e. between two stemmed implants) had a significantly increased risk of reoperation and infection; ORIF and revision had similar survivorship.
Stress concentration and inter-implant distance in (inter)prosthetic femoral fractures
- With both a hip stem and a knee prosthesis in the femur, the short inter-implant (inter-stem) distance concentrates stress and predisposes to interprosthetic/periprosthetic fracture.
- Prophylactic plate reinforcement can still fail if it does not adequately protect the stress-concentration region (e.g. a plate ending at the subtrochanteric region with a hip stem in situ).
- Awareness of stress-concentration points is important for both prevention and the design of fixation constructs.
Characteristics and outcomes of interprosthetic versus periprosthetic femur fractures
- 30 interprosthetic against 246 periprosthetic femoral fractures at one Level 1 trauma centre: the interprosthetic patients were older (74 vs 69), more often osteoporotic (33% vs 11%) and more often smokers.
- 40% presented with an UNSTABLE prosthesis against 21% of periprosthetic fractures - the evidence behind assessing the fixation of both implants rather than planning from the fracture line.
- Mortality was 15% versus 4%, implant failure 23% versus 7% and superficial infection 15% versus 4%; of seven treated with nail-plate hybrid constructs, six were immediately weight-bearing and none failed, against 30% failure with other techniques.
Locking plates for periprosthetic femoral fractures: union, weight-bearing and functional outcome in 89 patients
- 89 periprosthetic femoral fractures (including 4 interprosthetic), mean age 81, plated and divided by protocol into immediate versus delayed (at least 6 weeks) full weight-bearing.
- 91.8% united by six months, but at one year only 36.2% had resumed independent walking, 33.3% used a walker and 8.7% were non-walkers; mortality was 12.4% at one year.
- Time to full weight-bearing had no significant effect on walking level at one year, on complications, or on mortality - and pre- and post-operative walking levels did not differ significantly.
The implant-stability-driven treatment algorithm (ORIF for well-fixed, revision for loose stems, distal femoral replacement for deficient distal bone), the high reoperation rate (about 71% two-year survivorship free of reoperation) with periprosthetic joint infection the commonest cause, and the highest risk between two stemmed components come from the cited Neitzke series; the stress-concentration/inter-implant- distance concept and the caution that inadequately positioned reinforcement can still fail from the cited Taniguchi report. The spanning-fixation principle (bridge the whole femur to avoid a new stress riser) and the Vancouver-type assessment of the hip side are standard, well-established teaching. The interprosthetic-versus-periprosthetic comparison, the mortality and loose-implant rates and the nail-plate construct data come from the cited Blackwood cohort; the weight-bearing and functional-outcome findings from the cited Santoni series. (See also Periprosthetic Hip Fracture, Periprosthetic Fracture of the Hip, Periprosthetic Knee Fracture, Revision THA and Revision TKA.)