The Failed Carpal Tunnel Release (and Endoscopic Release)
- Carpal tunnel release is highly successful, but the index operation FAILS in about 5-10% of cases with reported REVISION rates of 0.3-7% (individual series report up to 20% persistent/recurrent and 12% revision) - so failure of the release is a recognised problem that must be analysed before re-operating, not simply 'done again'.
- There are THREE failure patterns and they have different causes: PERSISTENT (never resolved - usually an INCOMPLETE release, classically of the distal transverse carpal ligament or proximal antebrachial fascia, or a wrong/co-existing diagnosis); RECURRENT (resolved then returned after a symptom-free interval - usually PERINEURAL SCARRING/fibrosis or a reformed ligament); and NEW/IATROGENIC (a new deficit from injury to the median nerve or its recurrent motor or palmar cutaneous branch).
- The most important step before revision is to RE-CONFIRM the diagnosis and define the cause: a careful history/examination (was there ever relief? which symptoms persist? motor vs sensory? scar tenderness/Tinel's), ELECTRODIAGNOSTIC studies (comparison with pre-operative studies), IMAGING (ultrasound/MRI of the nerve and the canal for incomplete release, scarring, space-occupying lesions), and EXCLUSION of mimics (cervical radiculopathy, proximal median compression, peripheral neuropathy, thoracic outlet) - operating without a clear cause is a common error.
- PERSISTENT symptoms from a demonstrably INCOMPLETE release are the best candidates for revision and respond best - a COMPLETE re-release of the entire transverse carpal ligament (and antebrachial fascia) is performed, confirming full decompression under direct vision.
- For RECURRENT symptoms from PERINEURAL SCARRING, revision is a COMPLETE open re-release with EXTERNAL NEUROLYSIS (freeing the nerve from scar); to reduce re-scarring and to provide a healthy vascular bed, coverage/wrapping of the nerve may be added - options include local fat or muscle flaps (e.g. hypothenar fat pad, pronator quadratus) and vascularised soft-tissue flaps - and an internal neurolysis is generally avoided as it adds risk without benefit.
- The cardinal TECHNICAL rule of the revision operation is to IDENTIFY THE MEDIAN NERVE PROXIMALLY, in unoperated distal forearm proximal to the old scar, and then trace it DISTALLY into the scar - never to begin dissecting within the scar itself, where the nerve is tethered, displaced and has no reliable plane around it. Everything else about the revision follows from this: the incision is extended proximally, crossing the wrist crease obliquely towards the ulnar side (a straight transverse line contracts and a radial extension threatens the palmar cutaneous branch), the field is bloodless, and the approach is OPEN. The release must then be completed at BOTH ends under direct vision - the distal antebrachial fascia proximally, and distally to the true ligament edge where the palmar fat pad appears, with the superficial palmar arch immediately beyond.
- REHABILITATION after a revision is aimed at scar, because scar is what is being treated: EARLY active finger and nerve-gliding exercises within the first few days, plus scar massage and desensitisation - prolonged splinting allows the neurolysed nerve to re-adhere to the bed it was just freed from, defeating the operation.
- ENDOSCOPIC carpal tunnel release (single- or two-portal) gives a smaller scar and FASTER EARLY recovery (less pillar/scar pain, earlier return to work) with similar medium-term outcomes to open release, but it has a steeper learning curve and depends on good visualisation; in the REVISION setting, scarred/distorted anatomy makes OPEN release the safer choice, and any concern about completeness or nerve injury favours a direct open approach.
- “Classify the failed CTR: PERSISTENT (incomplete release / wrong diagnosis), RECURRENT (perineural scar after a symptom-free interval, conventionally at least ~3 months), or NEW/IATROGENIC (median or recurrent-motor/palmar-cutaneous branch injury). Failure 5-10%, revision 0.3-7%.
- “Before re-operating: re-confirm the diagnosis - history/exam, electrodiagnostics (vs pre-op), ultrasound/MRI, EXCLUDE mimics (cervical radiculopathy, proximal compression, polyneuropathy). Read the ORIGINAL OPERATIVE NOTE. Don't just 'release it again'.
- “Nerve conduction studies usually stay ABNORMAL after a successful release - a still-abnormal post-op study is expected, not proof of failure. Only the TREND against the pre-op study informs: improved-then-worse = recurrence; never changed = incomplete release or wrong diagnosis.
