The Wrist Extensor Tendons Beneath the Extensor Retinaculum
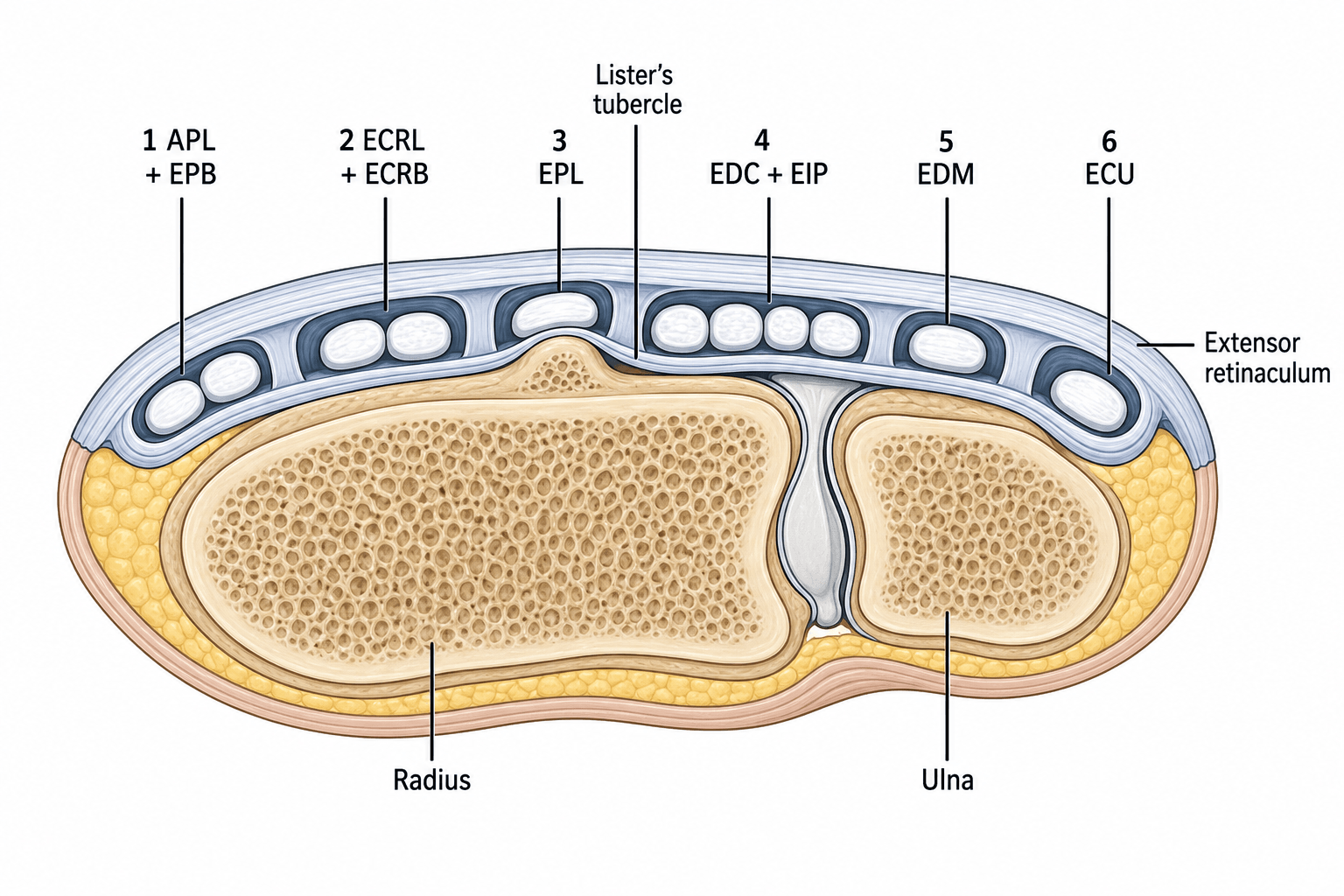
- On the dorsum of the wrist the extensor tendons pass beneath the EXTENSOR RETINACULUM, which sends septa to the radius and ulna dividing the space into SIX osseofibrous DORSAL COMPARTMENTS, numbered 1 to 6 from RADIAL to ULNAR; the retinaculum holds the tendons down (prevents bowstringing) while allowing them to glide.
