Image-Guided Spinal Instrumentation
- Pedicle-screw accuracy is the central metric, graded by the GERTZBEIN-ROBBINS classification (grade A = fully contained, B = breach under 2 mm, and so on), and both NAVIGATION (intraoperative image guidance) and ROBOTIC assistance improve accuracy over conventional FREEHAND and FLUOROSCOPY-guided techniques.
- NAVIGATION uses intraoperative imaging - most powerfully 3D imaging from an intraoperative CT/O-arm (or fluoroscopy-based 2D-3D) - registered to the patient so instruments are tracked in real time against the image, allowing the surgeon to plan and follow a pedicle-screw trajectory; it offers good accuracy with relatively SHORTER operative times than robotics.
- ROBOTIC systems (such as Mazor X, ROSA, ExcelsiusGPS and Cirq) position a guide/arm along a PRE-PLANNED trajectory for screw insertion; meta-analyses show robots achieve high Gertzbein-Robbins grade A/B accuracy (around 98%, with no single platform clearly superior to the others) and are MORE accurate than traditional methods, but at the cost of generally LONGER operative time (especially with setup/registration) and higher cost.
- The clinical BENEFITS beyond accuracy include generally FEWER intraoperative revisions and reoperations than freehand/fluoroscopic insertion, and importantly a reduction in RADIATION exposure to the SURGEON and theatre staff (the surgeon is away from the beam during navigated/robotic insertion) - although intraoperative CT delivers a radiation dose to the PATIENT that must be weighed.
- In a head-to-head sense, ROBOTICS tends to give the highest ACCURACY (valuable in complex/deformity cases) but takes LONGER, whereas NAVIGATION gives good accuracy with shorter operative times - so the choice balances precision against time/cost; in deformity surgery there is generally no significant difference between them in blood loss, curve correction or hospital stay.
- The TRADE-OFFS and PITFALLS are important: high capital and per-case COST, a LEARNING CURVE, added setup/registration time, and technical errors - REGISTRATION inaccuracy (the navigation image no longer matching the patient, e.g. after reference-frame movement or inter-segmental motion), LINE-OF-SIGHT issues with optical tracking, and tool 'SKIVE'/deflection off bone - so navigation/robotic guidance must be verified against anatomy and not trusted blindly.
- “Pedicle-screw accuracy = Gertzbein-Robbins grading; navigation and robotics both BEAT freehand/fluoroscopy (robots ~98% grade A/B, no platform clearly superior).
- “Robotics = highest accuracy but LONGER operative time/cost; navigation = good accuracy, shorter time. Both reduce SURGEON radiation and reoperations.
- “Pitfalls: cost, learning curve, REGISTRATION error, line-of-sight, tool skive, and patient CT radiation - verify against anatomy, don't trust blindly.
Navigation and robotics improve pedicle-screw accuracy (Gertzbein-Robbins) over freehand/fluoroscopy (robots ~98% grade A/B), with fewer reoperations and less surgeon radiation.
Cost, learning curve, longer operative time (robotics), and technical pitfalls - registration error, line-of-sight, tool skive, and patient CT radiation.
Trade-offs, Pitfalls & Practical Use
- Choose by case: robotics for maximal precision in complex/deformity cases (accepting longer time/cost); navigation for good accuracy with efficiency; freehand/fluoroscopy remains valid for standard cases.
- Registration is everything: the navigation image must accurately match the patient - reference-frame movement, inter-segmental motion between registration and insertion, or drift cause registration error and inaccurate screws.
- Watch line-of-sight and skive: optical tracking needs an unobstructed line of sight, and the drill/tap can skive (deflect) off a sloped pedicle/facet despite correct planning.
- Radiation balance: the surgeon's radiation falls, but intraoperative CT gives the patient a dose - justify and optimise it (especially in children).
- Account for cost and the learning curve: capital and per-case cost and a real learning curve are part of the decision; verify trajectories against bony anatomy intraoperatively rather than trusting the screen alone.
Navigation and robotics genuinely improve pedicle-screw accuracy over freehand and fluoroscopy and reduce both reoperations and surgeon radiation, which is their real value in deformity, complex-anatomy, minimally invasive and revision surgery. But the technology is only as good as its REGISTRATION: if the reference frame moves, if there is inter-segmental motion between registration and screw insertion, or if there is drift, the on-screen trajectory no longer matches the patient and a confidently 'navigated' screw can be malpositioned. Optical systems also need line-of-sight, and the drill can skive off a sloped pedicle. The safe surgeon therefore treats the guidance as an aid, re-checks registration, and verifies screw trajectories against the bony anatomy (and with imaging) intraoperatively, while weighing the cost, the learning curve and the patient's CT radiation dose.
