Hip & Knee
- Vascular injury is a RARE but potentially LIMB- and LIFE-THREATENING complication of hip and knee arthroplasty - arterial injury occurred in 0.08 percent of 41,633 arthroplasties (0.08 percent primary TKA, 0.04 percent primary THA), rising to about 0.2 percent for REVISION of either joint, which was the one factor independently predicting it (odds ratio 2.7). Because it is uncommon, a high index of suspicion and a low threshold for vascular imaging and specialist involvement are essential.
- In TOTAL KNEE ARTHROPLASTY the vessel at risk is the POPLITEAL ARTERY, which lies just posterior to the knee; it can be injured by DIRECT laceration (during posterior capsular release/cuts, osteophyte excision, or with a posterior retractor), and - importantly - by TOURNIQUET-related ischaemia, in which a tourniquet in a patient with PERIPHERAL ARTERIAL DISEASE or a heavily calcified/atherosclerotic popliteal artery causes plaque disruption, thrombosis or embolism (so assess for PAD preoperatively and use the tourniquet judiciously or avoid it).
- ANATOMIC VARIANTS increase the popliteal artery's vulnerability in TKA: a HIGH popliteal bifurcation and an aberrant/anteriorly-positioned ANTERIOR TIBIAL ARTERY (aberrant ATA prevalence around 0.4-6%) bring the artery closer to the operative field, especially in women, so awareness of variants and selective preoperative vascular imaging (reviewing any existing MRI) may reduce risk.
- In TOTAL HIP ARTHROPLASTY the EXTERNAL ILIAC, common femoral and profunda femoris vessels are at risk; the classic mechanism is ACETABULAR SCREW placement - the ANTERIOR acetabular 'quadrants' (the anterosuperior and anteroinferior quadrants) are dangerous because the external iliac and obturator vessels lie there, so screws are placed in the safe POSTERIOR (posterosuperior/posteroinferior) quadrants; other mechanisms are retractor placement (corona mortis), cement extrusion, and revision/protrusio surgery with intrapelvic components.
- PRESENTATION is either ACUTE - intra-operative or early haemorrhage, an absent distal pulse, an ischaemic/pale-cool limb, or an expanding haematoma - or DELAYED, as a PSEUDOANEURYSM or an ARTERIOVENOUS FISTULA presenting weeks to years later (with swelling, a pulsatile mass, a bruit, or distal ischaemia); a tourniquet can mask intra-operative bleeding until it is released, so the limb perfusion must be checked after deflation.
- MANAGEMENT is an EMERGENCY: involve VASCULAR SURGERY urgently, obtain CT ANGIOGRAPHY (or on-table angiography) when the limb is not critically ischaemic, and treat by direct REPAIR or BYPASS or by ENDOVASCULAR means (a covered stent, particularly effective for pseudoaneurysm/AV fistula); watch for and treat REPERFUSION/COMPARTMENT SYNDROME (fasciotomy). Prevention is key - assess pulses/PAD preoperatively, use the tourniquet judiciously, place acetabular screws in safe quadrants, and protect the popliteal vessels during posterior knee work.
- “Vascular injury in arthroplasty = rare but limb/life-threatening. TKA: POPLITEAL artery (posterior) - direct laceration AND tourniquet-related thrombosis in PAD/calcified vessels; anatomic variants (high bifurcation, aberrant ATA) increase risk.
- “THA: external iliac/femoral - ACETABULAR SCREWS in the ANTERIOR quadrants are dangerous (place in POSTERIOR quadrants); also retractors (corona mortis), cement, revision.
- “ACUTE (ischaemia/haemorrhage, absent pulse) or DELAYED (pseudoaneurysm/AV fistula weeks-years later). URGENT vascular surgery + CTA; repair/bypass/endovascular (covered stent); watch compartment syndrome. PREVENT: assess PAD, judicious tourniquet, safe screw quadrants.
TKA: popliteal artery (posterior) - laceration + tourniquet/PAD thrombosis; THA: external iliac/femoral - anterior acetabular screw quadrants are dangerous (use posterior quadrants).