- “Technique: find the nerve PROXIMAL to the scar in unoperated forearm and trace it distally - never start inside the scar. Complete the release at BOTH ends (antebrachial fascia proximally, fat pad distally), EXTERNAL neurolysis only, hypothenar fat pad flap if the bed is scarred, then EARLY mobilisation.
- “Endoscopic = faster early recovery in PRIMARY cases (~6 days earlier return to work), same long-term outcome; contraindicated by previous surgery, a mass or synovitis, and distorted anatomy - revision is OPEN.
Persistent (never resolved - incomplete release/wrong diagnosis), recurrent (relief then return - perineural scar), or new/iatrogenic (median or recurrent-motor/palmar-cutaneous branch injury). Each needs a different response.
Re-confirm the diagnosis: history/exam, electrodiagnostics (vs pre-op), ultrasound/MRI, and exclude mimics (cervical radiculopathy, proximal compression, polyneuropathy). No clear cause = no revision.
The Three Patterns of Failure
- Time course
- Never resolved
- Usual cause
- Incomplete release (distal TCL/antebrachial fascia) or wrong/co-existing diagnosis
- Response
- Complete re-release (best candidates)
- Time course
- Resolved then returned
- Usual cause
- Perineural scarring/fibrosis; reformed ligament; new/progressive cause
- Response
- Complete re-release + external neurolysis +/- flap
- Time course
- New deficit after surgery
- Usual cause
- Median nerve / recurrent motor / palmar cutaneous branch injury; CRPS; pillar pain
- Response
- Depends on injury (exploration/repair); manage pain
The two commonest reasons a carpal tunnel release 'fails' are an incomplete release (the transverse carpal ligament not fully divided - classically distally, or the proximal antebrachial fascia left intact) and an incorrect or co-existing diagnosis (the symptoms were not, or not only, from carpal tunnel compression). Both are identified by a careful work-up rather than by re-operating blindly. Genuine recurrence after a symptom-free interval is usually perineural scarring, and a new deficit points to a nerve/branch injury.
The Surgical Anatomy Behind the Failure Modes
The distal transverse carpal ligament, the antebrachial fascia, the recurrent motor branch and the palmar cutaneous branch are the anatomical causes of failure - and it is the anatomy that makes each failure mode make sense (the basic anatomy is developed in Carpal Tunnel Syndrome and Median Nerve Anatomy).
- Where release is left incomplete. The transverse carpal ligament (flexor retinaculum) spans the carpal arch from the scaphoid tubercle/trapezium radially to the pisiform/hook of hamate ulnarly. The most commonly under-divided parts are the distal edge (toward the palm) and the proximal antebrachial fascia - leaving either gives persistent symptoms.
- The recurrent (thenar) motor branch (Lanz variants). It usually arises extraligamentously and recurs distal to the ligament, but in subligamentous and transligamentous variants it runs under or pierces the ligament - these are the variants at risk during division, and injury causes thenar motor loss (a new/iatrogenic failure).
- The palmar cutaneous branch. Arises about 5 cm proximal to the wrist crease and runs between palmaris longus and FCR to the thenar skin; an incision placed too radially or across the crease can injure it, producing a painful neuroma/numb scar.
- The superficial palmar arch lies just distal to the ligament's distal edge - the structure at risk when chasing a complete distal release, and a reason distal visualisation matters.