The Gertzbein-Robbins Grade in Full
Every accuracy figure quoted for navigation and robotics is a Gertzbein-Robbins grade, so the full scale is worth knowing rather than just its acceptable end:
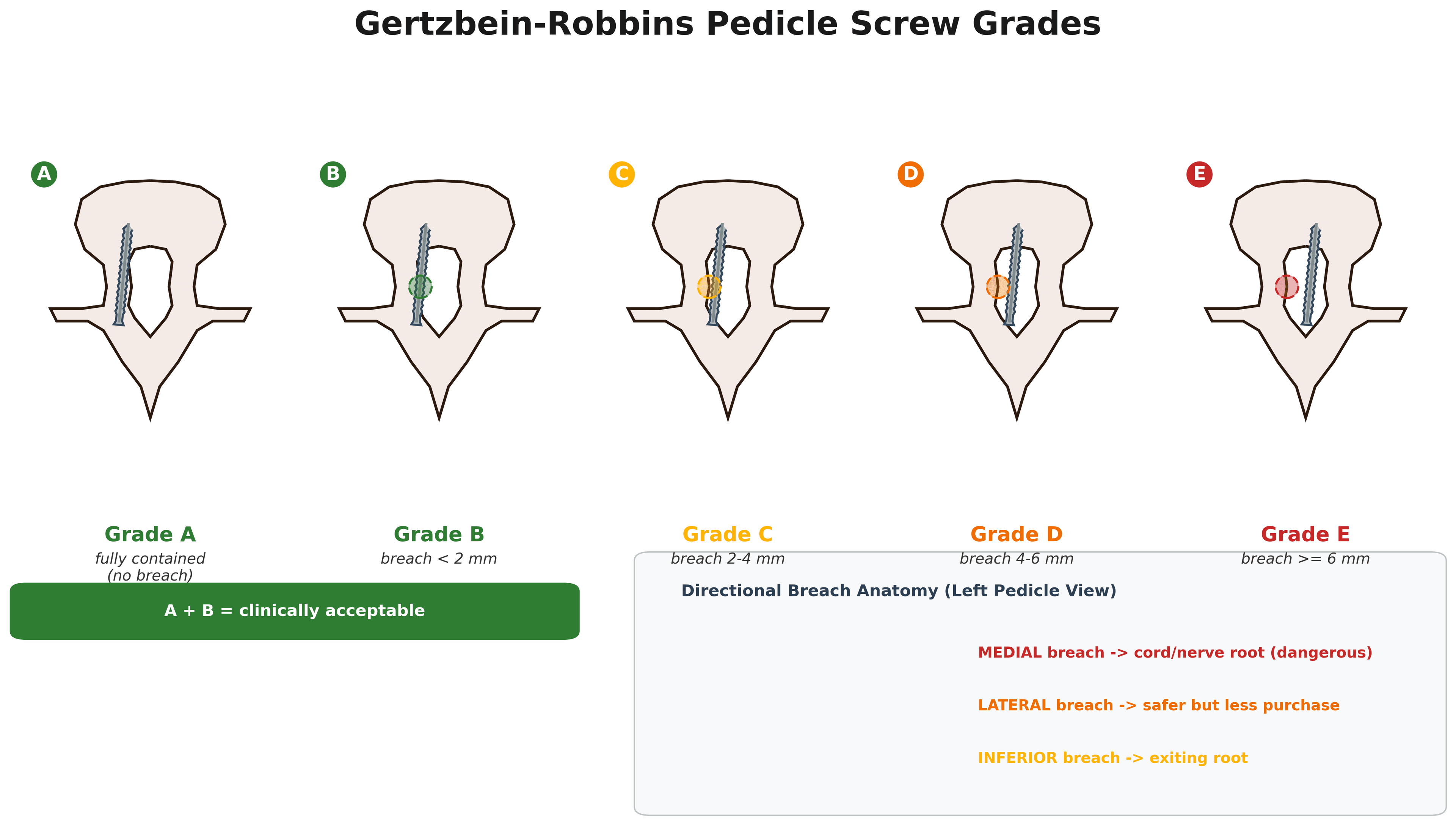
- Grade A - the screw is fully contained within the pedicle, with no cortical breach.
- Grade B - a cortical breach of less than 2 mm.
- Grade C - a breach of between 2 and 4 mm.
- Grade D - a breach of between 4 and 6 mm.