Acute (ischaemia/haemorrhage/absent pulse) or delayed (pseudoaneurysm/AV fistula). Urgent vascular surgery + CTA; repair/bypass/endovascular; watch compartment syndrome.
At-Risk Vessels, Mechanisms & Risk Factors
Vascular injury is a rare but limb- and life-threatening arthroplasty complication. In TKA the popliteal artery (just posterior to the knee) is at risk - from direct laceration (posterior capsular work, osteophyte excision, posterior retractor) and from tourniquet-related thrombosis/embolism in patients with peripheral arterial disease or a calcified popliteal artery; anatomic variants (high popliteal bifurcation, aberrant anterior tibial artery) increase the risk, especially in women. In THA the external iliac/common femoral/profunda vessels are at risk - classically from acetabular screws placed in the dangerous anterior quadrants (place screws in the safe posterior quadrants), and also from retractors (corona mortis), cement extrusion and revision/protrusio surgery. Presentation is acute (haemorrhage, absent pulse, ischaemia, expanding haematoma) or delayed (pseudoaneurysm or AV fistula weeks to years later); a tourniquet can mask bleeding until released, so check perfusion after deflation.
- Total knee arthroplasty
- Popliteal artery (posterior)
- Total hip arthroplasty
- External iliac / common femoral / profunda
- Total knee arthroplasty
- Direct laceration (posterior work), tourniquet thrombosis in PAD, retractor
- Total hip arthroplasty
- Acetabular screws (anterior quadrants), retractor (corona mortis), cement, revision
- Total knee arthroplasty
- PAD / calcified vessels, anatomic variants (high bifurcation, aberrant ATA)
- Total hip arthroplasty
- Intrapelvic components, protrusio, revision, anterior screw placement
- Total knee arthroplasty
- Assess PAD/pulses, judicious tourniquet, protect popliteal in posterior work
- Total hip arthroplasty
- Place screws in posterior (safe) quadrants; careful retractor placement
Presentation & Management
- Recognise acute injury: intra-operative/early haemorrhage, an absent or diminished distal pulse, a pale, cool, ischaemic limb, or an expanding haematoma; check limb perfusion AFTER tourniquet deflation.
- Recognise delayed injury: a pseudoaneurysm or arteriovenous fistula presenting weeks to years later with swelling, a pulsatile mass, a bruit/thrill, or distal ischaemia.
- Investigate and act urgently: involve VASCULAR SURGERY immediately; obtain CT ANGIOGRAPHY (or on-table angiography) unless the limb is critically ischaemic and needs immediate exploration.
- Treat: direct REPAIR or BYPASS, or ENDOVASCULAR treatment (a covered stent - particularly effective for pseudoaneurysm and AV fistula); watch for and treat REPERFUSION/COMPARTMENT SYNDROME with fasciotomy.
- Prevent: preoperative assessment of pulses/PAD (and revascularisation first if needed), judicious tourniquet use, safe (posterior) acetabular screw quadrants, careful retractor placement, and awareness of anatomic variants.
The two errors to avoid with vascular injury in arthroplasty are missing it and delaying treatment. Because it is rare, a pulseless, pale or painful limb, an expanding haematoma, or unexplained ongoing bleeding after a hip or knee replacement must be treated as a vascular emergency - with urgent vascular surgery involvement and CT angiography (or immediate exploration if critically ischaemic) - not attributed to positioning or a 'cold leg'. A tourniquet can mask intra-operative bleeding until it is released and can itself cause popliteal thrombosis in a patient with peripheral arterial disease, so perfusion must be checked after deflation and PAD assessed beforehand. Delayed presentations as a pseudoaneurysm or arteriovenous fistula occur weeks to years later, so a new pulsatile mass, bruit or distal ischaemia around a replaced joint warrants imaging. Prevention - assessing the vascular status, using the tourniquet judiciously, and placing acetabular screws in the safe posterior quadrants - is far better than managing the catastrophe.