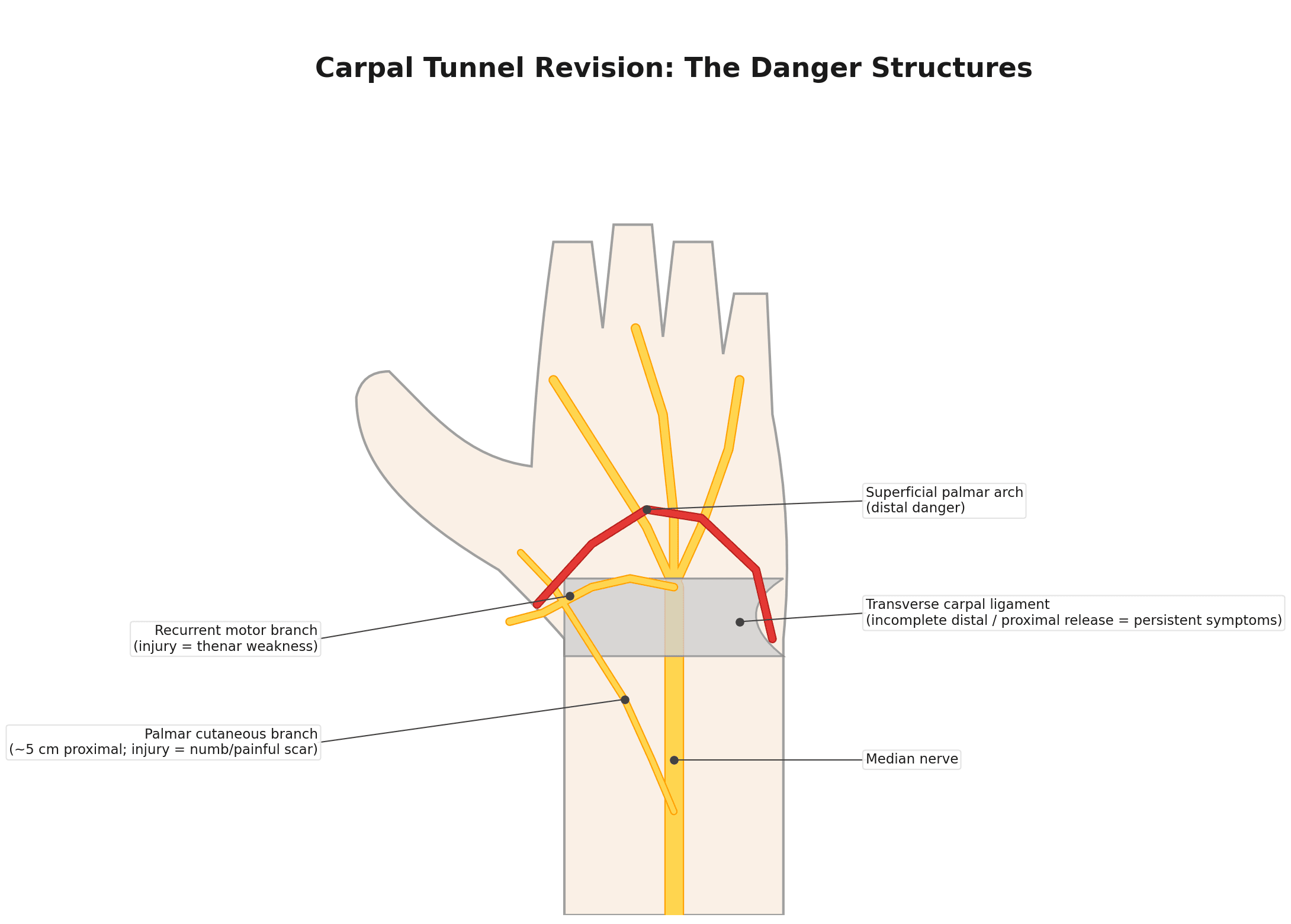
Map the failure to the anatomy: incomplete = under-divided distal TCL / proximal antebrachial fascia; iatrogenic motor = the sub-/transligamentous recurrent motor branch (Lanz); incision neuroma/numb scar = the palmar cutaneous branch (between PL and FCR, ~5 cm proximal to the crease); and the superficial palmar arch is the distal danger. This is why the revision field is approached open for direct visualisation.
The Revision Operation, Step by Step
Before the knife
- Obtain and read the original operative note. It states which approach was used, what was divided, what was seen and whether anything unexpected was found. A note describing a limited open or endoscopic release with no comment on the distal ligament edge raises the probability of an incomplete division; a note recording a normal-looking, fully decompressed nerve pushes the diagnosis back towards a mimic.
- Consent for the specific findings. Numbness in the palmar cutaneous distribution, a slower and initially more painful recovery than the first operation, the possibility that a flap will be raised, and the honest position that revision relieves symptoms less predictably than a primary release.
- Anaesthesia and tourniquet. Regional or general with an arm tourniquet; the field must be bloodless, because in scar the nerve is identified by texture and pattern rather than by colour contrast.
The incision
Extend the previous palmar incision proximally, keeping it ulnar to the thenar crease and in line with the radial border of the ring finger. Cross the wrist crease obliquely towards the ulnar side rather than as a straight transverse line - a straight line across a flexion crease contracts, and a radially placed extension runs directly onto the palmar cutaneous branch between palmaris longus and flexor carpi radialis. The proximal extension is not optional in a revision; it is what creates the unscarred territory the next step depends on.
In a revision the median nerve is tethered, displaced from its expected position and surrounded by tissue with no reliable surgical plane. Identify it proximal to the old scar in unoperated forearm, then follow it distally - this is the answer the examiner is listening for, and it is the reason the revision is done open and through an extended incision rather than endoscopically.