- Grade E - a breach of 6 mm or more.
Grades A and B together are considered "clinically acceptable" (a sub-2-mm breach is within the safety margin), which is why the literature reports combined grade A/B rates (around 98% for robotics). What also matters is the direction of any breach: a medial breach threatens the cord/nerve root and is the dangerous one, an inferior breach risks the exiting root, while a lateral breach is usually safer but sacrifices fixation purchase. So "accuracy" means not just the grade but a contained or safely-directed screw.
Gertzbein-Robbins: A = contained, B = breach under 2 mm, C = 2 to 4 mm, D = 4 to 6 mm, E = 6 mm or more; A + B = clinically acceptable. Always add the direction - a medial breach (cord/root) is the one that matters, lateral is safer but loses purchase.
How Registration Actually Works
- The dynamic reference frame (array): a tracked marker clamped rigidly to a fixed bony landmark (a spinous process, or the iliac crest for lumbosacral/pelvic work). Every instrument position is computed relative to this frame, so if the frame is bumped or shifts, the entire on-screen map is wrong even though it still looks plausible.
- How the image is matched to the patient (registration methods): most powerfully, automatic image-based registration from an intraoperative 3D scan (CT/O-arm), which co-registers the just-acquired volume to the tracked frame with no manual point-picking - fast and accurate. Alternatives are paired-point plus surface matching to a preoperative CT (pick anatomical landmarks, then surface-map - more error-prone), and 2D-3D fluoroscopy-based registration.
- Why accuracy decays - the spine is not a rigid body: registration is exact at the reference level but degrades at levels further away because of inter-segmental motion; so verify or re-register per region, re-spin/re-register after a major correction manoeuvre or any bump, and keep the array out of the working field. Always confirm registration against a known landmark (and verify screws against bony anatomy and imaging) before trusting the guidance. (General CT/fluoroscopy physics and dose are covered in CT Physics, Radiation Dose and Hounsfield Units and Radiation Safety in Orthopaedics.)
Registration = a reference array fixed to bone + a method to match image to patient (automatic intraoperative 3D is best; paired-point/surface-match to preop CT is more error-prone). Because the spine is not rigid, accuracy is best at the reference level and decays with distance - re-register per region, after any bump or big correction, and verify against anatomy.
Does the Accuracy Make the Patient Better? The Honest Answer
An examiner who has heard the accuracy figures will ask the question that matters: a screw that is 2 mm better placed - does the patient notice? The evidence for accuracy is consistent. The evidence that it changes how patients do is much weaker, and a candidate who claims otherwise is easy to dismantle.
Why the two questions come apart. Most malpositioned pedicle screws cause no symptoms whatsoever. A lateral breach may sacrifice purchase without ever troubling the patient; even a modest medial breach is frequently tolerated. Symptomatic malposition requiring revision is uncommon, so the event that better accuracy would prevent is rare - and a technology that reduces a rare event has to be studied in very large numbers before any effect on that event becomes visible. Accuracy is a surrogate outcome: easy to measure, measured in every study, and only loosely coupled to what the patient experiences.
What the appraised evidence says. An umbrella review took 22 published meta-analyses of robot-assisted versus freehand technique and assessed them formally with AMSTAR-2 and GRADE, across 14 associations including "perfect" and "clinically acceptable" screw placement, complications, facet joint violation and radiation. Robot assistance came out favourably - but the certainty of the evidence for the majority of those associations was rated LOW to VERY LOW, and the authors' own conclusion was that the findings need cautious interpretation before being applied in practice. Much of the underlying literature is observational, subject to selection of straightforward cases into the new technology and of difficult ones away from it, and reported by enthusiasts during their own learning curves.
The randomised evidence is still arriving, and it is worth knowing what it is measuring: the ROBARTHRODESE trial randomises 300 patients to robot-assisted versus fluoroscopic freehand thoracolumbar fusion, and its primary outcome is the proportion of Grade A screws - with disability score, pain, complications, reoperation, radiation and a cost-utility analysis as secondary outcomes. The surrogate is still the primary endpoint even in the trials designed to settle the question.
