Buerger's Disease
- Thromboangiitis obliterans (Buerger's disease) is a NON-ATHEROSCLEROTIC, SEGMENTAL, INFLAMMATORY occlusive disease of the SMALL and MEDIUM arteries and VEINS of the extremities; the occluding thrombus is highly cellular and inflammatory and characteristically spares the underlying vessel-wall architecture, distinguishing it from atherosclerosis and from a true necrotising vasculitis.
- It is strongly TRIGGERED by TOBACCO and occurs almost exclusively in SMOKERS, typically YOUNG adults (classically men, though increasingly women) with onset before about 45-50 years of age; substantial tobacco exposure is essential to the disease and its activity.
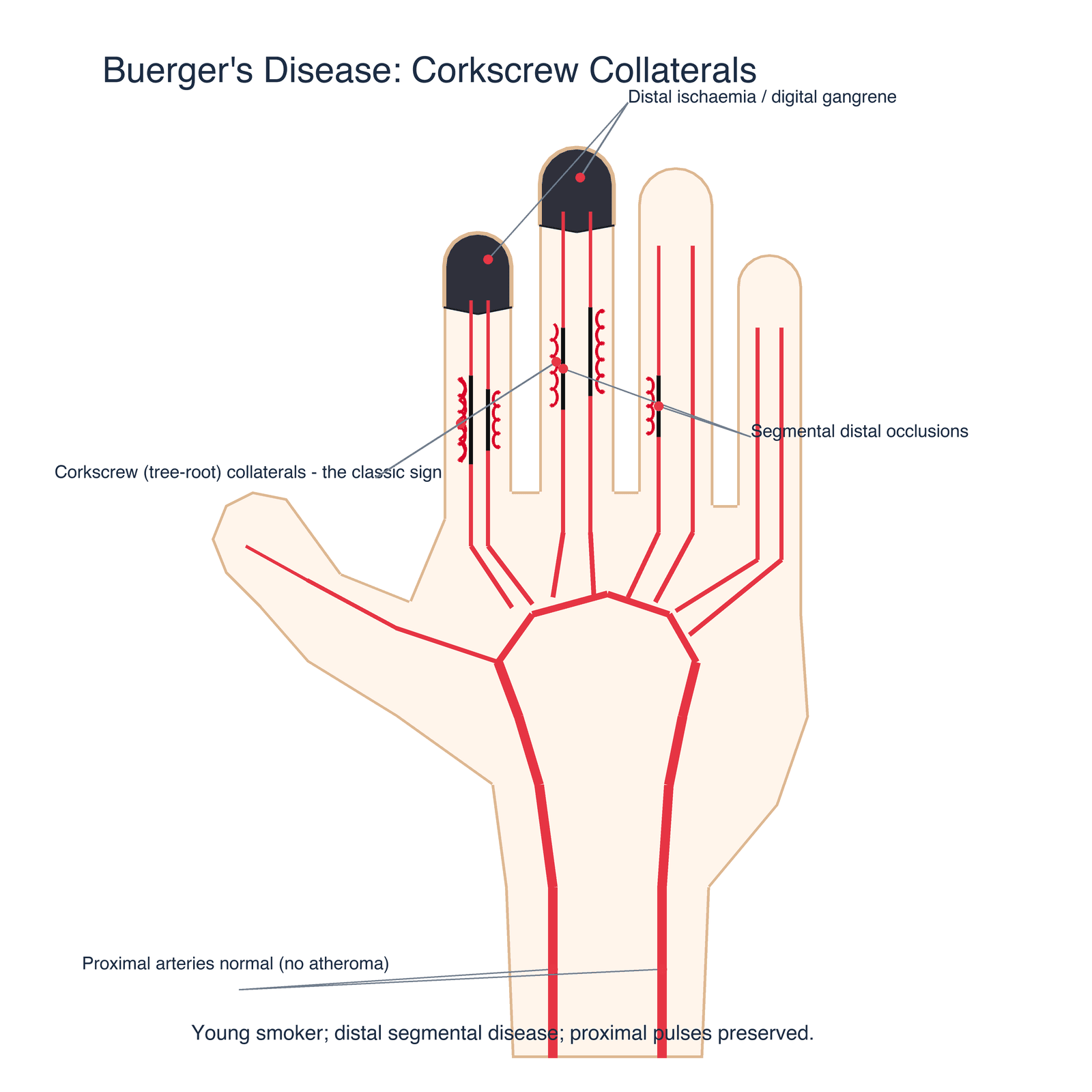
- It presents with DISTAL ischaemia - foot/instep or forearm/hand claudication, rest pain, and DIGITAL ULCERATION and GANGRENE of the fingers and toes - together with MIGRATORY SUPERFICIAL THROMBOPHLEBITIS and RAYNAUD'S phenomenon; the disease is distal and segmental, so proximal pulses are usually preserved while the digital vessels are occluded.