Prognostic Factors for Revision
- Best outcomes (revise with confidence). Persistent symptoms from a demonstrably incomplete release, with objective electrodiagnostic confirmation and a clear anatomical cause; or recurrent symptoms after a genuine symptom-free interval with scar on imaging - these have a definable, correctable problem.
- Poorer outcomes (be cautious). No prior relief at all with normal/unchanged electrodiagnostics (suggests the diagnosis was wrong), pure pain without nerve-compression signs, CRPS, an untreated proximal / double-crush component, established thenar wasting (incomplete motor recovery), and workers'-compensation/litigation contexts.
- Counsel on recovery. Even when revision works, expect higher early pain and a longer recovery than a primary release before reaching comparable symptom and function scores (per the cited propensity-matched data).
Revise the patient with a clear, correctable cause - incomplete release or scar plus objective electrodiagnostic/imaging confirmation and (ideally) a prior period of relief. Temper expectations where there was never any relief with normal studies, pure pain/CRPS, a double crush, or fixed thenar wasting. Always counsel that revision recovery is slower and initially more painful than the first operation.
Work-up of the Failed Release
- History/examination: was there ever relief (recurrent) or none (persistent)? Which symptoms persist (sensory vs motor/thenar wasting)? Scar tenderness, Tinel's/Phalen's, signs of a branch injury or CRPS.
- Electrodiagnostics: repeat nerve conduction/EMG and compare with pre-operative studies (improved then worsened vs never changed).
- Imaging: ultrasound/MRI of the nerve and canal - incomplete release, perineural scar, a reformed ligament, or a space-occupying lesion.
- Exclude mimics: cervical radiculopathy, proximal median compression (pronator/lacertus), peripheral polyneuropathy (e.g. diabetic), thoracic outlet - a 'double crush' may coexist.
What Each Result Actually Changes
Was there ever relief, and for how long? This one question does more work than any investigation, because it separates the two commonest patterns before anything is measured. Relief followed by return after a symptom-free interval of at least about three months is conventionally taken as recurrence, and points to scar. No meaningful relief at any point is persistence, and points to an incomplete release or to the wrong diagnosis. The three-month figure is a working convention rather than a validated threshold, and a very short interval sits awkwardly between the two - it is better recorded honestly than forced into a category.
Repeat nerve conduction studies are interpreted as a trend, not as a verdict. Standard median conduction parameters improve after a successful release but usually do not return to normal. In a prospective study of 35 patients undergoing carpal tunnel surgery, every electrophysiological parameter except conduction-velocity distribution improved significantly after surgery, yet most remained worse than in controls; only quantitative sensory testing fully returned to normal limits, with the residual signs attributed to incomplete recovery in the large fibres. So a post-operative study that is still abnormal is the expected finding after a technically good release and is not, by itself, evidence of failure. What is informative is the comparison with the pre-operative study: improved and then deteriorated supports recurrence, whereas unchanged from the outset supports either an incomplete release or a diagnosis that was never carpal tunnel compression. Studies reported without the pre-operative comparison should be treated as an incomplete investigation, not as a negative one.
A diagnostic corticosteroid injection remains useful after surgery. Meaningful, if temporary, relief from an injection into the canal (10-40 mg methylprednisolone, the same dose used in primary disease) indicates that the median nerve is still being compressed there and is one of the better predictors that a complete re-release will help. No response at all should prompt a serious reconsideration of the diagnosis before any second operation.
Not Every Failed Release Returns to Theatre
Where no correctable structural cause is demonstrated, the treatment is non-operative: a neutral night splint, hand therapy with nerve-gliding and scar desensitisation, neuropathic pain agents where the picture is predominantly painful, treating the mimic that has been uncovered (cervical radiculopathy, proximal median compression, diabetic polyneuropathy, thyroid disease), and specific management of complex regional pain syndrome if present. Pillar pain and scar tenderness after a primary release commonly settle over three to six months on their own, and a re-operation performed during that window is being asked to treat a problem that was going to resolve.
Revision Surgery & Endoscopic Release
- Complete open re-release: divide the entire transverse carpal ligament (and antebrachial fascia) under direct vision - the definitive treatment for an incomplete prior release.
- External neurolysis: free the nerve from perineural scar (the mainstay for recurrent disease); internal neurolysis is generally avoided (added risk, no proven benefit).