- The contents in order are: (1) ABDUCTOR POLLICIS LONGUS + EXTENSOR POLLICIS BREVIS; (2) EXTENSOR CARPI RADIALIS LONGUS + BREVIS; (3) EXTENSOR POLLICIS LONGUS; (4) EXTENSOR DIGITORUM COMMUNIS + EXTENSOR INDICIS PROPRIUS; (5) EXTENSOR DIGITI MINIMI; (6) EXTENSOR CARPI ULNARIS.
- LISTER'S TUBERCLE on the dorsal distal radius is the landmark: compartment 2 lies radial to it and compartment 3 (EPL) lies ulnar to it, using the tubercle as a PULLEY that turns the EPL toward the thumb - this turn plus a watershed blood supply makes the EPL vulnerable.
- COMPARTMENT 1 is the site of DE QUERVAIN'S tenosynovitis (APL/EPB); an INTRACOMPARTMENTAL SEPTUM separating APL from EPB is common and is more frequent in the de Quervain's surgical population than in general cadaveric series (67 percent versus 35 percent in a systematic review), and is a recognised cause of failed conservative treatment / failed release.
- EPL RUPTURE (compartment 3) is a classic delayed complication of a NON-DISPLACED distal radius fracture (attrition/ischaemia at the watershed around Lister's tubercle) and of rheumatoid arthritis; because the tendon end retracts it is usually reconstructed with an EIP-to-EPL TENDON TRANSFER rather than direct repair.
- The relations matter surgically: the POSTERIOR INTEROSSEOUS NERVE lies on the FLOOR OF THE FOURTH COMPARTMENT (target for dorsal wrist denervation, and at risk in dorsal approaches); the EDM of compartment 5 over the DRUJ is the first to rupture in rheumatoid (Vaughan-Jackson syndrome); and the ECU subsheath of compartment 6 stabilises the ECU, whose instability causes painful ulnar-sided snapping.
- “Order radial->ulnar: 1 APL/EPB, 2 ECRL/ECRB, 3 EPL, 4 EDC/EIP, 5 EDM, 6 ECU (mnemonic below).
- “Lister's tubercle = pulley for EPL (compartment 3 is ulnar to it); EPL ruptures at this watershed after a non-displaced distal radius fracture -> EIP-to-EPL transfer.
- “Compartment 1 = de Quervain's; a septum (APL/EPB) causes failed conservative/operative treatment - look for and release it.
1: APL + EPB (de Quervain's) - 2: ECRL + ECRB (intersection syndrome at the crossover) - 3: EPL (around Lister's tubercle, watershed rupture).
4: EDC + EIP (PIN on its floor) - 5: EDM (over the DRUJ, Vaughan-Jackson) - 6: ECU (own ulnar groove; subsheath instability).
The Anatomy
The extensor retinaculum is a thickening of the deep antebrachial fascia over the dorsum of the wrist. It attaches radially to the lateral margin of the radius and ulnarly to the triquetrum and pisiform (and loosely to the ulnar styloid), and sends septa down to the dorsal ridges of the radius and ulna. These septa create six osseofibrous compartments, each lined by synovium, through which the extensor tendons glide. Functionally the retinaculum prevents bowstringing of the extensor tendons during wrist and finger extension while still permitting smooth excursion. The compartments are numbered 1 to 6 from the RADIAL (thumb) side to the ULNAR side.
- Contents
- APL + EPB
- Key relation / landmark
- Radial styloid; often septated
- Classic pathology
- De Quervain's tenosynovitis
- Contents
- ECRL + ECRB
- Key relation / landmark
- Radial to Lister's tubercle
- Classic pathology
- Intersection syndrome (crossover with comp 1)
- Contents
- EPL
- Key relation / landmark
- Hooks around Lister's tubercle (pulley)
- Classic pathology
- EPL rupture (distal radius #, RA) -> EIP transfer
- Contents
- EDC + EIP
- Key relation / landmark
- PIN on the compartment floor
- Classic pathology
- Dorsal wrist denervation; EIP transfer donor
- Contents
- EDM
- Key relation / landmark
- Overlies the DRUJ
- Classic pathology
- Vaughan-Jackson (first rupture in RA)
- Contents
- ECU
- Key relation / landmark
- Own groove on dorsal ulnar head; subsheath
- Classic pathology
- ECU instability/subluxation; ulnar wrist pain
Surface Anatomy: the Snuffbox & Palpating the Compartments
Compartments 1 and 3 are not only listed - they are the two borders of the anatomical snuffbox, which is where both are examined at the bedside.
- Borders of the snuffbox. The volar (radial) border is compartment 1 - abductor pollicis longus and extensor pollicis brevis; the dorsal (ulnar) border is compartment 3 - extensor pollicis longus (turning around Lister's tubercle toward the thumb). The floor is the scaphoid and trapezium, and the proximal apex is the radial styloid.