- DIAGNOSIS is essentially clinical and one of EXCLUSION: a young smoker with distal ischaemia, an absence of the usual atherosclerotic risk factors and embolic sources, normal proximal arteries, and CORKSCREW (tortuous 'tree-root') COLLATERALS around segmental occlusions on angiography; one must exclude atherosclerosis, diabetes, an embolic source (echo), autoimmune/connective-tissue disease (autoantibodies) and hypercoagulable states.
- The ONLY treatment that genuinely changes the course of the disease is COMPLETE and PERMANENT cessation of ALL tobacco - continued smoking drives progression and amputation, whereas stopping is associated with a significantly lower amputation rate; the honest framing is that it markedly reduces the risk of losing tissue rather than abolishing symptoms, since ex-smokers may still have claudication and rest pain. LIMB INFECTION at diagnosis is the dominant independent predictor of amputation (hazard ratio 12.1 in a 224-patient cohort), so treating infection early sits alongside cessation as the other thing that changes the outcome.
- REVASCULARISATION is of LIMITED value because the disease is distal and segmental with poor distal targets; surgical or endovascular revascularisation (including palmar-arch angioplasty in the hand) is reserved for selected cases with critical ischaemia and suitable anatomy and is a SUPPORTIVE limb-salvage measure rather than a cure - even with revascularisation MINOR amputations remain frequent, although major amputation can often be avoided; wound care, analgesia, and where appropriate vasodilators/prostanoids (e.g. iloprost) and sympathectomy are adjuncts.
- “Buerger's = young SMOKER + DISTAL ischaemia/digital gangrene + migratory superficial thrombophlebitis + Raynaud's. Non-atherosclerotic, segmental, small/medium arteries AND veins; thrombus spares the vessel wall.
- “Diagnosis = exclusion + CORKSCREW collaterals on angiography; normal proximal arteries; exclude emboli/atheroma/diabetes/autoimmune/hypercoagulable.
- “ONLY disease-modifying treatment = total smoking cessation - it markedly lowers amputation but does not reliably abolish symptoms. LIMB INFECTION at diagnosis is the dominant amputation risk (HR 12.1). Revascularisation limited (distal disease, poor targets) - supportive limb salvage. Amputation in about 21% at mean 5.7 years, roughly a third by 15 years; mortality only 1.4%.
Young smoker with distal ischaemia, digital ulcers/gangrene, migratory superficial thrombophlebitis and Raynaud's - non-atherosclerotic, small/medium arteries and veins, normal proximal arteries, corkscrew collaterals on angiography.
Complete, permanent smoking cessation is the only treatment that changes the disease. Revascularisation is limited (distal, poor targets). Continued smoking = progression and amputation.
Pathology & Presentation
Buerger's disease is a non-atherosclerotic, segmental, inflammatory occlusive disease of the small and medium arteries and veins of the extremities. The occluding thrombus is highly cellular and inflammatory and characteristically spares the vessel-wall architecture, which distinguishes it from atherosclerosis and from a destructive necrotising vasculitis. It occurs almost exclusively in smokers, typically young adults with onset before about 45-50. It presents with distal ischaemia - instep/forearm claudication, rest pain, digital ulceration and gangrene - and with migratory superficial thrombophlebitis and Raynaud's phenomenon. Because it is distal and segmental, proximal pulses are usually preserved while the digital arteries are occluded.