The Acetabular Screw Quadrant System (Wasielewski)
- Constructing the quadrants. Draw a line from the anterior superior iliac spine through the centre of the acetabulum to the posterior fovea; then a second line perpendicular to it at the acetabular centre. This divides the acetabulum into four quadrants: anterosuperior, anteroinferior, posterosuperior and posteroinferior.
- What lies behind each. Anterosuperior - the external iliac artery and vein (the most dangerous; screws here can be catastrophic). Anteroinferior - the obturator artery, vein and nerve. Posterosuperior - the sciatic nerve and superior gluteal vessels/nerve. Posteroinferior - the sciatic nerve, inferior gluteal and internal pudendal vessels.
- The rule. Place acetabular screws in the POSTERIOR (posterosuperior and posteroinferior) quadrants, which have both the best bone stock AND the safest depth; the posterosuperior quadrant is the preferred primary screw zone. Avoid the anterior quadrants, where the external iliac and obturator vessels lie a short distance from a screw tip that perforates the medial wall.
- Practical caveats. Keep screws short and angled to avoid intrapelvic penetration; in revision/protrusio or dysplastic anatomy the landmarks shift, so a preoperative CT and a low threshold for navigation help - and revision is also the one factor measured to raise arterial-injury risk. Nerve-specific injury in hip replacement is developed in neurovascular injury in total hip arthroplasty.
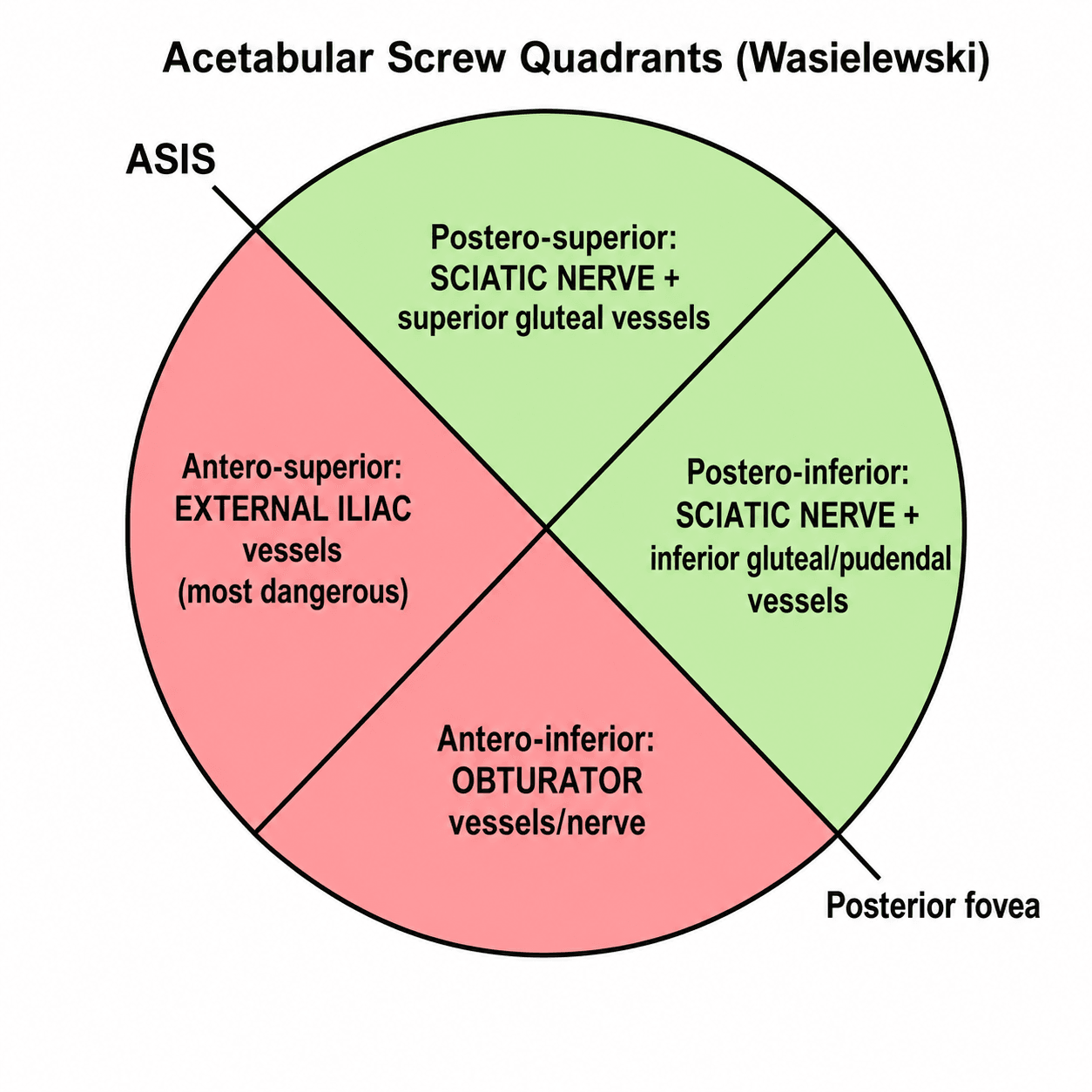
Wasielewski quadrants: a line from the ASIS through the acetabular centre to the posterior fovea, plus a perpendicular, makes four zones. Anterosuperior = external iliac vessels (most dangerous); anteroinferior = obturator; posterior two = sciatic/gluteal/pudendal. Put screws in the posterior (esp posterosuperior) quadrants - best bone, safest - and never the anterior quadrants.
Screening the At-Risk Patient & the Tourniquet Decision
- Preoperative vascular screening. Palpate the distal pulses, ask about claudication/rest pain, and look for signs of peripheral arterial disease (hair loss, trophic skin, prior bypass scars); heavily calcified vessels on the plain radiograph are a red flag. Where pulses are absent or PAD is suspected, obtain an ankle-brachial index and arterial duplex / CT angiography and get a vascular surgery opinion - and revascularise first if there is significant occlusive disease, deferring the elective arthroplasty.