- Coverage/wrap for a scarred nerve: to provide a healthy vascular bed and reduce re-scarring - local fat or muscle flaps (hypothenar fat pad, pronator quadratus) or vascularised soft-tissue flaps.
- Address a branch injury appropriately (exploration/repair/grafting) and manage pain (including CRPS).
- Endoscopic vs open (primary): endoscopic release gives a smaller scar and faster early recovery (less pillar/scar pain, earlier return to work) with similar medium-term outcomes - but a steeper learning curve and reliance on visualisation; revision should be open because scarred/distorted anatomy makes endoscopy unsafe.
The cardinal error in managing a failed carpal tunnel release is to re-operate without first establishing why it failed. A revision aimed at the wrong problem will not help and adds the risks of scar and nerve injury. So the discipline is to classify the failure - persistent (was there ever relief?), recurrent (relief then return), or a new deficit (iatrogenic injury) - and to re-confirm the diagnosis with examination, electrodiagnostics compared with the pre-operative studies, and imaging, while actively excluding mimics such as cervical radiculopathy, proximal median compression and peripheral neuropathy. Persistent symptoms from a demonstrably incomplete release are the patients who benefit most from a complete re-release; recurrent symptoms from perineural scar are treated by re-release with external neurolysis and, where the nerve is heavily scarred, vascularised coverage; and a new deficit needs assessment for a nerve or branch injury. In the scarred revision field, choose an open approach over endoscopy for safe visualisation.
Endoscopic Release - What It Buys, and Where It Must Not Be Used
Endoscopic release divides the transverse carpal ligament from beneath through one portal at the distal wrist crease (single-portal, Agee) or through proximal and distal portals (two-portal, Chow), viewing the ligament from inside the canal. The gain is confined to the early period and is modest but real: less pillar and scar pain, grip strength recovering by around two weeks rather than six, and return to work earlier by a weighted mean of about six days (95% CI 3-9) in Cochrane's pooled analysis. Long-term symptom relief and success rates are the same as open release, around 90-95% by six to twelve months, so the choice is properly framed as a trade of early comfort against exposure - not as one technique being better.
The cost is that the ligament is divided without the nerve being inspected and without the canal contents being available to the surgeon's eye, along a learning curve of roughly 30-50 cases during which transient nerve injury is more frequent. That defines when it must not be used:
- Any previous carpal tunnel surgery - the reason revision is done open. Scar obliterates the plane the cannula is meant to pass through and displaces the nerve from where the endoscope expects it.
- A suspected mass or tenosynovitis needing biopsy or debulking - endoscopic release can divide the ligament but cannot address, or even see, what is in the canal.
- Distorted anatomy - previous distal radius or carpal fracture, severe wrist arthritis with osteophytes, a known bifid median nerve or persistent median artery.
- Inadequate visualisation at any point during the case. Failure to see the ligament clearly is an indication to convert to open, not to continue by feel; the ability to convert is part of consenting for the procedure.
Mnemonics & Memory Aids
REDO
Hook:REDO: Recognise the pattern, Electrodiagnostics + Exclude mimics, Define the cause, Open re-release + external neurolysis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient returns with hand symptoms after a carpal tunnel release. How do you work this up and decide on revision?”
“You have decided to revise. The patient had good relief for two years and the symptoms have returned; ultrasound shows the nerve encased in scar. Take me through the operation.”
Classify the failure
- Persistent: never resolved (incomplete release / wrong or co-existing diagnosis)
- Recurrent: relief then return (perineural scar / reformed ligament)
- New / iatrogenic: median or recurrent-motor/palmar-cutaneous branch injury; CRPS
Scale & work-up
- Failure 5-10%; revision 0.3-7% (up to 20%/12% in individual series)
- Re-confirm diagnosis: history/exam, original operative note, electrodiagnostics vs pre-op, ultrasound/MRI
- NCS usually stay abnormal after success - read the TREND, not the absolute value
- Exclude mimics: cervical radiculopathy, proximal median compression, polyneuropathy
- Diagnostic injection (10-40 mg methylprednisolone): relief predicts benefit from re-release
Revision technique
- Extend the incision proximally; cross the crease obliquely towards the ulnar side
- FIND THE NERVE PROXIMAL TO THE SCAR in unoperated forearm, then trace it distally
- Complete both ends: antebrachial fascia proximally, fat pad distally (arch beyond)
- External neurolysis ONLY - never internal neurolysis or epineurotomy
- Scarred bed -> hypothenar fat pad flap (protect Guyon's canal when raising it)
- Early nerve gliding and scar desensitisation - scar is the disease being treated
Endoscopic vs open
- Endoscopic (primary): return to work ~6 days earlier, same outcome by 6-12 months
- Learning curve 30-50 cases; the nerve is never inspected
- Contraindicated: previous surgery, mass/synovitis, distorted anatomy, bifid nerve
- Poor visualisation at any point -> CONVERT TO OPEN, do not proceed by feel
Evidence & Key Studies
Revision carpal tunnel release with external neurolysis versus primary release - a propensity-matched study
- Up to 20% of patients experience persistent or recurrent symptoms after carpal tunnel release, and up to 12% may require revision surgery.