Histopathology: the Inflammatory, Wall-Sparing Thrombus
- Acute phase. An occlusive, highly cellular inflammatory thrombus with characteristic intraluminal microabscesses (neutrophil collections) and multinucleated giant cells; the inflammation involves all wall layers, but the internal elastic lamina and the overall vessel-wall architecture are preserved - the pathognomonic wall-sparing feature that separates it from atherosclerosis and from a destructive necrotising vasculitis.
- Subacute (intermediate) phase. Progressive organisation of the thrombus with persistent but less florid inflammation.
- Chronic (end-stage) phase. An organised, recanalised thrombus with perivascular fibrosis; the appearance becomes non-specific and indistinguishable from other end-stage vasculopathy.
- Why biopsy is rarely done. The diagnostic microabscess/giant-cell features are seen only in the acute phase, and excising an artery from an already-ischaemic limb risks the limb - so the diagnosis stays clinical/angiographic, not histological.
Acute Buerger's = an inflammatory occlusive thrombus with microabscesses and giant cells that spares the vessel wall (internal elastic lamina intact) - the feature distinguishing it from atherosclerosis and necrotising vasculitis. Later phases organise and recanalise and become non-specific, so biopsy (which would also threaten the ischaemic limb) is rarely performed - the diagnosis is clinical and angiographic.
Diagnosis - A Clinical Diagnosis of Exclusion
There is no single confirmatory test; the diagnosis is clinical and one of exclusion:
- Typical patient/picture: young smoker, distal ischaemia, digital ulcers/gangrene, thrombophlebitis, Raynaud's; onset before ~45-50.
- Angiography: segmental occlusions of distal vessels with corkscrew (tortuous 'tree-root') collaterals and normal proximal arteries (no atheroma).
- Exclude: atherosclerosis and its risk factors, diabetes, an embolic source (echocardiography, proximal aneurysm), autoimmune/connective-tissue disease (autoantibodies, inflammatory markers) and hypercoagulable states.
- Allen's test is often abnormal (involvement of both forearm arteries / palmar arch).
Formal Diagnostic Criteria (Shionoya / Olin)
- Shionoya's criteria (five). (1) a smoking history; (2) onset before age 50; (3) infrapopliteal arterial occlusive disease; (4) either upper-limb involvement or migratory phlebitis; and (5) absence of atherosclerotic risk factors other than smoking. Meeting all five supports the diagnosis.
- Olin's clinical (exclusion-based) approach. A young current/recent tobacco user with distal-extremity ischaemia (claudication, rest pain, ulcers or gangrene) confirmed non-invasively, consistent arteriography, and exclusion of autoimmune/connective-tissue disease, a hypercoagulable state, diabetes and a proximal embolic source (echocardiography/proximal imaging).
- Both formalise the same idea: the right patient and distal pattern plus rigorous exclusion of the mimics.
Quote a set: Shionoya = smoking + onset under 50 + infrapopliteal occlusion + (upper-limb involvement OR migratory phlebitis) + no atherosclerotic risk factors besides smoking. Olin = young smoker + distal ischaemia + consistent arteriography + exclusion of autoimmune/hypercoagulable/diabetes/embolic source. There is no single confirmatory test - it is criteria plus exclusion.
Management
- Complete, permanent smoking cessation - the only disease-modifying treatment; deliver the message unambiguously and support it actively (counselling, pharmacotherapy). Continued tobacco drives progression and amputation; stopping significantly lowers the amputation rate, though symptoms may persist.
- Treat limb infection early and aggressively - infection at diagnosis carried a hazard ratio of 12.1 for amputation, the largest single factor measured, so an infected ischaemic digit warrants prompt antimicrobial therapy and debridement rather than watchful wound care.
- Wound and limb care: meticulous foot/hand care, analgesia for ischaemic rest pain.
- Pharmacological adjuncts: vasodilators and prostanoids (e.g. iloprost) may help ischaemic rest pain and ulcer healing; address pain (including for ulcers/gangrene).
- Revascularisation - limited: the distal, segmental pattern gives poor distal targets, so surgical or endovascular revascularisation (including palmar-arch angioplasty in the hand) is reserved for selected critical ischaemia with suitable anatomy and is a supportive limb-salvage measure, not a cure - minor amputations remain frequent even after revascularisation, but major amputation can often be avoided.
