Symptomatic Synovial Plicae
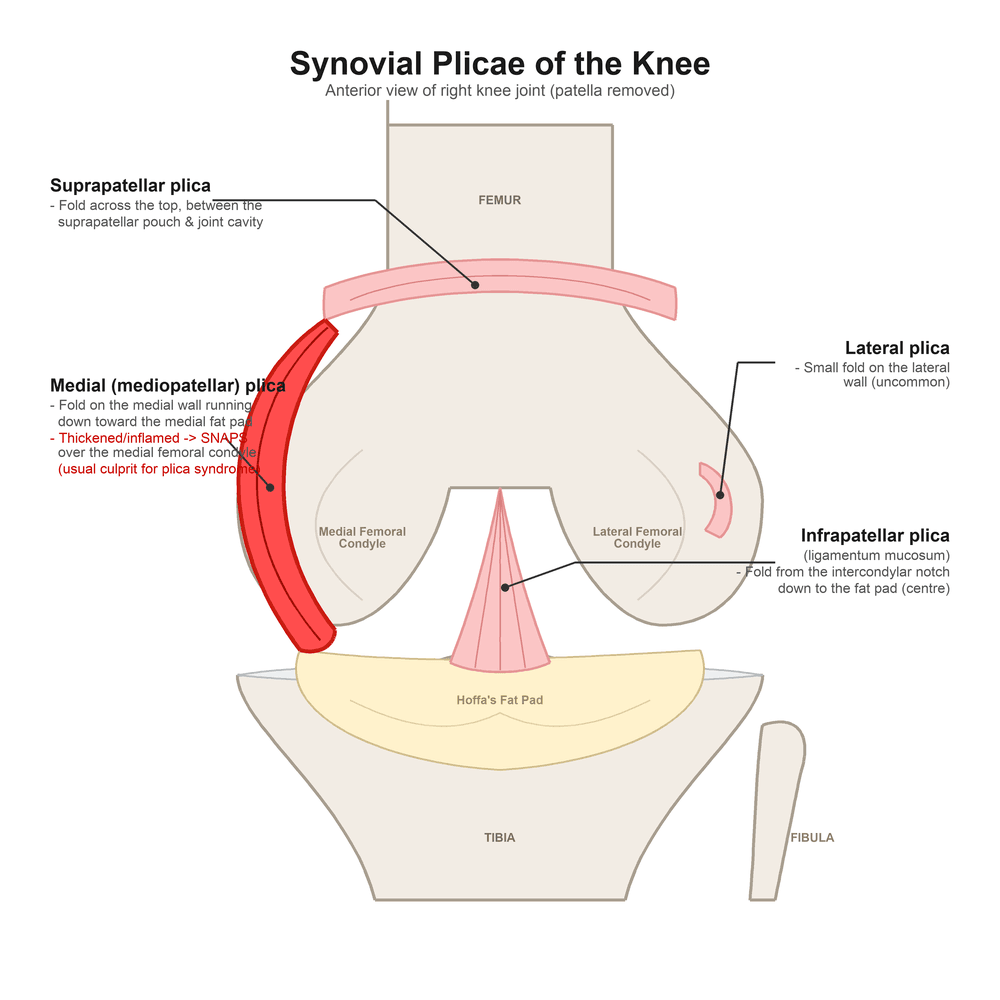
- Synovial plicae are normal EMBRYOLOGICAL folds (septal remnants) of the knee synovium and there are four recognised types - the SUPRAPATELLAR, the MEDIAL (mediopatellar / medial parapatellar), the INFRAPATELLAR (ligamentum mucosum) and the (uncommon) LATERAL plica; they are present in a large proportion of normal knees and are usually ASYMPTOMATIC incidental findings, so the mere presence of a plica is not a diagnosis.
- The MEDIAL (mediopatellar) plica is the one that most often becomes symptomatic: when it becomes THICKENED, fibrotic and inflamed - often after overuse or minor trauma - it loses its elasticity and SNAPS over the medial femoral condyle during flexion/extension, producing anteromedial knee pain and, over time, abrasion of the medial femoral condyle and adjacent patellar cartilage (a chondral 'footprint').
- The CLINICAL picture is ANTEROMEDIAL knee pain, often in a young patient (frequently female), with CLICKING or SNAPPING, a sensation of PSEUDO-LOCKING or giving way, and pain that is worse with stairs, squatting and prolonged sitting (the theatre sign); examination classically reveals local MEDIAL PARAPATELLAR tenderness and a PALPABLE, tender, cord-like band medial to the patella that may be felt to snap as the knee is extended.