- What crosses it. The radial artery runs across the floor of the snuffbox (pulse palpable here), the cephalic vein begins over it, and branches of the superficial radial nerve cross the roof and compartment 1 - so the nerve is at risk in de Quervain's release and gives the dorsal radial sensory numbness of Wartenberg's (cheiralgia paraesthetica) syndrome.
- Using it clinically. Tenderness in the snuffbox is the classic sign of a scaphoid fracture; pain along the volar border on a thumb-tuck (Finkelstein/Eichhoff) points to compartment 1 / de Quervain's; and loss of the EPL dorsal border with absent thumb retropulsion signals EPL rupture.
- Palpating the rest. Lister's tubercle is the palpable dorsal ridge that separates compartment 2 (radial) from compartment 3 (ulnar); the extensor carpi ulnaris (compartment 6) is felt in its groove on the dorsal ulnar head and tested for snapping in forearm rotation.
The work-up behind each of those signs sits in scaphoid fractures, de Quervain's tenosynovitis, extensor pollicis longus rupture, Wartenberg's syndrome and snapping ECU instability.
The anatomical snuffbox is bounded by compartment 1 (APL + EPB) volarly and compartment 3 (EPL) dorsally, floored by the scaphoid/trapezium, with the radial artery crossing and the superficial radial nerve over the roof. Snuffbox tenderness = scaphoid fracture; the same nerve is the one injured in de Quervain's release and irritated in Wartenberg's syndrome.
Anatomical Variations of the Dorsal Compartments
The dorsal compartments are among the most variable regions in the body, and the variations are examinable because they cause failed surgery, complicate transfer planning, and present as dorsal masses.
- Compartment 1. Besides the intracompartmental septum, the abductor pollicis longus commonly has multiple slips - typically two to four (inserting variably on the trapezium and thenar fascia), and the extensor pollicis brevis may be absent or have its own sub-sheath - all relevant to recognising and fully releasing de Quervain's.
- Compartment 4. The extensor indicis proprius is the usual EPL transfer donor, but accessory extensors exist - an extensor medii proprius (to the middle finger) or extensor indicis et medii communis - and the EIP is rarely absent; the surgeon must therefore confirm independent index extension before harvesting it. The extensor digitorum brevis manus, an accessory muscle belly arising in the fourth compartment, presents as a soft dorsal wrist swelling that is mistaken for a ganglion or tenosynovitis.
- Compartment 5. The extensor digiti minimi is frequently double (two slips), useful to know when assessing little-finger extension and in Vaughan-Jackson ruptures.
- Why it matters. These variants explain a proportion of failed de Quervain's releases (an unreleased EPB sub-sheath), influence tendon-transfer donor choice (confirm an independent donor and a remaining motor to the index/little finger), and account for benign dorsal masses (extensor digitorum brevis manus). Donor selection is developed in tendon transfers for nerve palsy.
The "2,2,1,2,1,1" count is the default, not a rule: APL usually has two to four slips, EPB may have its own sub-sheath or be absent (failed de Quervain's release), EDM is often double, and accessory extensors (extensor medii proprius, extensor digitorum brevis manus) exist - so always confirm an independent index extensor before harvesting EIP, and remember the brevis manus as a cause of a dorsal wrist lump.
High-Yield Clinical Correlations
De Quervain's tenosynovitis is stenosing tenosynovitis of the first dorsal compartment (APL and EPB), causing radial-sided wrist pain reproduced by Finkelstein's / Eichhoff's test. A key surgical point is the frequent intracompartmental SEPTUM that creates a separate sub-sheath for the EPB: if it is not recognised, a corticosteroid injection or a surgical release that only opens the APL sub-sheath fails. A septum was found in 67 percent of the de Quervain surgical population against 35 percent of general cadaveric series in a systematic review and meta-analysis - so in the patient in front of you who has already failed an injection, a separate EPB sub-sheath is more likely than not. Recognising and releasing all sub-compartments is essential; the condition itself is set out in de Quervain's tenosynovitis, and the proximal crossover in intersection syndrome.
The extensor pollicis longus runs in the third compartment and makes a sharp turn around Lister's tubercle, which acts as its pulley. The segment around the tubercle has a relatively avascular watershed, so the EPL is vulnerable to attritional/ischaemic rupture - classically a delayed complication of a NON-DISPLACED distal radius fracture (the intact dorsal cortex and haematoma compromise the tendon), and also in rheumatoid arthritis and after volar plating with prominent dorsal screws. Because the ruptured ends retract and fray, direct repair usually fails, so the standard reconstruction is an extensor indicis proprius (EIP) to EPL tendon transfer.