- Sympathectomy and other adjuncts have a limited, selective role.
- Amputation: the most distal level that will heal, for established gangrene/intractable pain - far more likely if the patient continues to smoke.
The defining clinical truth of Buerger's disease is that it is a tobacco-driven disease and that complete, permanent cessation of all tobacco is the only intervention that changes its natural history. Revascularisation, prostanoids, sympathectomy and wound care are supportive and, because the disease is distal and segmental with poor targets, revascularisation often fails or only delays tissue loss - minor amputations were still needed in most of the nine patients in the small upper-limb series reported, though none lost a limb. A patient who continues to smoke will progress to further ulceration, gangrene and amputation regardless of any procedure, whereas one who stops has a significantly lower amputation risk and can frequently avoid major amputation - even though about a fifth of all patients still come to amputation by a mean of under six years. Therefore the central, non-negotiable management step - to be delivered clearly and supported actively - is total smoking cessation, alongside prompt treatment of any limb infection, and no operative plan should be framed as a substitute for either.
What Actually Happens Over Time - and What Drives Amputation
Telling a patient that stopping tobacco "arrests the disease" is the right message delivered slightly too absolutely. The largest long-term series puts numbers to both halves of the truth.
In a multicentre retrospective cohort of 224 patients (median age at diagnosis 38.5 years, 23.8 percent female, mean follow-up 5.7 years) a vascular event occurred in 58.9 percent and an amputation in 21.4 percent. Amputation-free survival was 85 percent at 5 years, 74 percent at 10 and 66 percent at 15 - so roughly a third of patients will lose tissue within 15 years of diagnosis. Mortality, by contrast, was only 1.4 percent: this is a disease that takes digits and limbs, not usually life.
The strongest independent factor for amputation in that cohort was limb infection at diagnosis (hazard ratio 12.1, 95 percent CI 3.5 to 42.1) - far larger than anything else measured. Non-white ethnicity predicted vascular events (hazard ratio 2.35). Patients who stopped tobacco had a significantly lower amputation risk than those who continued. So the two things that change the outcome are stopping tobacco and treating infection early and aggressively - and an infected ischaemic digit is not a wound-care problem to review in a fortnight.
Cessation is still the only intervention that changes the disease, and it is worth every effort - but the honest framing is that it substantially reduces the risk of amputation, not that it stops the illness dead. In a separate long-term series of Buerger's patients followed by questionnaire, the amputation rate was higher in current smokers than in ex-smokers, yet there was no significant difference in the persistence of symptoms between the two groups - so an ex-smoker may still have claudication, Raynaud's and rest pain even though the limb is far more likely to be saved. Counselling that promises the symptoms will disappear sets the patient up to feel that quitting failed, which is the last thing that helps them stay stopped.
Numbers worth carrying: amputation in about one in five at a mean of 5.7 years and about a third by 15 years; limb infection at diagnosis is the dominant amputation risk (hazard ratio 12.1); mortality is low (1.4 percent). Stopping tobacco lowers amputation significantly but does not reliably abolish symptoms.
Mnemonics & Memory Aids
BUERGER
Hook:BUERGER: Blokes who smoke, Ulcers/gangrene, Extremity small vessels, Raynaud's/phlebitis, Gangrene if they keep smoking, Exclusion + corkscrew collaterals, Renounce tobacco.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old man who smokes presents with painful ulceration and early gangrene of two fingertips and a tender cord on his forearm. What is your diagnosis and management?”