- DIAGNOSIS is clinical, supported by MRI, which can show a thickened medial plica (best seen with a joint effusion) and any associated infrapatellar fat-pad or chondral change; however, plica syndrome is to a degree a diagnosis of exclusion (other causes of anteromedial pain must be excluded) and is frequently confirmed (and treated) at ARTHROSCOPY, which directly visualises the pathological plica and any chondral footprint.
- MANAGEMENT is CONSERVATIVE first: activity modification, NSAIDs, physiotherapy (quadriceps/VMO and flexibility work) and sometimes a corticosteroid injection - many symptomatic plicae settle with non-operative treatment.
- For symptoms RECALCITRANT to adequate conservative treatment, ARTHROSCOPIC RESECTION of the symptomatic plica gives excellent results - studies in young patients show significant improvement in knee scores and pain, and outcome is not adversely affected by trauma, high-impact sport, plica type or a low-grade (ICRS grade I) medial-condyle cartilage lesion; a reduplicated/atypical plica anatomical variant can be recalcitrant to conservative treatment and respond to resection.
- “Synovial plicae = embryological folds (suprapatellar, MEDIAL, infrapatellar, lateral); usually asymptomatic - presence alone is NOT a diagnosis.
- “MEDIAL (mediopatellar) plica is the one that symptomises: thickened/inflamed -> SNAPS over the medial femoral condyle -> anteromedial pain, clicking, pseudo-locking; palpable tender band medial to patella.
- “Clinical + MRI diagnosis (often confirmed at arthroscopy). CONSERVATIVE first (physio, NSAIDs, +/- injection); ARTHROSCOPIC RESECTION for refractory cases (excellent results in the young).
Anteromedial knee pain with clicking/snapping and pseudo-locking, worse on stairs/squatting/sitting, and a palpable tender band medial to the patella - usually a medial (mediopatellar) plica.
Plicae are common and usually asymptomatic - presence alone is not a diagnosis. It is partly a diagnosis of exclusion; conservative treatment first.
Types, Pathology & Diagnosis
Synovial plicae are normal embryological folds of synovium - the suprapatellar, medial (mediopatellar), infrapatellar (ligamentum mucosum) and (uncommon) lateral plicae - present in many normal knees and usually asymptomatic. The medial (mediopatellar) plica is the one that most often becomes symptomatic: when it thickens, becomes fibrotic and inflamed it snaps over the medial femoral condyle, causing anteromedial knee pain and, over time, abrasion of the condyle/patellar cartilage. The clinical picture is anteromedial pain (often in a young, frequently female patient) with clicking/snapping, pseudo-locking, and pain worse on stairs, squatting and prolonged sitting, with a palpable tender band medial to the patella. Diagnosis is clinical plus MRI (a thickened plica, best with an effusion), but it is partly a diagnosis of exclusion and is frequently confirmed at arthroscopy.
- Location
- Between suprapatellar pouch and joint
- Note
- Usually asymptomatic; can be complete (septum)
- Location
- Medial wall, runs to the medial fat pad
- Note
- The one that MOST often becomes symptomatic (snaps over medial femoral condyle)
- Location
- From intercondylar notch to fat pad
- Note
- Common; rarely symptomatic (can mimic an ACL band at arthroscopy)
- Location
- Lateral wall (uncommon)
- Note
- Rarely symptomatic
Where Plicae Come From, and Why That Matters
Calling a plica an "embryological remnant" is only useful if you can say a remnant of what.
In the developing knee, mesenchymal tissue between the femur and tibia is resorbed to create the joint cavity, but it does so in stages: three separate synovial compartments form first - a medial, a lateral and a suprapatellar cavity - divided by synovial septa. Those septa normally break down around the third to fourth month of gestation, leaving a single cavity. A plica is the part of a septum that never fully resorbed, which is why each named plica sits exactly where its septum used to be: the suprapatellar plica along the old division between the suprapatellar pouch and the joint, the medial plica on the medial wall, and the infrapatellar plica running from the intercondylar notch to the fat pad.
Two consequences follow. First, a plica is normal tissue in an unusual amount, not a lesion - which is why finding one means very little on its own. Second, incomplete resorption is common and highly variable: reported frequencies differ widely between arthroscopic, cadaveric and MRI series, and that variability is itself the argument against treating a plica as a diagnosis. What turns a normal fold into a symptomatic one is acquired change - repetitive flexion and extension, a direct blow, or a haemarthrosis - producing inflammation, fibrosis and loss of elasticity, so the fold stops gliding and starts to bowstring.