- Compartment 4 (EDC + EIP): the posterior interosseous nerve lies on its floor - the target for dorsal wrist denervation, and at risk in dorsal exposures. The EIP (which lies ulnar and deep to the EDC of the index) is the standard donor for EPL reconstruction.
- Compartment 5 (EDM): overlies the DRUJ; in rheumatoid arthritis a dorsally subluxed, eroded ulnar head ruptures the ulnar-sided extensors first - the Vaughan-Jackson sequence (EDM/EDC little then ring finger).
- Compartment 6 (ECU): the ECU sits in its own groove on the ulnar head within a subsheath; disruption of the subsheath causes ECU instability/subluxation and painful ulnar-sided snapping on forearm rotation.
Mnemonics & Memory Aids
2-2-1-2-1-1
Hook:Tendon count radial->ulnar = 2,2,1,2,1,1 - get the counts and the contents follow.
LISTER
Hook:Find Lister's tubercle and you have located compartments 2, 3 and the EPL watershed.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Name the six dorsal extensor compartments of the wrist in order and their contents, and tell me the clinical relevance of each.”
“A patient develops inability to lift the thumb off the table (retropulsion) six weeks after a non-displaced distal radius fracture treated in a cast. What has happened, why, and how would you manage it?”
Contents (radial -> ulnar)
- 1: APL + EPB | 2: ECRL + ECRB | 3: EPL
- 4: EDC + EIP | 5: EDM | 6: ECU
- Tendon counts: 2,2,1,2,1,1
Landmarks & relations
- Lister's tubercle: comp 2 radial, comp 3 (EPL) ulnar - EPL pulley
- PIN on floor of compartment 4 (dorsal denervation; at risk in dorsal approaches)
- EDM (comp 5) overlies the DRUJ; ECU (comp 6) in its own groove + subsheath
Pathology by compartment
- 1: De Quervain's (look for the septum) | 1+2: intersection syndrome
- 3: EPL rupture (non-displaced distal radius #, RA) -> EIP-to-EPL transfer
- 5: Vaughan-Jackson (first RA rupture) | 6: ECU instability
EPL rupture quick facts
- Sign: loss of thumb retropulsion (lift off table)
- Incidence after distal radius fracture ~0.07-5%; watershed at Lister's tubercle
- Reconstruct with EIP-to-EPL transfer (confirm independent index extension)
Evidence & Key Studies
Ultrasonography and surgical anatomy in de Quervain disease: a systematic review and meta-analysis
- An intercompartmental SEPTUM in the first dorsal compartment was significantly more common in the de Quervain surgical population than in the general cadaveric population (67% vs 35%).
- Ultrasound-guided corticosteroid injections were more accurate than blind/manual injections (90-100% vs 40-100%) and gave significantly better outcomes.
- Recognising first-compartment anatomical variation (the septum) is prognostically important and helps explain failure of conservative treatment and incomplete surgical release.
Ruptured extensor pollicis longus tendon after a nondisplaced distal radius fracture
- Delayed EPL rupture is a recognised complication of distal radius fracture, with a reported incidence ranging from 0.07% to 5%.
- In adults it is seen more often after NON-DISPLACED fractures (attrition/ischaemia at the third-compartment watershed around Lister's tubercle), whereas in children it follows displaced/unstable fractures requiring fixation.
- Management of complete rupture is typically tendon transfer (EIP to EPL) rather than direct repair.
The first-compartment septum prevalence and ultrasound data come from the cited Abi-Rafeh meta-analysis, and the EPL-rupture incidence/association with non-displaced distal radius fractures from the cited Bogart and Vidlock report - a single case report, so the 0.07 to 5 percent range is a figure it quotes from the wider literature rather than one it measured, and the quoted span is wide enough that it should be given as an order of magnitude rather than a precise risk when consenting. The compartment numbering and tendon contents are standard, universally established anatomy. The anatomical variants (abductor pollicis longus slips, accessory extensors, extensor digitorum brevis manus, double extensor digiti minimi) are established descriptive anatomy; no series was found giving the proportion of failed de Quervain releases attributable specifically to an unreleased extensor pollicis brevis sub-sheath, so no such figure is quoted. See also de Quervain's tenosynovitis, intersection syndrome, extensor pollicis longus rupture, distal radius fractures, snapping ECU instability and rheumatoid arthritis of the hand.