What it is
- Non-atherosclerotic, segmental, inflammatory occlusion of small/medium arteries AND veins
- Inflammatory thrombus that spares the vessel-wall architecture
- Strongly tobacco-driven; young adults (classically male)
Presentation
- Distal ischaemia: instep/forearm claudication, rest pain, digital ulcers/gangrene
- Migratory superficial thrombophlebitis; Raynaud's phenomenon
- Proximal pulses usually preserved (distal/segmental disease)
Diagnosis
- Clinical diagnosis of exclusion; abnormal Allen's test common
- Angiography: corkscrew collaterals, normal proximal arteries (no atheroma)
- Exclude atheroma/diabetes/emboli/autoimmune/hypercoagulable
Management
- Complete permanent smoking cessation - the ONLY disease-modifying treatment (lowers amputation; may not abolish symptoms)
- Treat limb infection early - hazard ratio 12.1 for amputation, the dominant risk factor
- Wound care, analgesia, prostanoids (iloprost) for rest pain/ulcers
- Revascularisation limited/supportive; amputate distal-most level that heals
- Outcome: amputation 21.4% at mean 5.7 yrs, about 34% by 15 yrs; mortality 1.4%
Evidence & Key Studies
Buerger disease (thromboangiitis obliterans) - clinical features, diagnosis and management
- Buerger disease is a non-atherosclerotic vasculitis triggered by substantial exposure to tobacco, usually affecting the small and medium arteries of the upper and lower extremities.
- The review sets out the clinical presentation, diagnostic criteria and work-up (non-invasive arterial studies and angiography, with typical distal findings).
- Management centres on smoking cessation, with revascularisation - surgical and endovascular - having a limited, selective role.
Endovascular revascularisation of upper-limb thromboangiitis obliterans via palmar-arch angioplasty
- In nine men with angiographically confirmed upper-extremity TAO (all active smokers), the radial artery was involved in all and the ulnar in most, with digital gangrene or ischaemic ulceration at presentation.
- Palmar-arch angioplasty was technically successful in 4 of 6 attempts; minor amputations occurred in 88.9% but no major amputations were required, and successful revascularisation improved wound healing and limb salvage.
- Endovascular revascularisation is a feasible supportive limb-salvage measure in selected patients rather than a definitive solution - outcomes remain variable and minor amputations are still frequent.
Long-term outcome and prognostic factors in 224 patients: limb infection dominates amputation risk
- Retrospective multicentre cohort of 224 patients meeting Papa's criteria; median age at diagnosis 38.5 years, 23.8 percent female, 81.7 percent white, mean follow-up 5.7 years.
- Vascular events occurred in 58.9 percent, amputation in 21.4 percent and death in only 1.4 percent.
- Amputation-free survival was 85 percent at 5 years, 74 percent at 10 and 66 percent at 15 - about a third of patients undergo amputation within 15 years of diagnosis.
- Limb infection at diagnosis was the dominant independent risk factor for amputation (hazard ratio 12.1, 95 percent CI 3.5 to 42.1); non-white ethnicity predicted vascular events (hazard ratio 2.35).
- Patients who stopped tobacco had a significantly lower risk of amputation than those who continued.
- Retrospective design, and the cohort was predominantly white and European, unlike most published series which come from India and Japan - so the ethnicity finding in particular should not be read as a biological rule.
The nature of Buerger's disease (a non-atherosclerotic, tobacco-triggered vasculitis of the small/medium arteries of the extremities), its diagnostic work-up, and the central role of smoking cessation with a limited role for revascularisation come from the cited Del Conde review; the limits of revascularisation in the upper limb (frequent minor amputations, major amputation often avoidable) from the cited Varim series. The classic clinical picture (young smoker, distal ischaemia, migratory thrombophlebitis, Raynaud's, corkscrew collaterals) is standard, well-established teaching. The long-term amputation figures, the amputation-free survival curve and the dominance of limb infection as a risk factor come from the cited Le Joncour multicentre cohort; the observation that ex-smokers still had persistent symptoms although a lower amputation rate is from Shigematsu and Shigematsu (Int Angiol 1999, PMID 10392482), a postal-questionnaire follow-up of 287 responders from an original 682 patients, so it carries substantial responder bias. The Varim upper-limb figures come from only nine patients with six angioplasty attempts - the 88.9 percent minor-amputation figure is therefore a single small-series signal, not a general rate, and should not be quoted to a patient as their personal risk. No trial was found comparing prostanoid regimens head to head in this disease, and no agreed dose schedule specific to Buerger's was retrieved, so iloprost is named without a dose here; prescribe to local formulary. See also Raynaud's phenomenon of the hand, hypothenar hammer syndrome, vasculitides of orthopaedic relevance and smoking cessation.