Why the snap happens where it does
The medial plica runs obliquely from the medial wall to the fat pad, and during flexion the medial femoral condyle advances beneath it. Through the first part of flexion the plica sits harmlessly on the condyle; as the knee passes roughly 30 to 60 degrees, a taut, fibrotic plica is drawn tightly across the condyle and then snaps over its anterior margin - which is why the pain and the palpable click occur in mid-flexion rather than at either extreme, why the symptoms are provoked by stairs and squatting, and why compressing the plica against the condyle in extension reproduces the pain while further flexion relieves it. The repeated passage of a hard fibrotic band across the same strip of cartilage is what produces the chondral footprint on the anterior medial femoral condyle.
Grading the Medial Plica: the Sakakibara (Arthroscopic) Classification
Medial plica thickening, snapping over the condyle and the "reduplicated/double" variant are all captured by the arthroscopic Sakakibara classification, which grades the medial (mediopatellar) plica by how much it covers the anterior medial femoral condyle - a measure that tracks its symptomatic and chondral-damage potential.
- Arthroscopic appearance
- A cord-like elevation in the synovial wall
- Significance
- Small; usually asymptomatic
- Arthroscopic appearance
- A shelf-like fold that does NOT cover the anterior medial femoral condyle
- Significance
- Usually asymptomatic
- Arthroscopic appearance
- A large shelf-like fold that DOES cover the anterior medial femoral condyle
- Significance
- More often symptomatic; can abrade the condyle
- Arthroscopic appearance
- A fenestrated or double (reduplicated) plica
- Significance
- Symptomatic/atypical variant; often recalcitrant to conservative care
Sakakibara grades the medial plica A (cord) - B (shelf not covering the MFC) - C (shelf covering the anterior MFC) - D (fenestrated/double). The larger types C and D are the ones that snap over and abrade the medial femoral condyle and are most likely to be symptomatic - type D being the reduplicated variant that resists conservative treatment.
Examining for a Symptomatic Medial Plica
- Roll the band. Palpate the cord-like, tender plica band medial to the patella and roll it under the fingers; tenderness localised to it is suggestive.
- Mediopatellar plica (MPP) test. With the knee in extension, push the patella medially (and inferomedially) with the thumb to compress the plica between the patella and the medial femoral condyle - reproduction of the patient's pain is positive; the pain typically eases as the knee flexes (the plica moves off the condyle).
- Hughston's / flexion-extension (stutter) test. While palpating the medial band, flex and extend the knee through roughly mid-range; a palpable, sometimes painful snap or "stutter" as the plica rolls over the medial femoral condyle supports the diagnosis.
- Always exclude the mimics. Because plicae are common incidentally, pair these tests with a full knee examination to exclude patellofemoral pain, meniscal and chondral pathology before attributing symptoms to the plica.
Two named tests: the MPP test (knee extended, push the patella medially -> reproduces pain, eases on flexion) and the flexion-extension "stutter"/Hughston test (palpate the medial band while flexing-extending -> a snap over the medial femoral condyle). A positive test plus a tender snapping band plus exclusion of other anteromedial causes is what makes the diagnosis - not the plica's mere presence.
Management
- Conservative first: activity modification, NSAIDs, physiotherapy (quadriceps/VMO and flexibility), and sometimes a corticosteroid injection - many symptomatic plicae settle non-operatively.
- Confirm it is the plica: anteromedial pain with a snapping tender band, supportive MRI, and exclusion of other anterior/anteromedial causes (patellofemoral pain, meniscal pathology, chondral lesions).
- Arthroscopic resection for symptoms recalcitrant to adequate conservative treatment - it gives excellent results, with significant improvement in knee scores and pain in young patients, and outcome is not worsened by trauma, high-impact sport, plica type or a low-grade (ICRS grade I) medial-condyle cartilage lesion.
- Atypical variants: a reduplicated/atypical medial plica can be recalcitrant to conservative care and respond to resection (with fat-pad debridement if it is impinging).
Resect it - do not simply divide it
The word matters. Dividing a plica, or releasing it at one end, leaves the fold in place and it commonly scars back down and becomes symptomatic again; the operation is a complete excision of the plica back to the synovial wall, taken far enough proximally and distally that no thickened band remains to re-tether. The practical points at arthroscopy:
- Look before you resect. Confirm the plica is genuinely pathological - thickened, fibrotic, avascular or frayed - and look for the corroborating chondral footprint on the anterior medial femoral condyle. A thin, soft, mobile fold in a knee whose pain is coming from somewhere else should be left alone.