- The tourniquet decision in TKA. A tourniquet in a limb with PAD, a heavily calcified popliteal artery or a previous arterial bypass graft risks plaque disruption, thrombosis or graft occlusion - so in these patients avoid the tourniquet (or use it without forcible exsanguination, at a lower cuff pressure, for the shortest time). A tourniquet over a bypass graft or a severely calcified vessel is effectively contraindicated.
- Check perfusion at the end. Because a tourniquet can mask arterial injury and bleeding until released, document the distal pulses and limb perfusion after deflation (and before leaving theatre) - a newly pulseless or ischaemic foot is a vascular emergency, not a "cold leg".
- Keep checking after theatre. Deflation is the first check, not the last: in the largest series nearly half the arterial injuries declared after the day of surgery, and roughly a quarter after the first postoperative week - so distal perfusion belongs on the daily ward round, and a new pulse deficit, disproportionate pain or a falling haemoglobin days later should be imaged.
General tourniquet physiology and complications are developed in tourniquet use.
Prevent it: examine the pulses and screen for PAD (claudication, calcified vessels on the radiograph, a reduced ankle-brachial index → duplex/CTA + vascular opinion, revascularise first). In PAD or a heavily calcified/bypassed limb avoid the tourniquet (it can thrombose the vessel or occlude a graft), and always re-check perfusion after deflation before leaving theatre.
How Rare, in Whom, and When Does It Declare Itself
"Rare but devastating" is true and unhelpful at the bedside. The numbers change three things: how hard to look, whom to look at hardest, and for how long.
In a prospectively collected multi-institutional dataset of 41,633 arthroplasties, arterial injury occurred in 34 patients - 0.08 percent overall. Broken down: 0.08 percent primary TKA, 0.04 percent primary THA, and 0.19 percent revision TKA and 0.20 percent revision THA. A single high-volume community system separately found 13 vascular complications in 9,951 knees (0.13 percent), consistent with the pooled picture. So roughly one in a thousand or fewer, but the figure roughly doubles to trebles with revision surgery.