- Status of the evidence
- Consistent and repeatedly reproduced - this much is settled
- Status of the evidence
- Well supported, and mechanistically obvious - the surgeon leaves the beam
- Status of the evidence
- Reasonably supported, and follows directly from the accuracy gain
- Status of the evidence
- Reported, but graded LOW to VERY LOW certainty; largely observational
- Status of the evidence
- NOT established - awaited from randomised trials in progress
- Status of the evidence
- NOT established; the event is too rare for existing studies to show it
How to say this in a viva without sounding either credulous or dismissive. The technology reliably does what it claims - it places screws more accurately and it takes the surgeon out of the radiation beam, and both are worth having. Its value is greatest where the anatomy makes freehand genuinely hazardous: severe deformity, revision with distorted landmarks, high thoracic and cervicothoracic levels, sacropelvic fixation, obesity, and percutaneous minimally invasive work where landmarks are not exposed at all. What it has not yet been shown to do is make an average lumbar fusion turn out better, and the case for buying one rests as much on radiation protection and on capability in complex cases as on outcomes data that does not yet exist.
Mnemonics & Memory Aids
GUIDE
Hook:GUIDE: Gertzbein-Robbins improved, Use robotics for complex, Imaging/navigation efficient, Dose/cost considerations, Errors (registration) - verify.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do navigation and robotics improve spinal instrumentation, and what are the trade-offs?”
“What are the main pitfalls of navigated/robotic screw placement?”
Evidence & Key Studies
Freehand fluoroscopic vs navigation vs robotic pedicle-screw accuracy in AIS (network meta-analysis)
- Across 764 patients and 8,144 screws, robotic-assisted (RBA) insertion offered superior pedicle-screw accuracy compared with both freehand fluoroscopic (FHF) and navigation-assisted (NVA) techniques.
- Robotics was associated with longer operative times; navigation provided a balanced approach with good accuracy and relatively shorter surgery times.
- No significant differences were observed in blood loss, Cobb-angle correction or hospital stay between the techniques.
Accuracy, revision and perioperative outcomes of robot-assisted spine surgery (meta-analysis)
- Across 46 studies (4,670 patients, 25,054 screws) of four robotic systems, weighted Gertzbein-Robbins grade A/B accuracy was about 98% (Cirq 94.2%), with no robot significantly more accurate than the others.
- Robotic accuracy was significantly higher than traditional methods; intraoperative revision and reoperation rates were low.
- Robots tended to be more accurate and were associated with fewer reoperations and less blood loss than freehand, fluoroscopic or CT-navigated techniques; one system had the lowest radiation exposure.
Robot-assisted versus freehand spine surgery: an umbrella review appraising the evidence quality
- Appraised 22 existing meta-analyses (randomised, cohort and observational data) with AMSTAR-2 and GRADE, across 14 associations including 'perfect' and 'clinically acceptable' screw placement, complications, facet joint violation and intraoperative radiation.
- Robot-assisted technique appeared beneficial across those associations.
- The certainty of evidence for the MAJORITY of associations was LOW to VERY LOW, with flaws identified in the underlying meta-analyses.
- The authors advise cautious interpretation and application in clinical practice - the counterweight to headline accuracy figures.
ROBARTHRODESE: randomised trial of robot-assisted versus freehand thoracolumbar fusion (protocol)
- A single-centre evaluator-blinded RCT randomising 300 patients 1:1 to robot-assisted (Mazor X Stealth) versus freehand with 2D fluoroscopy.
- The PRIMARY outcome is the proportion of Gertzbein-Robbins grade A screws - a surrogate, even in a trial designed to settle the clinical question.
- Secondary outcomes include Oswestry Disability Index, pain, complication and reoperation rates, surgeon radiation exposure, facet joint violation, length of stay and a cost-utility analysis.
- A protocol rather than a result: the randomised answer on patient-centred outcomes is awaited, not available.
The comparison showing robotic-assisted insertion superior in accuracy (but with longer operative time) and navigation as a balanced option, with no difference in blood loss/curve correction/hospital stay, comes from the cited Lajczak network meta-analysis; the ~98% Gertzbein-Robbins grade A/B robotic accuracy across multiple platforms (none clearly superior), the low revision/reoperation rates and the advantages over traditional methods from the cited MacLean meta-analysis. The mechanics of navigation/robotics, the Gertzbein- Robbins grading, the reduction in surgeon radiation, and the pitfalls (registration error, line-of-sight, skive, cost, learning curve, patient CT dose) are standard, well-established teaching. The formal appraisal showing that most of these associations rest on low to very low certainty evidence comes from the cited Li umbrella review, and the design and outcome measures of the awaited randomised comparison from the cited ROBARTHRODESE protocol. Triggered-EMG interpretation follows Spinal Cord Monitoring and IONM, which sets out why threshold cut-offs are quoted as local protocol rather than a single number. (See also Adolescent Idiopathic Scoliosis, Screw Biomechanics, CT Physics, Radiation Dose and Hounsfield Units and Radiation Safety in Orthopaedics.)