- In a propensity-matched comparison, revision carpal tunnel release with external neurolysis achieved Boston Carpal Tunnel Questionnaire symptom and function scores comparable to primary release at follow-up, despite higher initial pain scores.
- Revision release with external neurolysis can effectively manage persistent or recurrent CTS, though patients may require a longer recovery period to reach outcomes similar to primary release.
Autologous nerve coverage in revision surgery for recurrent or persistent carpal tunnel syndrome - systematic review and meta-analysis
- Across the pooled literature, initial carpal tunnel surgery fails in about 5% to 10% of cases, with revision rates ranging from 0.3% to 7% - a lower and wider range than single-series figures.
- Twenty-six studies described eight different autologous nerve coverage techniques, but only two - the hypothenar fat pad flap and the synovial flap - could be compared directly.
- On random-effects meta-analysis both flaps were effective, with more patients achieving complete relief of symptoms, satisfaction and pain improvement in the hypothenar fat pad group.
Vascularised hypothenar fat pad flap in revision surgery for carpal tunnel syndrome
- Eighteen consecutive patients with recurrent CTS underwent median nerve decompression with a vascularised hypothenar fat pad flap, having had the index release 5 to 22 months earlier.
- At a mean of 22 months, 15 of 18 reported symptomatic improvement and 15 of 18 were satisfied; no patient was made worse and no recurrence was seen.
- Grip strength recovered to 90% of the contralateral side and median DASH was 18 - but 3 of 18 continued to struggle with pain and dysfunction, so a residual functional deficit should be part of the consent.
Which nerve fibres recover after carpal tunnel surgery - electrophysiological and quantitative sensory testing
- In 35 patients studied before and after carpal tunnel surgery, every electrophysiological parameter except conduction-velocity distribution improved significantly - yet most remained worse than in controls.
- Only quantitative sensory testing returned fully to normal limits; complete recovery was confined to small fibres, with residual signs attributed to the larger fibres.
- Clinical improvement occurred in 54.3% and was greater in less advanced disease, with patient age and CTS severity the important predictors of no improvement.
The pooled failure rate of the index release (about 5-10%) and the revision rate (0.3-7%), together with the head-to-head superiority of the hypothenar fat pad flap over the synovial flap, come from the cited Natroshvili systematic review and meta-analysis of 26 studies. The higher single-series figures - up to about 20% persistent/recurrent and 12% revision - and the finding that revision with external neurolysis reaches symptom and function scores comparable to primary release despite higher initial pain come from the cited Kim propensity-matched study; they are reported alongside the pooled range rather than in place of it, because a referred surgical cohort is enriched for difficult cases and the ceiling figure would mislead a candidate asked how often carpal tunnel release fails. The specific hypothenar fat pad flap outcomes (15 of 18 improved and satisfied, grip 90% of the contralateral side, median DASH 18, 3 of 18 with continuing pain) are Wichelhaus. The point that standard nerve conduction parameters improve but usually do not normalise after a successful release - which is why a still-abnormal post-operative study is not evidence of failure - is Koszewicz.
The corticosteroid dose (10-40 mg methylprednisolone), the endoscopic learning curve and contraindications, and the Cochrane return-to-work difference of about six days are taken in substance from Carpal Tunnel Syndrome, where they are set out for primary disease with their own sources; they apply unchanged here. The classification of failure (persistent vs recurrent vs new/iatrogenic), the work-up to re-confirm the diagnosis and exclude mimics, the proximal-to-distal dissection principle, the avoidance of internal neurolysis, and the technique of raising the hypothenar fat pad flap are standard, well-established teaching. The three-month symptom-free interval used to define recurrence is a working convention rather than a validated threshold, and is described as such.