On logistic regression the significant predictor was a redo (revision) procedure - odds ratio 2.7 (95 percent CI 1.2 to 6.0). That is the measured risk factor, and it maps onto the mechanisms already known: scarred planes, distorted anatomy, intrapelvic components and longer retraction. Demographic associations were also reported - African American race with an odds ratio of 2.5, and in the single-centre series a striking relative risk in Black women - but these rest on 34 and 13 events respectively, are unadjusted for comorbidity, vascular disease burden and access to preoperative vascular assessment, and must not be read as biological risk. Treat them as a prompt to examine every patient's vessels properly, not as a patient category.
Of the 34 arterial injuries in that dataset, 18 were repaired on the day of the index operation, 8 between postoperative days 1 and 5, and 8 between days 6 and 30. Almost half therefore became apparent after the patient left theatre, and nearly a quarter after the first postoperative week. Documenting pulses once after tourniquet deflation is necessary but not sufficient - distal perfusion belongs on the daily postoperative check, and a new pulse deficit, disproportionate pain, an expanding haematoma or a falling haemoglobin days after an uneventful arthroplasty warrants imaging rather than reassurance. Where injuries were detected early and repaired, limb salvage was excellent: only 2 of the 34 (5.9 percent) came to amputation.
Carry the numbers: about 0.08 percent overall, 0.04 percent primary THA, 0.08 percent primary TKA, and near 0.2 percent for either revision; revision is the measured predictor (odds ratio 2.7); only about half present on the day of surgery; and with early detection and repair limb loss was 5.9 percent of those injured - the catastrophic outcomes follow delay, not the injury itself.
Mnemonics & Memory Aids
VESSEL
Hook:VESSEL: Vessels (popliteal/iliac-femoral), Emergency (vascular surgery+CTA), Screws posterior, Suspect tourniquet thrombosis, Endovascular for pseudoaneurysm/AVF, Look out for compartment syndrome.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Which vessels are at risk in knee and hip arthroplasty, and by what mechanisms?”
“How would you manage a suspected vascular injury after a knee replacement?”
TKA
- Popliteal artery (posterior to the knee) at risk
- Mechanisms: direct laceration (posterior work), tourniquet thrombosis in PAD/calcified vessels
- Anatomic variants (high bifurcation, aberrant ATA) increase risk (esp. women)
THA
- External iliac / common femoral / profunda at risk
- Acetabular screws: anterior quadrants dangerous -> place in POSTERIOR (safe) quadrants
- Also: retractor (corona mortis), cement extrusion, revision/protrusio
Presentation
- Acute: haemorrhage, absent pulse, ischaemic limb, expanding haematoma (check after tourniquet deflation)
- About HALF declare after the day of surgery (8 of 34 on days 1-5, 8 on days 6-30) - keep checking pulses on the ward round
- Delayed: pseudoaneurysm or AV fistula (weeks-years later)
- Incidence 0.08% overall; ~0.2% in revision (OR 2.7); limb loss 5.9% of those injured with early repair
Management & prevention
- Urgent vascular surgery + CT angiography (or immediate exploration if critically ischaemic)
- Repair/bypass or endovascular (covered stent); watch/treat compartment syndrome (fasciotomy)
- Prevent: assess PAD/pulses, judicious tourniquet, safe screw quadrants, know variants
Evidence & Key Studies
Popliteal artery injury risk in TKA related to anatomic variations (scoping review)
- Popliteal artery injury during TKA is rare but can be devastating - leading to repair/bypass, limb ischaemia, compartment syndrome, fasciotomy, amputation or death.
- Anatomical variations such as a high popliteal bifurcation or an aberrant anterior tibial artery (aberrant ATA prevalence about 0.4-6%, ~3.2% on one MRI study) elevate the risk, with proximity to landmarks increasing injury risk especially in women.
- Awareness of anatomical variation, review of pre-existing MRI and selective vascular imaging may improve surgical planning and mitigate complications.