- Resect completely, taking the whole band rather than dividing it, and check through a full arc of flexion and extension that nothing remains to catch.
- Address what accompanies it - an impinging hypertrophied infrapatellar fat pad, and any chondral lesion.
- Haemostasis matters, since the plica is vascular at its base and a postoperative haemarthrosis both hurts and promotes the fibrosis you were trying to remove.
The complications to counsel for are recurrence from incomplete excision, persistent pain when the plica was never the real source, haemarthrosis, and the general arthroscopic risks including stiffness and infection. The first two are both failures of selection rather than of technique, which is why the diagnosis has to be earned before the arthroscope is picked up.
The key judgement in plica syndrome is restraint: synovial plicae are present in a large proportion of normal, pain-free knees and are usually incidental, so finding a plica on MRI or at arthroscopy does NOT by itself explain a patient's pain. Plica syndrome is partly a diagnosis of exclusion - the symptoms (anteromedial pain, a snapping tender band, pseudo-locking) must fit, and other causes of anterior/anteromedial knee pain such as patellofemoral pain, meniscal tears and chondral lesions must be excluded - before attributing the problem to the plica and certainly before resecting it. Treat conservatively first; reserve arthroscopic resection for the genuinely symptomatic, recalcitrant plica, where results are excellent.
Mnemonics & Memory Aids
PLICA
Hook:PLICA: Plicae (folds), Lateral/etc but medial symptomises, Inflamed plica snaps over condyle, Click/anteromedial pain, Arthroscopic resection if refractory.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young patient has anteromedial knee pain with clicking and a palpable band medial to the patella. What is your diagnosis and how do you confirm it?”
“How would you manage symptomatic knee plica syndrome?”
Types
- Embryological synovial folds: suprapatellar, medial (mediopatellar), infrapatellar (ligamentum mucosum), lateral
- Common in normal knees - usually asymptomatic
- Medial (mediopatellar) plica is the one that usually symptomises
Pathology & presentation
- Thickened/inflamed medial plica snaps over the medial femoral condyle (can abrade cartilage)
- Anteromedial pain, clicking/snapping, pseudo-locking; worse on stairs/squatting/sitting
- Palpable tender band medial to the patella (often young, female)
Diagnosis
- Clinical + MRI (thickened plica, best with effusion)
- Partly a diagnosis of exclusion (plicae are common/asymptomatic)
- Often confirmed at arthroscopy (plica + chondral footprint)
Management
- Conservative first: activity modification, NSAIDs, physio (VMO/flexibility), +/- injection
- Arthroscopic resection for refractory cases (excellent results in young)
- Outcome not worsened by trauma/sport/plica type/ICRS grade I lesion
Evidence & Key Studies
Symptomatic medial synovial plica of the knee: arthroscopic resection outcomes in young patients
- Symptomatic medial synovial plica is an underestimated pathology in young patients (mean age about 16 years, predominantly female).
- Arthroscopic resection produced significant improvement in KOOS, Tegner activity, Kujala anterior knee pain score and pain at a mean 20-month follow-up.
- Trauma, high-impact sport, plica type and a low-grade (ICRS grade I) medial-femoral-condyle cartilage lesion did not adversely affect the outcome.
Reduplicated medial parapatellar plica: an anatomical variant recalcitrant to conservative treatment
- A medial parapatellar plica presented with anteromedial knee pain aggravated by descending stairs and prolonged sitting, with medial parapatellar tenderness and a palpable click on extension.
- MRI suggested a duplicated medial plica with infrapatellar fat-pad change; after conservative treatment failure, arthroscopy confirmed two medial plicae and fat-pad hypertrophy.
- Resection of the plicae and impinging fat pad fully resolved symptoms with no recurrence at one year.
The excellent outcomes of arthroscopic resection of a symptomatic medial plica in young patients, and the finding that trauma, high-impact sport, plica type and low-grade cartilage lesions do not worsen outcome, come from the cited Hufeland study; the typical presentation (anteromedial pain worse on stairs/ prolonged sitting, medial parapatellar tenderness and a palpable click), the MRI appearance and the response of an atypical reduplicated plica to resection from the cited Marin Fermin report. The classification of synovial plicae and the conservative-first pathway are standard, well-established teaching, as are the embryology of the synovial septa, the mid-flexion mechanism of the snap and the resect-rather-than-divide principle. (See also Chondromalacia Patellae, which sets out the wider anterior knee pain differential, Patellofemoral Instability, Lateral Patellar Compression Syndrome and Articular Cartilage Injuries.)