Popliteal arteriovenous fistula diagnosed years after TKA, treated endovascularly
- Iatrogenic vascular lesions are rare in orthopaedic surgery but carry significant consequences, and the knee is particularly susceptible.
- A popliteal arteriovenous fistula was diagnosed eight years after a total knee arthroplasty and treated successfully with an endovascular covered stent (Viabahn), patent at five-year follow-up.
- Both pseudoaneurysms and arteriovenous fistulae should be considered as delayed presentations, and endovascular treatment is effective.
Predictors of lower-extremity arterial injury after knee or hip arthroplasty: 41,633 procedures
- Prospectively collected NSQIP data from Veterans Affairs centres, 1996 to 2003: 41,633 arthroplasties (24,029 primary TKA, 2,077 revision TKA, 13,494 primary THA, 2,033 revision THA).
- 34 arterial injuries (0.08 percent overall): 0.08 percent primary TKA, 0.19 percent revision TKA, 0.04 percent primary THA, 0.20 percent revision THA - revision roughly doubles to trebles the rate.
- TIMING: 18 repaired on the day of surgery, 8 on postoperative days 1 to 5, and 8 on days 6 to 30 - nearly half declared after the day of operation.
- Only 2 patients required amputation, a limb-loss rate of 5.9 percent among those injured; the authors attribute this to close surveillance and early repair.
- Independent predictors were a redo procedure (OR 2.7, 95 percent CI 1.2 to 6.0) and African American race (OR 2.5, 95 percent CI 1.2 to 5.3).
- A predominantly male veteran population with 34 events in total, unadjusted for peripheral arterial disease burden - the demographic association in particular should not be read as biological risk.
Vascular complications after TKA in a high-volume community system: 13 in 9,951 knees
- 13 vascular complications in 9,951 total knee arthroplasties (0.13 percent), 2010 to 2014, identified by cross-referencing billing and diagnosis codes.
- 12 of the 13 were diagnosed and treated on the same day as the index arthroplasty; treatment was endovascular in most (9 stents, 2 endarterectomies, 1 thrombectomy, 1 bypass).
- There were NO amputations, no compartment syndrome, no periprosthetic joint infection and no mortality - but 3 patients had persistent stiffness needing manipulation and 1 sustained a peroneal nerve injury.
- Only 4 of the 13 had vascular calcification visible on the preoperative radiograph, so a clean radiograph does not exclude the at-risk vessel.
- 13 events in a single system: the reported demographic risk ratios rest on very small numbers and are hypothesis-generating.
The rarity-but-severity of popliteal artery injury in TKA (repair/bypass, ischaemia, compartment syndrome, fasciotomy, amputation, death), the role of anatomic variants (high popliteal bifurcation, aberrant anterior tibial artery) in elevating risk - especially in women - and the value of preoperative awareness and selective imaging come from the cited Parekh scoping review; the delayed presentation as a pseudoaneurysm/arteriovenous fistula years after TKA and the effectiveness of endovascular (covered-stent) treatment from the cited Lozano-Sanchez report. The THA acetabular-screw 'quadrant' safe zones, the tourniquet/peripheral-arterial-disease mechanism, and the urgent CT-angiography-plus-vascular-surgery management are standard, well-established teaching. The incidence figures, the revision odds ratio and the timing distribution come from the cited Abularrage analysis of NSQIP data - a predominantly male veteran population with only 34 events, and one that predates much contemporary practice; the single-system knee figures and the observation that most vessels had no visible calcification preoperatively from the cited Padegimas series of 13 events. Both report demographic associations which are stated here only to be set aside: with 34 and 13 events respectively, unadjusted for vascular disease burden or access to preoperative assessment, they do not support any biological claim. No randomised evidence exists for any preventive strategy in this complication, and no validated risk score, safe tourniquet pressure or screening threshold specific to arthroplasty was retrieved, so none is quoted. See also neurovascular injury in total hip arthroplasty, neurovascular injury in total knee arthroplasty, tourniquet use and compartment syndrome.